Article Text

Abstract
Objective Tumour necrosis factor (TNF) blockers have been demonstrated to be effective in the treatment of systemic and ocular inflammatory diseases. We conducted a prospective, multicentre, open-label Phase II clinical trial to assess the effectiveness and safety of adalimumab, a fully human anti-TNF monoclonal antibody, in treating refractory uveitis.
Methods Subjects with non-infectious uveitis refractory to corticosteroids and at least one other immunosuppressive medication were enrolled. Treatment outcome was ascertained by a composite endpoint comprised of visual acuity, intraocular inflammation, ability to taper immunosuppressives, and posterior segment imaging. Clinical response was defined by improvement in at least one parameter, worsening in none, and well controlled intraocular inflammation. Week 10 responders were permitted to continue receiving adalimumab for the study duration of 50 weeks.
Results Twenty-one of 31 patients (68%) were characterised as clinical responders at 10 weeks, of whom 12 patients (39%) exhibited durable response after 50 weeks. The most common reason for study termination was primary or secondary inefficacy. No patients experienced treatment-limiting toxicity clearly related to study therapy.
Conclusions Adalimumab was safe and effective in 68% of refractory uveitis patients 10 weeks after study enrolment, and maintained in 39% after 1 year. Ongoing study is required to determine the place of adalimumab and other TNF blockers in the treatment of uveitis.
- Clinical Trial
- Immunology
- Inflammation
- Treatment Medical
- Epidemiology
Statistics from Altmetric.com
The term, uveitis, describes a heterogeneous group of diseases characterised by inflammation of intraocular structures. Epidemiologic studies indicate the prevalence of uveitis to be between 70 and 110 cases per 100 000 persons.1 ,2 Despite its relative uncommonness, uveitis accounts for 2–10% of prevalent blindness in European and North American population-based series, and is a significant public health problem.3 Non-infectious uveitides are thought to represent cell-mediated autoimmunity,4 ,5 providing the rationale for immunosuppressive treatment. Corticosteroids improve the signs and symptoms of ocular inflammation, as well as the prognosis for vision preservation.6 The well-known side effects of chronic corticosteroid therapy have led ophthalmologists to employ corticosteroid-sparing agents; however, these agents also may cause undesirable toxicity.7 Efforts, therefore, continue to identify more effective, targeted therapies.
Recently, the search for new treatments has focused on biologic response modifiers (BRMs), which are therapeutic agents bioengineered to block specific immunologic mediators.8 Tumour necrosis factor (TNF) blockers have been the most commonly employed and successful BRMs. Animal and human studies substantiate that TNFα is an important mediator in uveitis.9 ,10
Adalimumab is a fully human monoclonal IgG1κ antibody against TNFα, which binds both circulating and cell-surface cytokine. At our study inception, it was one of three commercially available TNF blockers, along with the fusion protein etanercept (Enbrel; Amgen) and the chimeric murine-human monoclonal antibody, infliximab (Remicade; Centocor). At that time, most published research on TNF blockers in uveitis involved infliximab and etanercept, though adalimumab had been reported effective in smaller case series in children.11 ,12 Our group reported the results of a prospective clinical trial of infliximab, which revealed good efficacy but unexpected toxicity.13 ,14 Two retrospective studies comparing infliximab to etanercept suggested superior efficacy of monoclonal antibody therapy with infliximab.15 ,16
In theory, adalimumab offers the efficacy of a monoclonal antibody with the convenience of subcutaneous injection, potentially with less likelihood of neutralising antibodies. We therefore sought to perform a prospective multicentre clinical trial to assess the safety and efficacy of adalimumab for the treatment of refractory non-infectious uveitis.
Methods
Enrolment criteria and study screening
All patients were recruited from the tertiary referral clinics of Oregon Health & Science University, Cleveland Clinic Foundation, and University of Illinois-Chicago between February 2008 and September 2009, after respective institutional review board approvals. Prior to enrolment, all patients received complete ophthalmic and systemic evaluations. Patients were required to be at least 18 years old and have vision-threatening uveitis refractory to therapy with corticosteroids, and at least one other immunosuppressive, or to be intolerant of such therapy. Refractory disease was defined by the presence of persistent inflammation despite treatment with a given immunosuppressive and/or inability to taper corticosteroids under cover of the indicated immunosuppressive drug.
