Article Text

Abstract
Background Extension of retinoblastoma cells into the posterior chamber is a criterion for group E according to the international classification of intraocular retinoblastoma. Currently, the anterior extension of retinoblastoma is based on the presence of tumour cells in the anterior chamber assessed by biomicroscopy.
Aim To determine the value of ultrasound biomicroscopy (UBM) in the assessment of posterior chamber involvement in advanced retinoblastoma.
Methods Retrospective review of all retinoblastoma cases enucleated at the Jules Gonin Eye Hospital from January 1996 to December 2009 for which UBM (35 MHz) evaluation was available. The patients' records were reviewed for patient and tumour features and histopathological findings. UBM findings were compared with histopathological features.
Results UBM documentation was available in 31 cases. Retinoblastoma was detected by UBM in the posterior chamber in 18 cases and was absent in 13 cases while histopathological analysis demonstrated its presence in the posterior chamber in 22 cases and its absence in 9 cases. Among the 18 UBM-positive cases, 7 had biomicroscopic detectable involvement of the anterior chamber. There was a significant correlation between echodensities consistent with retinoblastoma on UBM in the posterior chamber and histopathological tumorous involvement of the posterior chamber (p=0.0001). The sensitivity of UBM in the assessment of posterior chamber invasion by retinoblastoma was 81% and the specificity was 100%.
Conclusion In selected cases of advanced retinoblastoma, UBM appears to represent a valuable tool in the precise evaluation of anterior extension of disease, with good sensitivity and specificity for the assessment of posterior chamber involvement. UBM may provide useful criteria governing the indication for enucleation.
- Pathology
- retinoblastoma
- ultrasound biomicroscopy
- neoplasia
- imaging
- diagnostic tests/investigation
Statistics from Altmetric.com
Introduction
The precise delineation of tumour extension is important in the management of patients with retinoblastoma. More specifically, extension of retinoblastoma cells anterior to the vitreous surface is a criterion used to categorise retinoblastoma in group E.1 In retinoblastoma with peripheral retinal involvement, the assessment of tumour invasion of the posterior chamber remains uncertain in the absence of detectable retinoblastoma cells in the anterior chamber by slit lamp. In these circumstances, CT, MRI or conventional ultrasound is of limited value.
Ultrasound biomicroscopy (UBM) yields high-resolution images of the anterior segment and structures hidden from clinical visualisation, such as the ciliary body, zonule or posterior chamber.2 This technique, developed in Canada in the 1990s, uses high-frequency continuous wave transducers (50 MHz) incorporated into a B-scan device with an axial and lateral resolution of 50 μm and a tissue penetration of 4–5 mm.3 UBM has enabled better assessment of anterior segment tumour extension4–6 and has been used in several studies in the management of iris or ciliary body melanoma, with good clinicopathological correlation.7 8 In a recent prospective study of 18 anterior segment tumours comparing the use of UBM and anterior segment optical coherence tomography, UBM was found to be more flexible due its ability to penetrate lesions up to 5 mm thick or heavily pigmented tumours.9
There are only a few reports documenting the use of UBM in paediatric ocular oncology.6 10–12 This prompted us to examine the value of UBM in the assessment of posterior and anterior chamber involvement in cases of peripheral extension of retinoblastoma.
Patients and methods
A retrospective chart review was undertaken in all patients who underwent enucleation at the Jules Gonin Eye Hospital Paediatric Oncology Unit from January 1996 to December 2009. The study was approved by the Institutional Review Board of Lausanne University. The study adhered to the tenets of the Helsinki Declaration. Patients for whom ultrasound biomicroscopic documentation of disease extension was available were selected for the study. For each patient, information regarding age, sex, primary or secondary tumour and tumour laterality was retrieved. Anterior segment findings including the presence of anterior inflammation were recorded.
The UBM device used in this study was the commercially available OTI Scan 2000 (Ophthalmic Technologies, North York, Ontario, Canada) with 35 MHz transducers. The acoustic axial resolution of UBM at 35 MHz is 68 μm. UBM testing was performed by the same examiner (FLM) in all cases using an eyecup filled with methylcellulose and 0.9% water medium, under general anaesthesia. Longitudinal scans were obtained along each meridian circumferentially. Maximal tumour thickness and diameter as well as the presence of abnormal echodensities consistent with retinoblastoma in the posterior or anterior chamber were noted in each case.
