Article Text

Abstract
Aim To compare efficacy (intraocular pressure (IOP) reduction) and safety of preservative-free latanoprost (T2345) to benzalkonium chloride (BAK)-preserved latanoprost (BPL; Xalatan) in ocular hypertension (OHT) or primary open angle glaucoma (POAG) patients.
Methods Prospective, international, multicentre, randomised, investigator-masked, parallel–group trial. After a wash-out period, POAG or OHT patients, previously managed by BPL monotherapy, randomly received T2345 or BPL (one drop into the affected eye(s)) once daily from D0 to D84. Change in IOP was measured at 09:00 (±1 h) from D0 to D84 in the worse eye.
Results Mean IOP reduction (D0–D84) was −8.6±2.6 mm Hg (−36%) on T2345 and −9.0±2.4 mm Hg (−38%) on BPL, confirming non-inferiority of T2345 to BPL. Non-inferiority of T2345 was observed from D15. The most frequent ocular adverse event, drug intolerance, was reported in 1 (0.5%) patient on T2345 versus 4 (2.1%) patients on BPL. Moderate to severe conjunctival hyperaemia was less frequent on T2345 than on BPL at D42 (20.2% vs 30.6%; p=0.003) and D84 (21.4% vs 29.1%; p=0.02). Upon instillation, the global subjective ocular symptom score was significantly lower on T2345 than BPL on D42 (0.15 vs 0.41; p=0.001) and D84 (0.18 vs 0.46; p=0.001).
Conclusions Preservative-free latanoprost has the same efficacy as BPL, with improved local tolerance.
- Intraocular Pressure
- Glaucoma
Statistics from Altmetric.com
Introduction
Over the last 15 years, the pharmacological management of glaucoma and ocular hypertension (OHT) has significantly changed with the introduction of the prostaglandin analogues (PGAs), specifically latanoprost, bimatoprost, travoprost, and more recently tafluprost. PGAs administered once per day are a popular choice of therapy given their effective reduction of intraocular pressure (IOP) and accepted safety profiles, and are currently recommended by European Glaucoma Society Guidelines (2008) for the first-line treatment of glaucoma.1
PGAs have demonstrated consistent superiority in IOP reduction over β-adrenergic blockers, α-adrenergic agonists or topical carbonic anhydrase inhibitor therapies.2 ,3 Among PGAs, no major differences in efficacy were observed between latanoprost versus bimatoprost,4 ,5 travoprost4 ,5 or tafluprost.6 Furthermore, when compared with other PGAs, latanoprost consistently exhibited greater ocular tolerability with few adverse events (AEs), suggesting a better efficacy/tolerability ratio.4–7 Reported local untoward effects related to latanoprost were mainly conjunctival hyperaemia, increased eyelash growth and iris colour darkening.8
Latanoprost is marketed as a 0.005% ophthalmic solution containing 0.02% of the preservative benzalkonium chloride (BAK), representing a BAK concentration twice that of most other glaucoma drops. BAK may contribute significantly to the ocular toxicity and inflammation associated with the chronic use of PGAs,9 and may have an important role in the main observed AEs such as conjunctival hyperaemia, decreased tear turnover, reduced tear film break-up time and inflammatory cell infiltration of the cornea.10 Furthermore, prolonged exposure to BAK causes indirect and direct toxic effects to the ocular surface, with reduced cellular viability and compromised epithelial barrier function.11
A preservative-free formulation of latanoprost eye drops, the most widely used PGA, called T2345 has been developed to avoid the undesirable effects of BAK. The efficacy of T2345 in reducing IOP was tested in a non-inferiority phase III study.
Methods
Study design and patients
This was an international, multicentre, randomised, investigator-masked, parallel-group clinical study, conducted in five European countries (France, Belgium, Italy, Spain, Portugal) and Tunisia, comparing the preservative-free latanoprost formulation T2345 (Laboratoires Théa) with BAK-preserved latanoprost (BPL; Xalatan, Pfizer) during a 3-month treatment period. Given that T2345 is supplied in single dose units and BPL in bottles, the investigator measuring IOP during ophthalmological examination was masked to study medication. The study was approved by ethics committees of participating countries and centres, and was conducted according to the Declaration of Helsinki (2004), Good Clinical Practice, and local regulations. All participating patients provided written informed consent. The study was registered on the clinicaltrials.gov website with the identifier NCT01156012.