All patients were required to have a Protein Purified Derivative (PPD) skin test and chest x-ray within 3 months of enrolment. Patients with latent tuberculosis (positive PPD without radiographic or clinical evidence of pulmonary or disseminated tuberculosis) were enrolled only if they agreed to undergo concomitant chemoprophylaxis with antituberculosis therapy due to the risk of tuberculosis reactivation with TNF inhibition.17 All patients received a fluorescein angiogram (FA) and ocular coherence tomography (OCT) at enrolment, week 10 and week 50. PPD was repeated at weeks 26 and 50. All patients with pars planitis were required to undergo neuroimaging to rule out demyelinating disease, given the association between pars planitis and multiple sclerosis,18 and previous studies indicating that TNF blockade may worsen demyelinating disease.19
Treatment protocol
Enrolled patients received adalimumab 40 mg subcutaneous injections every 2 weeks, which was provided gratis by Abbott (Chicago, Illinois, USA). The first injection was investigator-administered; the second was patient-administered and physician-supervised. All subsequent injections were patient-administered. Study visits occurred at baseline, weeks 2, 6 and 10. Positive clinical responders to adalimumab at week 10 were eligible to continue receiving study therapy for the complete 50-week study period, and were seen every 8 weeks thereafter. Non-responders were terminated from the study. Additional visits were allowed on an ad hoc basis.
Ophthalmic evaluation
Ophthalmic evaluation included best-corrected visual acuity measured utilising standard Early Treatment of Diabetic Retinopathy Standard (ETDRS) protocols at all primary outcome-measurement study visits (weeks 0, 10 and 50), and best-corrected Snellen chart-measured acuities at other visits. Intraocular pressure measurement, biomicroscopy and dilated indirect ophthalmoscopy was performed at all study visits. Anterior chamber cell and vitreous haze were graded by Standardisation of Uveitis Nomenclature (SUN) Working group criteria.20 Specific notation of the presence or absence of cystoid macular oedema, active retinal vasculitis and active chorioretinitis was made.
Systemic evaluation and laboratory monitoring
Patients had a general physical examination at each visit and were specifically queried about the occurrence of possible drug-related adverse events. Laboratory evaluations were performed at the outset and conclusion of the study and included metabolic panel, liver function tests, complete blood count and antinuclear antibody (ANA) titres, and on an ad hoc basis as needed. Patients on concomitant immunosuppression continued to be monitored as indicated for their concomitant therapy. Patients were queried about compliance at each visit and returned used syringes to the investigators for verification of compliance.
Outcome variables and definitions of composite clinical endpoint
The primary outcome variable was a composite endpoint with four parts, as described in our earlier study13: visual acuity, inflammatory control, medication tapering and reduction of inflammatory signs by FA and OCT. As in our previous study, patients were required to improve in at least one of the four subendpoints, to worsen in none, and to have well controlled intraocular inflammation to be characterised as a treatment success.
The four components of our composite clinical endpoint each were graded dichotomously (yes or no) for success. To be defined as a success for visual acuity, a subject had to have an improvement of at least two Snellen chart lines in at least one eye from baseline. Conversely, criteria for worsening visual acuity were loss of two lines in at least one eye. Intraocular inflammation was considered active or uncontrolled if anterior chamber cells or vitreous haze was 1+ or greater by SUN standardised grading, and adalimumab was defined as successful in controlling inflammation when patients with active disease at study outset achieved clinical quiescence (zero or trace anterior chamber or vitreous inflammation). Adalimumab was deemed an effective concomitant immunosuppressive-sparing agent if the dose of prednisone or other immunosuppressive drug could be reduced by ≥50% without inflammation reactivation. In general, prednisone was tapered first unless it was medically necessary to first taper another concomitant immunosuppressive due to drug-related toxicity. Improvement in FA required reduction in cystoid macular edema (CME) and other signs of inflammation as graded by a masked investigator (AKL) using a standardised grading form as described previously.13 ,14 Improvement in macular oedema as measured by OCT was regarded as supportive to the FA studies, but was not used as a sole measure for successful grading.