UBM results were compared with the histopathological data in each case. Formalin-fixed enucleated eyes were routinely processed, paraffin embedded and serially sectioned with a mean of 50 sections/case. H&E staining was performed on all sections. Histopathological analysis included the number of primary tumours, largest tumour diameter, growth pattern, tumour differentiation, presence of calcification, tumour necrosis and precise tumorous involvement of the different ocular structures (Schlemm's canal, anterior chamber, posterior chamber, ciliary body, vitreous, retina, choroid, sclera and optic nerve). The international classification for intraocular retinoblastoma1 and TNM13 was used for grouping each eye at presentation. In the recent TNM classification,13 extension of retinoblastoma in the anterior segment defines severe intraocular disease (T3b); however, posterior chamber invasion is not specifically mentioned in this classification.
Statistical analysis was performed using JUMP 8.0 software (SAS). Fischer's exact test was used to test for statistically significant association between unpaired data.
Results
From January 1996 to December 2009, 149 enucleations for retinoblastoma were performed in our institution. UBM information was retrieved in 31 cases. There were 15 men and 16 women. The mean age at diagnosis was 5.3 years. There were 21 primary enucleations and 10 secondary enucleations. Retinoblastoma was unilateral in 24 patients and bilateral in 7. Anterior chamber involvement was clinically identified by slit lamp examination in seven cases.
UBM and histopathological features of anatomical landmarks of the posterior chamber in the absence of retinoblastoma are illustrated in figure 1. The results of UBM and histopathological findings are shown in table 1.

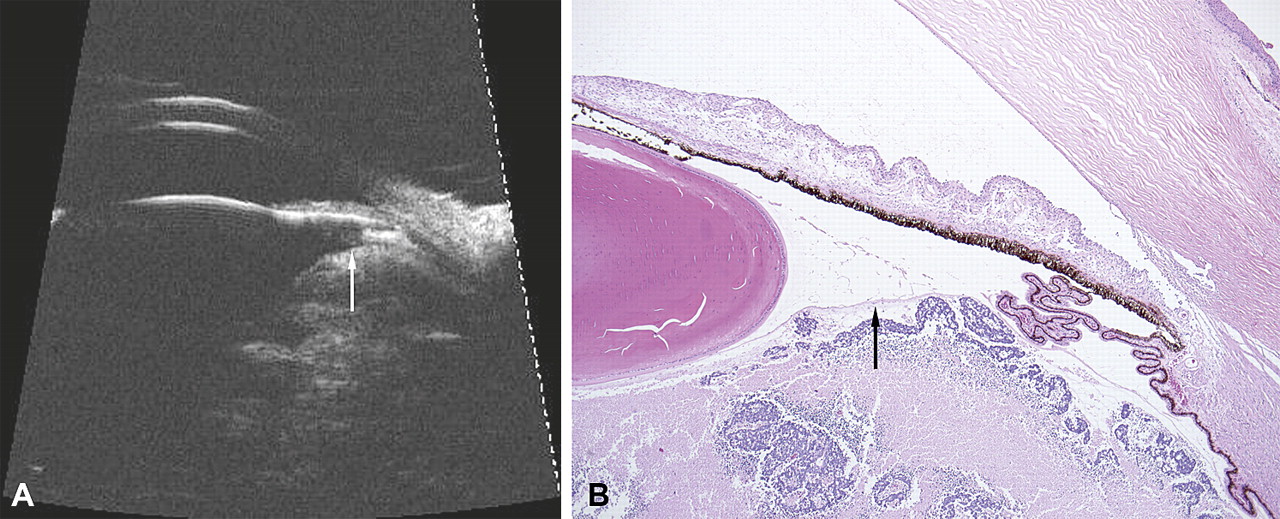
Clinicopathological correlation in the absence of invasion of the posterior chamber. (A) In this untreated case, a ciliary process underneath the iris is clearly visible by ultrasound biomicroscopy (UBM). (B) The anterior hyaloid (arrow), normally difficult to detect with UBM, is identifiable posterior to the ciliary process. There is no invasion of the posterior chamber ultrasonographically and histopathologically. A large area of necrosis can be observed behind aggregates of viable retinoblastoma cells posterior to the hyaloid. UBM, 35 MHz; pathological slide; stain, H&E; original magnification, ×26.