The study enrolled male or female adult patients (≥18 years of age) with chronic primary open angle glaucoma (POAG) or OHT, already managed by BPL monotherapy for at least 9 months as defined by stable IOP (≤18 mm Hg) and stable visual field (based on two visual fields available within the last 18 months, including one in the last 6 months), and corneal thickness ≥500 and ≤580 µm. Primary exclusion criteria included any secondary OHT, severe glaucoma (defined by advanced cupping and/or severe visual loss, notably an absolute defect in the 10° central point), corrected visual acuity ≤1/10, filtration or laser surgery for glaucoma (within the last 12 months), other intraocular surgery (except filtration surgery within the last 6 months), and abnormality preventing accurate IOP assessment.
Following a screening visit (D-42), selected patients discontinued their current treatment for 6 weeks prior to randomisation (D0). During this run-in period, patients were treated with brinzolamide eye drops (10 mg/ml), one drop twice daily for 5 weeks. Brinzolamide treatment was stopped 5 days before randomisation. Patients were randomised if IOP was ≥22 mm Hg in the eligible eye(s). Patients were randomised 1 : 1 to monotherapy with either T2345 or BPL. Patients were instructed to instil one drop in each eye once daily in the evening (9 : 00 pm±1 h) and were scheduled for follow-up visits at D15, D42 and D84.
Assessment parameters
The primary efficacy variable was the change in IOP between D0 and D84 in the worse eye, which was defined as the eligible eye with the highest IOP at randomisation. Mean IOP (average of 2 or 3 consecutive IOP measurements) was measured at the same hour (09 : 00 am±1 h) at each visit using a calibrated Goldmann applanation tonometer.
Safety outcome measures included AE reporting, ocular signs on slit-lamp biomicroscopy, and ocular symptoms upon and not upon instillation (see legends of table 4). Conjunctival hyperaemia was scored using a standardised photographic scale derived from McMonnies grading (1–6). Other biomicroscopic findings were scored on a four-grade scale of none (0), mild (1), moderate (2) and severe (3). All AEs observed by the investigator or reported by patients were recorded, along with their severity and potential relationship to study treatment.
Statistical analyses
Results were obtained from the worse eye. The analysis of efficacy was primarily performed on a modified Intent-To-Treat (mITT) set (all randomised patients with at least one eligible eye, who received at least one dose of study treatment, and for whom any follow-up IOP data was available). For confirmatory purposes, the efficacy analysis was also performed on the intent-to-treat (ITT) and per protocol (PP) sets. Tolerance was evaluated for the Safety set (all patients who used study medication and with any available safety data).
Statistical analysis consisted of descriptive statistics for the quantitative variables, and frequency distribution for the categorical variables. The primary efficacy variable was analysed using a mixed effect model for repeated measures adjusting for baseline IOP, treatment, visit, country, treatment by visit interaction and baseline IOP by visit interaction. Treatment difference for the primary criterion was estimated with a 2-sided 95% CI and a 1.5 mm Hg non-inferiority margin. Other quantitative variables were analysed using an analysis of covariance (ANCOVA) model, and the ordinal and binary variables using the Cochran-Mantel-Haenszel test. All statistical tests performed were two-sided, at the 5% level of significance.
Results
Patient baseline characteristics and disposition
A total of 463 patients were screened; 404 were randomised and 402 received the study treatment: 213 in the T2345 group and 189 in the BPL group (Safety Set; figure 1). The mITT Set consisted of 353 patients (189 in the T2345 group and 164 in the BPL group); 392 patients completed the study (206 for T2345, 96.3%; 153 for BPL, 97.9%). Patient characteristics at baseline are presented in table 1; no relevant difference was noted between treatment groups.
Patient characteristics at baseline—safety set

Study flow diagram.