Results
Demographic information on enrolled patients is summarised in table 1. Eighteen of the 31 patients (58%) enrolled were women. The age range was 20–66 years (mean and median 40.9 years). Using the SUN classification criteria,19 the most common anatomic diagnosis was panuveitis (17/31; 54.8%), followed by posterior (6/31; 19.4%), intermediate (3/31; 9.7%), anterior (3/31; 9.7%) and anterior and intermediate uveitis (2/31; 6.4%). The most commonly diagnosed aetiologies of uveitis were sarcoidosis (6/31, 19.3%), birdshot chorioretinopathy (4/31; 12.9%), Vogt–Koyanagi–Harada syndrome (3/31; 9.7%); 2 each with Behcet's, juvenile idiopathic arthritis (JIA) and seronegative spondylarthropathies, and one each with tubulointerstitial nephritis and uveitis, and pars planitis. Twelve patients (38.7%) were classified as having idiopathic uveitis. All patients had been treated previously with at least two immunosuppressive agents (range 2–6, mean 2.8).
Demographics of enrolled patients
The 10-week outcome measures are summarised in table 2. Twenty-one of 31 patients (67.7%) met a priori criteria for clinical success after 10 weeks of treatment.
Parameters defining clinical success in enrolled patients at week 10 outcome measurement
The reasons for primary study failures are summarised in table 3. Among the 10 patients not meeting criteria for success, nine were due to inability to demonstrate efficacy as measured by our composite endpoint, while one diabetic patient discontinued due to the hospitalisation with a hypoglycaemic coma which was not clearly related to adalimumab therapy.
Failures at 10-week outcome measurement
Twelve of 21 patients (57%) meeting the composite endpoint at 10 weeks had durable success and completed 1 year of study therapy, representing 39% (12/31) of the total study population. Subdivided by anatomic location of inflammation revealed statistically indistinguishable success rates in each of the four SUN categories (anterior uveitis: 1 of 3; intermediate or anterior+intermediate uveitis, 1/5; posterior uveitis: 2/6; panuveitis 8/17). Among aetiologic diagnoses, no groups were large enough to make meaningful analyses. The nine patients who did not continue treatment through week 50 were classified as secondary study failures. The reasons for these secondary failures are summarised in table 4. Six ceased treatment due to breakthrough inflammation occurring between weeks 18 and 50. One was lost to follow-up at week 42, having demonstrated efficacy until that time point, but did not return for the study exit. One patient voluntarily discontinued due to subjective worsening at week 18. Another was terminated by protocol requirement due to unexpected pregnancy, but continued to receive adalimumab outside of the study at the recommendation of her obstetrician and rheumatologist due to its beneficial effect on her inflammatory eye, joint and bowel disease.
Secondary failures between 10- and 50–week outcome measurement
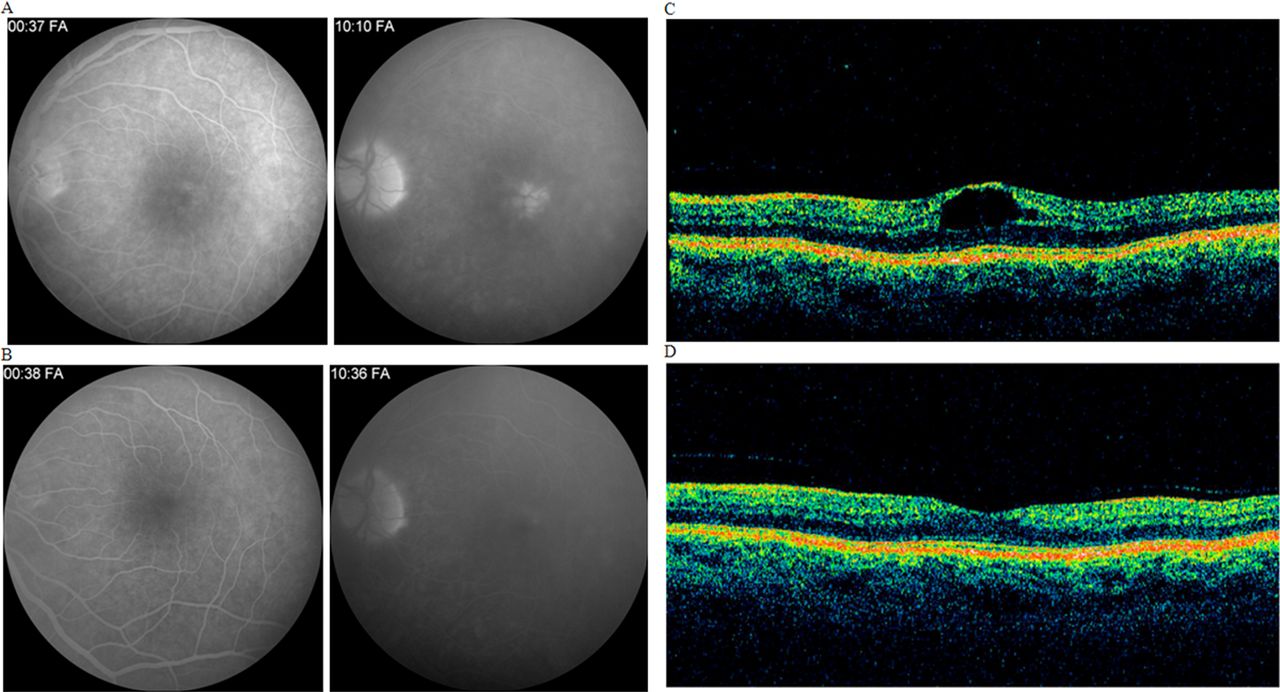
With regard to the four subcriteria of our composite endpoint, among the 12 patients meeting criteria for success at 50 weeks, six had improved visual acuity; eight enrolling with active inflammation had achieved inflammatory control; nine patients successfully reduced their corticosteroid and/or immunosuppressive dosage by 50%; and nine had improvement in their FA/OCT grading (representative images are found in figure 1).