35 MHz ultrasound imaging and histopathological findings
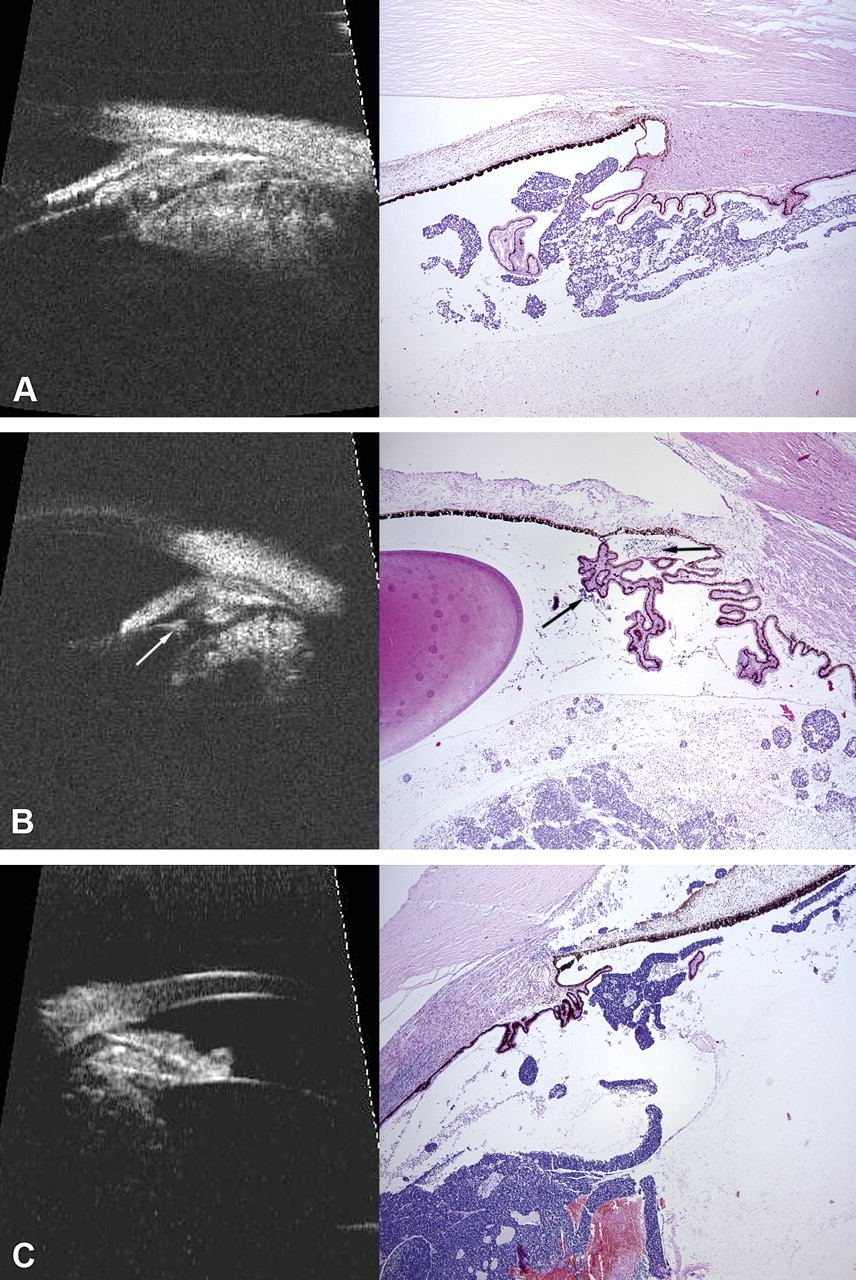
UBM enabled the correct assessment of posterior chamber invasion in 27 cases (18 cases positive for retinoblastoma in the posterior chamber and 9 cases negative). Examples of clinicopathological correlations are highlighted in figure 2. There was a significant correlation between echodensities on UBM, which was consistent with retinoblastoma in the posterior chamber and the histopathological confirmation of posterior chamber involvement (p=0.0001). The sensitivity of UBM in the assessment of posterior chamber invasion by retinoblastoma was 81% and the specificity was 100%. There were four cases where UBM failed to detect the presence of retinoblastoma cells in the posterior chamber. In these cases, there were very small aggregates of retinoblastoma cells with a mean diameter of 150 μm floating in the posterior chamber. These aggregates were only identified in one or two histopathological sections (ie, in <2.3% of all the sections performed in each case).