IOP-lowering efficacy
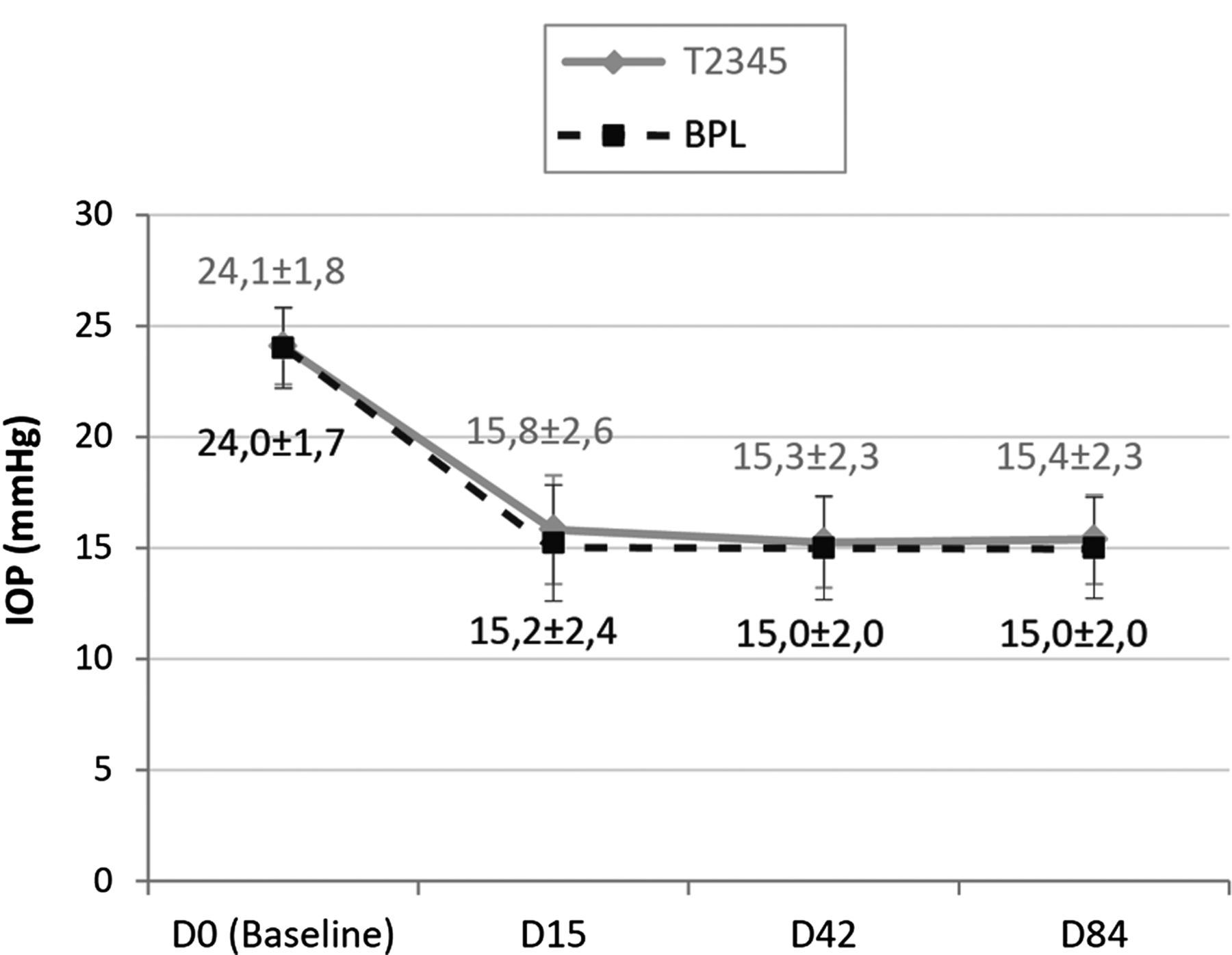
In the mITT Set, the mean IOP decreased from 24.1±1.8 at D0 to 15.4±2.3 mm Hg at D84 in the T2345 group, and from 24.0±1.7 at D0 to 15.0±2.0 mm Hg at D84 in the BPL group (figure 2). The majority of the IOP reduction was observed by D15 in both groups, with further small decreases at D42. The mean IOP decreased from baseline to D84 by 36% in the T2345 group and 38% in the BPL group (table 2). The 95% CI of the mean estimated difference between treatments (T2345 minus BPL) in the change from baseline IOP to D84 was (−0.006 to 0.840), respecting the upper limit of the non-inferiority margin (1.5 mm Hg).