{kind=link}
Representative clinical images demonstrating resolution of inflammatory macular oedema on fluorescein angiography (A, baseline; B, study week 10) and and ocular coherence tomography (C, baseline; D, study week 10). This figure is only reproduced in colour in the online version.
Among the nine eyes of the seven patients meeting criteria for vision improvement at week 50, improvement ranged from two to 12 lines. Three patients experienced visual deterioration on the study, two due to inflammation resulting in study discontinuation at week 10, and one due to significant worsening of cataract with the subject remaining in the study; the remainder of the patients had stable vision.
Eighteen of 31 patients (58%) had active intraocular inflammation at the outset of therapy. Within this group, 11 patients (61.1%) achieved 2-step improvement of inflammation, or complete quiescence after 10 weeks in the study, of whom eight completed the study with durable control of previously active inflammatory disease. With regard to immunosuppressive drug tapering, among the 10 subjects completing 50 weeks who entered the study on corticosteroids, average dose reduction was 90% (31–3 mg), with 9/10 reducing prednisone to <10 mg daily dose, and six patients able to discontinue corticosteroids altogether. Seven patients entered the study not taking prednisone; hence, the overall steroid-sparing effectiveness of adalimumab in this study among all participants was nine of 24 (38%).
There were no significant adverse events requiring study discontinuation that were clearly related to adalimumab usage. Self-limiting adverse events that were recorded and that did not require study discontinuation were infrequent. The most common adverse events reported were headache, common cold, joint pains and nausea. Serious adverse events included the aforementioned hypoglycaemic coma and one cerebrovascular accident which occurred a few days prior to the week 50 study completion visit. Of 15 patients with ANA testing performed at the beginning and end of the study, two (13%) developed positive ANA titres over the study period; none had clinical findings suggesting drug-related lupus.
Discussion
We report a prospective study using adalimumab to treat diverse forms of uveitis. As we have discussed previously, the innate heterogeneity of uveitis makes it a challenge to study therapeutically.7 ,13 As in our previous studies, we used a composite definition of success, which we believe parallels the disparate goals that a treating physician might have in a tertiary referral practice. Published series on the use of adalimumab in uveitis prior to our study primarily focused on paediatric populations, with excellent reported results. Biester and colleagues noted an 88% response rate (n=18) of JIA uveitis to adalimumab, though at least one patient required weekly administration to maintain clinical quiescence.11 Coban–Vazquez reported similar results, with 65.3% of 26 eyes experiencing sustained resolution of inflammation in a study of 14 paediatric uveitis patients with and without JIA.21 However, Tynjala and colleagues noted only a 35% response in 20 patients with JIA uveitis.12 Reports since the inception of our study have suggested promise for the use of adalimumab in adult uveitis. Diaz–Llopis reported that 12 of 19 patients with uveitis experienced reduction of inflammation with adalimumab treatment, with many patients experiencing reduction in CME measured by OCT. However, 42% of patients in this study had at least one recurrence over 1 year of therapy, which the authors treated with periocular steroid injections.22 In a comment on this paper, Callejas noted nearly universal initial response in 10 patients, but with 20% relapse rate over 6–24 months of follow-up.23 A multinational randomised study of adalimumab treatment for ankylosing spondylitis with uveitis as a secondary outcome noted a 45–61% reduction in uveitis flares in various strata divided by prior history and severity of anterior uveitis24; similar results have been reported for infliximab. Etanercept, in contrast, seems to be less effective in the treatment of uveitis, and has even been reported to be associated with new onset ocular inflammation.25 ,26
A common clinical question relates to where should TNF blockers or other biologics enter into the therapeutic armamentarium for treatment of uveitis, and which TNF blocker should be preferred. Dimensions of this question include concerns over cost, relative efficacy and safety. While this study does not directly compare adalimumab to infliximab, we feel that, as we have studied both drugs using a similar study design and identical outcome assessment criteria, we are able to make some interesting observations regarding these two TNF-blocking monoclonal antibodies.