{kind=link}
{kind=link}
Correlation between ultrasound biomicroscopy (UBM) findings and pathological findings in the evaluation of the posterior chamber. In (A) and (C), there is a massive invasion of the posterior chamber by retinoblastoma detected ultrasonographically and confirmed histopathologically. In (C), invasion of the anterior chamber is also visible. (B) In the posterior chamber, UBM demonstrates an abnormal hyper-reflectivity (white arrow) that corresponds to the presence of retinoblastoma (oblique black arrow). Clusters of retinoblastoma cells can also be observed anterior to ciliary processes (horizontal black arrow). UBM, 35 MHz; pathological slides; stain, H&E; original magnification, ×26.
There were eight primary enucleations where UBM correctly identified the presence of retinoblastoma cells in the posterior chamber in the absence of invasion of the anterior chamber. Among these cases, all were correctly assigned to group E (or T3) without the use of UBM, except in one case clinically classified as group D (or T2a) according to the presence of a massive vitreous seeding arising from a purely endophytic anterior tumour with no optic nerve and/or macular involvement. This eye was finally reassigned to group E based on the UBM detection of suspicious echodensities in the posterior chamber, which were later confirmed to correlate histopathologically with retinoblastoma involvement.
Discussion
Retinoblastoma with peripheral retinal involvement may extend into the posterior chamber and ultimately progress into the anterior chamber. Involvement of the anterior segment clearly requires rupture of the anterior hyaloid, an established enucleation criterion according to the international classification of intraocular retinoblastoma (group E). However, the clinical status of the anterior hyaloid cannot be unequivocally determined in the absence of a full evaluation of the posterior chamber. The posterior segment up to the ora serrata can be visualised by fundoscopy or conventional ultrasound, but these modalities appear to be of limited value in the assessment of disease anterior to the ora serrata. In this context, we examined the value of UBM in the detection of posterior chamber involvement and correlated all cases with histopathological evaluation.
It is essential to correctly interpret the normal features of UBM in children in order to distinguish them from those relating to retinoblastoma. The ciliary processes are long in children and may be confused with tumours, but their linear aspect can easily be detected by rotation of the UBM device. In a normal situation, the vitreous base shows moderate and homogenous reflectivity with UBM, whereas tumour seeding and infiltration of the vitreous base by retinoblastoma show a slightly increased reflectivity of irregular shape and distribution.
In the posterior chamber, UBM allows correct evaluation of this anatomical area in 87% of the cases, and we identified a significant correlation between UBM findings and histopathological documentation of posterior chamber invasion by retinoblastoma. There were only four cases where UBM failed to detect small aggregates of retinoblastoma cells in the posterior chamber. Histopathology showed that these aggregates had a mean diameter of 150 μm. These cells were probably undetected due to the limited number of UBM scans, preventing precise documentation of these very small areas of the posterior chamber. On the other hand, it cannot be completely ruled out that these small clusters of cells may represent a spillover from the main tumour during macroscopic evaluation and section of the globe.
In borderline situations, the correct distinction between group D and E eyes is critical, especially with the advent of novel therapeutical tools for advanced retinoblastoma such as superselective ophthalmic artery chemotherapy. Among the eight primary enucleations without clinical evidence of retinoblastoma in the anterior chamber in our study, the distinction between group D or E was UBM dependent in one case. In a recent study from Canada,13 11 cases were enucleated with UBM demonstrating retinoblastoma extension anterior to the ora serrata and excellent clinicopathological correlation.
The presence of retinoblastoma cells in the posterior chamber with and without visible tumorous involvement of the anterior chamber most likely carries the same prognostic value. In this context, UBM appears to represent a valuable tool in the precise evaluation of disease extension in selected cases of advanced retinoblastoma, in particular posterior chamber assessment in the absence of biomicroscopic involvement of the anterior chamber. Although our series includes only a limited number of cases, the sensitivity and specificity of UBM in the assessment of anterior extension of retinoblastoma provides useful information for therapeutic decision-making.
References
Footnotes
Presented in part at The Annual Meeting of the Association for Research in Vision and Ophthalmology, May 2010, session 2075, A15, Fort Lauderdale, Florida, USA.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.