IOP change from D0 to D84—mITT set
{kind=link}
{kind=link}
Mean intraocular pressure (IOP) at each assessment time. Error bars represent the SE of the mean.
The mean reduction from baseline IOP was −8.3±2.7 mm Hg (−34%) in the T2345 group and −8.8±2.7 mm Hg (−37%) in the BPL group on D15, and −8.8±2.6 mm Hg (−37%) in the T2345 group and −9.0±2.5 mm Hg (−38%) in the BPL group on D42. The mean estimated treatment differences (T2345 minus BPL) in the change from baseline IOP to D15 was 0.572 (95% CI, −0.083 to 1.061) and to D42 was 0.274 (95% CI, −0.157 to 0.705) mm Hg, confirming the non-inferiority hypothesis at visits D15 and D42. Non-inferiority was also demonstrated in the ITT and PP sets at all evaluation times. The investigator assessed the global efficacy of the study medication as ‘very satisfactory’ or ‘satisfactory’ for at least 96% of patients in both treatment groups at each visit.
Safety and tolerabilty
Adverse events
Ocular AEs were reported in 18 (8.5%) patients in the T2345 group versus 22 (11.6%) patients in the BPL group, without any serious AEs. The most frequent ocular AE, regardless of treatment groups, was drug intolerance which was reported in 1 patient (0.5%) on T2345 and 4 (2.1%) patients on BPL. All ocular AEs were of mild or moderate intensity, except for one severe AE of ocular discomfort reported in the T2345 group. Treatment-related ocular AEs were reported in 8 (3.8%) patients in the T2345 group versus 10 (5.3%) patients in the BPL group.
Systemic AEs were reported in 28 (13.1%) patients in the T2345 group and 30 (16.9%) patients in the BPL group. None of the systemic AEs were related to the study drug in the T2345 group, while 6 AEs of mild intensity, reported in 4 (2.1%) patients, were considered by the investigator as related to BPL treatment (2 patients had headache and 1 patient each had dizziness, migraine, palpitation and muscular weakness).
Objective ocular signs
Conjunctival hyperaemia was less frequent and severe in the T2345 group than in the BPL group, with a statistically significant lower incidence apparent at D42 (20.2% vs 30.6%, p=0.003) and D84 (21.4% vs 29.1%, p=0.019; table 3). Importantly, the percentage of moderate to severe hyperaemia decreased over time in the T2345 group (7.5%, 7.1%, 5.3% and 4.9% at D0, D15, D42 and D84, respectively), and increased over time in the BPL group (2.6%, 5.9%, 8.6% and 7.6% at D0, D15, D42 and D84, respectively). No difference between treatment groups was observed for other objective signs (corneal punctate staining, anterior chamber flare, folliculo-papillary conjunctivitis, palpebral abnormality).
Conjunctival hyperaemia score (worse eye) at each visit—safety set
Subjective ocular symptoms
The subjective ocular symptom score upon instillation of eye drops was significantly lower in the T2345 group than in the BPL group on D42 and D84 (p=0.001; table 4). The difference between treatments tended to increase throughout the study, and was largely due to a difference in the percentage of patients experiencing burning/stinging with T2345 and BPL, respectively: 5.2% versus 14.0% on D15 (p=0.004), 6.8% versus 15.1% on D42 (p=0.006), and 7.3% versus 19.9% on D84 (p<0.001).
Total subjective ocular symptom† score upon instillation—safety set
A trend for less subjective ocular symptoms between instillations was also observed in the T2345 group compared with the BPL group on D42 (total score: 0.47±1.19 vs 0.65±1.54, p=0.057) and D84 (total score: 0.47±1.37 vs 0.69±1.73, p=0.053).