Our 10- and 50-week success rates of 67% and 39% in the adalimumab study are consistent with the reported response rates reported in the Systemic Immunosuppressive Therapy for Eye Diseases (SITE) study of numerous commonly employed immunosuppressives used as monotherapy. This study employed a retrospective cohort design, found 6-month rates of inflammatory control of 66%, 62% and 73% for the antimetabolites methotrexate,27 azathioprine,8 mycophenolate mofetil,28 52% for cyclosporine29 and 76% for cyclophosphamide.30 Our study differs from these in that monotherapy with adalimumab was not required, and also in that, by protocol, multiple previously described agents had been tried unsuccessfully, presumably selecting a more refractory study population, and one perhaps with more limiting premorbid complications. The observed success rates were slightly lower than reported in our infliximab study, which reported 10- and 50-week success rates of 77% and 48%. However, the rate of treatment-limiting toxicity requiring study discontinuation was much lower in this study than in our infliximab study, in which we reported cases of drug-associated lupus, thromboembolic events and malignancy, although not all manifest toxicity was clearly related to infliximab therapy. At least two patients in the current study population demonstrated a strong efficacy signal but had to be discontinued for methodologic reasons (pregnancy and loss to follow-up at week 42), leading to their classification as failures. Subtle differences in the study designs also may have contributed to differential efficacy. Our infliximab study included loading doses and the option for dose escalation from 3 to 10 mg/kg/dose in initial responders with subsequent breakthrough inflammation; neither of which was an option in the present adalimumab study. Additionally, as a three-centre (rather than single-centre) study, differences between the study populations are possible. A currently enrolling multicentre study of adalimumab incorporating an 80 mg loading dose of adalimumab will be informative on the efficacy of this approach (see http://www.clinicaltrials.gov).
In summary, we found adalimumab to be a useful treatment for many patients with refractory uveitis, with a 10-week success rate of 68%, although relapsing inflammation reduced treatment success at 1 year to 39%, perhaps limited by the refractory nature of the population and our strict criteria for treatment success. The relative reduction in efficacy when compared with a similar study of infliximab by our group was counterbalanced by a superior outcome in terms of safety, with only two of 31 patients stopping the study due to significant adverse events, both of which were not clearly attributable to study drug therapy. Ongoing research is needed to identify ideal patient populations to receive TNF blockers generally, and adalimumab specifically, and in identifying ideal dosing regimens with regard to loading doses and ideal intervals for subsequent maintenance doses.
Acknowledgments
This work was supported by Abbott (Chicago, IL) protocol number HUM05-029. Research support was provided by the Department of Veterans’ Affairs (EBS), Research to Prevent Blindness (unrestricted grant to Casey Eye Institute and University of Illinois-Chicago, Senior Scholar Award to JTR), the Rosenfeld Family Trust (JTR), the William and Mary Bauman Foundation, and the William C Kuzell Foundation. Dr Suhler has served as a paid consultant to LuxBio. Dr Rosenbaum has served as a paid consultant to Amgen, LuxBio, Xoma, Centocor, Genentech, Pfizer and Abbott. Dr Suhler, Dr Rosenbaum and Ms Giles have received research support from Abbott, Bristol-Myers-Squibb, EyeGate, Genentech, LuxBio and Novartis. Dr Goldstein has served as a paid consultant to Bausch and Lomb, Allergan, GSK, Santen, LuxBio, and serves on an IDMC for Abbott. Dr Lowder serves on an advisory board for Allergan. Authorship is based on (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
References
Footnotes
-
Contributors All authors contributed to acquisition of study data, authorship of publication, and/or critical editing of manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.