Global tolerance assessment
According to the investigator, the tolerance was very satisfactory or satisfactory for more than 97% of patients in both treatment groups. However, the rate of “very satisfactory” was higher in the T2345 group versus the BPL group on D15 (65.1% vs 59.7%), D42 (74.0% vs 65.1%) and D84 (71.4% vs 62.9%), and the global tolerance assessment was in favour of T2345 at D42 (p=0.013) and D84 (p=0.047).
Discussion
This study demonstrated the non-inferiority of unidose preservative-free latanoprost eye drops (T2345) to multidose BPL in reduction of IOP. This was shown from the first assessment time (ie, 15 days after treatment initiation), and the IOP reduction was maintained for the duration of the study. The percentage reduction of IOP from baseline at D84 was −36% for T2345 and −38% for BPL, corresponding to the upper limit of the range of the optimal reduction in IOP expected with latanoprost 0.005% (between −22% and −39%).4 ,12 ,13 Moreover, according to the investigators, the efficacy of both study medications was deemed ‘very satisfactory’ or ‘satisfactory’ in more than 96% of patients at all visits.
Some authors have reported increased penetration of BAK preserved drugs to the eye, probably due to its detrimental effect to the ocular surface, and thus hypothesised that preservatives play an important role in the drug penetration into the eye by loosening tight junctions between corneal epithelial cells.14–16 However, this finding is controversial as some clinical studies comparing PGAs with and without BAK demonstrated similar efficacy.17 ,18 In a recent study, Pellinen and Lokkila (2009) demonstrated comparable corneal penetration of preserved and preservative-free tafluprost in the aqueous humour of rabbits.19 Tafluprost is currently the only preservative-free PGA on the market with proven non–inferiority efficacy to timolol.20 Our findings do not indicate that the IOP-lowering efficacy of latanoprost is dependent upon the presence of BAK. The relatively high BAK concentration (0.02%) in preserved latanoprost has been justified by the popular assumption that BAK is necessary for latanoprost solubilisation, and that BAK acts as a protective and stabilising agent for PGA. The formulation of T2345 eye drops has been developed based on specific polymeric agents which (1) allow stabilisation of latanoprost in the absence of BAK and at room temperature, and (2) facilitate ocular penetration of PGA.
The safety results suggest a better local tolerance of T2345 compared with BPL, with less conjunctival hyperaemia and less subjective symptoms upon instillation (especially burning/stinging and pruritus). These observations may be explained by the absence of the preservative BAK in the T2345 formulation.
Among the many studies demonstrating an improved safety profile in subjects receiving unpreserved formulations compared with preserved formulations, Pisella et al21 ,22 showed that removal of preservative from timolol ophthalmic solution resulted in improved corneal epithelial barrier function, prevention of ocular surface inflammation and reduction of complaints. The improvement was found to be proportional to the duration of the preceding preservative–containing therapy.23 In clinical practice, patient complaints and objective damage to the ocular surface were more frequent among patients treated with preserved eye drops.24 The switch from preserved to preservative-free topical antiglaucoma medication was associated with a significant increase in tear break-up time and decrease in corneal staining and ocular surface disease index.25 ,26 In a long-term 12-month prospective study, fewer ocular surface complications were observed with BAK-free travoprost than with preserved latanoprost, with a reduced prevalence of superficial punctate keratitis and less hyperaemia. No clinically relevant changes in IOP were observed.27 Recently, Baudouin et al reviewed the large body of evidence from experimental and clinical studies showing that the long-term use of preservatives, and in particular BAK, in topical drugs may induce ocular surface changes causing ocular discomfort, tear film instability, conjunctival inflammation, subconjunctival fibrosis, epithelial apoptosis, corneal surface impairment, and the potential risk of failure for further glaucoma surgery.10 On the basis of these data, BAK-free solutions should be used whenever possible, especially in patients with exposure to prolonged treatments, and in patients suffering from pre-existing or concomitant ocular surface diseases. The ocular surface side effects of preserved anti–glaucoma medications should not be neglected as they may deeply impact patients’ quality of life, compliance and later surgical outcome.
T2345 is the first preservative-free formulation of latanoprost to demonstrate non-inferiority compared with BPL in reducing IOP. T2345 also had a more favourable safety profile, most notably for subjective symptoms upon instillation and conjunctival hyperaemia.
Acknowledgments
The authors wish to thank the investigators of the T2345 Study Group for allowing their patients to be included in this trial.
References
Footnotes
-
Collaborators France: Dr Arnoux Yvon, Dr Baron Philippe, Dr Boudouard Marie-Noëlle, Pr Bremond-Gignac Dominique, Pr Chiambaretta Frédéric, Dr Chretien-Malinconi Anne, Dr Clausel Laurent, Pr Cochereau Isabelle, Pr Colin Joseph, Dr Corlay Jean Pierre, Pr Bron Alain, Dr Dusseuil Olivier, Dr Francoz Nicole, Dr Hanoun François, Dr Jaulerry Stéphane, Dr Katan Alain, Pr Kodjikian Laurent, Dr Lamoureux Andrée, Pr Labetoulle Marc, Dr Blumen-Ohana Esther, Dr Pincemin Daniel, Pr Pisella Pierre-Jean, Dr Puyal Gaby, Pr Robert Pierre-Yves, Dr Rozot Pascal, Dr Sabadel Anne, Dr Veschambre-Cavaroc Marie-Claude, Dr Vounatsos Jean-Paul, Dr Williamson Wilfrid, Dr Peyre Catherine, Pr Gain Philippe, Dr Ligeon-Ligeonnet Patrick, Dr Le Bot François-Bruno, Dr Gaultier Isabelle, Dr Alliot Emmanuel, Dr Gabisson Pierre, Pr Renard Jean-Paul, Dr Auzerie Olivier, Dr Ballonzoli Laurent, Dr Cousin Philippe, Dr Payan Jacques, Dr Roncin Stéphane, Dr Vincent Alain, Dr Maalouf Toufic, Dr Briat Benoït, Dr Conan Stefan, Dr Gracies Henri, Dr Delemazure Barbara, Dr Mounier Gilles, Dr Collet Anne. Belgium: Pr De Groot Veva, Dr Stevens Anna-Maria, Pr Zeyen Thierry, Pr Detry Morel Michèle, Dr Ehongo Adèle, Dr Collignon Nathalie. Italy: Pr Grignolo Federico, Pr Marchini Giorgio, Pr Vetrugno Michèle, Pr Mastropasqua Leonardo. Spain: Dr Corsino Fernandez Vila Pedro, Dr Duch Tuesda Susana, Dr Lillo Sopena Juan, Dr Ayala Fuentes Miriam Eleonora, Dr Teus Guezala. Portugal: Pr Castanheira Dinis António, Dr Ribeiro Luisa, Pr Silva José Pedro, Pr Falcao Reis Fernando, Pr Teixeira Monteiro Grillo Manuel Eduardo, Pr Segurado Joao. Tunisia: Pr Ouertani Amel, Dr Messaoud Riadh, Pr El Matri Leila, Khairallah Moncef, Pr Ben-Hadjhamida Fafani, Pr Ayed Saïda, Pr Jeddi Amel, Pr Kraiem Abdelhafid, Dr Kamoun Mohamed, Pr Rekik Raouf, Dr Nouira Fathi, Dr Chachia Nejib, Pr Gabsi Salem, Pr Feki Jamel.
-
Contributors LD and DR participated in the design and conduct of the study. J-FR, CET, IS, LEF and CB were all investigators of the study, participated in the conduct of the study, and in the review and approval of the manuscript.
-
Funding This study was sponsored by Laboratoires Théa.
-
Competing interests LD and DR are employed by Laboratoires Théa. J-FR; CET; IS; LEF; and CB were investigators of the study and received financial compensation.
-
Provenance and peer review Not commissioned; externally peer reviewed
-
Correction notice This article has been corrected since it was published Online First. The Acknowledgements section has been changed into the Collaborators section.