Article Text

Abstract
Background To assess prevalence and causes of blindness and vision impairment in high-income regions and in Central/Eastern Europe in 1990 and 2010.
Methods Based on a systematic review of medical literature, prevalence of moderate and severe vision impairment (MSVI; presenting visual acuity <6/18 but ≥3/60 in the better eye) and blindness (presenting visual acuity <3/60) was estimated for 1990 and 2010.
Results Age-standardised prevalence of blindness and MSVI decreased from 0.2% to 0.1% (3.314 million to 2.736 million people) and from 1.6% to 1.0% (25.362 million to 22.176 million), respectively. Women were generally more affected than men. Cataract was the most frequent cause of blindness in all subregions in 1990, but macular degeneration and uncorrected refractive error became the most frequent causes of blindness in 2010 in all high-income countries, except for Eastern/Central Europe, where cataract remained the leading cause. Glaucoma and diabetic retinopathy were fourth and fifth most common causes for blindness for all regions at both times. Uncorrected refractive error, followed by cataract, macular degeneration, glaucoma and diabetic retinopathy, was the most common cause for MSVI in 1990 and 2010.
Conclusions In highly developed countries, prevalence of blindness and MSVI has been reduced by 50% and 38%, respectively, and the number of blind people and people with MSVI decreased by 17.4% and 12.6%, respectively, even with the increasing number of older people in the population. In high-income countries, macular degeneration has become the most important cause of blindness, but uncorrected refractive errors continue to be the leading cause of MSVI.
- Epidemiology
- Glaucoma
- Public health
Statistics from Altmetric.com
Blindness and vision impairment have a great impact on quality of life and are of high importance for the socioeconomics and public health of countries. A recent systematic review estimated that globally 32.4 million people, with 60% of them women, were blind (defined as presenting visual acuity <3/60 in the better eye) in 2010 and 191 million people (57% women) had a moderate and severe vision impairment (MSVI; defined as presenting visual acuity <6/18 but ≥3/60 in the better eye).1–3 In the past, cataract was the major cause of visual impairment and blindness, but it is expected that with aging populations other conditions such as age-related macular degeneration (AMD), diabetic retinopathy and glaucoma will become more important causes of vision loss.
Since there were marked differences between regions in the prevalence of blindness and MSVI, its causes and temporal changes during the last 20 years,3 we analysed the prevalence and causes of blindness and MSVI, focusing on high-income countries (eg, USA, Western Europe, Australia, Japan, etc.) and on Eastern and Central Europe (HIC/EC-Europe) (table 1). Countries from Eastern and Central Europe were added to the group since these countries were geographically located close to Western Europe.
Countries included into the category of ‘high-income countries, Eastern and Central Europe’
Methods
A systematic review of medical literature from 1 January 1980 to 31 January 2012 identified indexed articles containing data on incidence, prevalence and causes of blindness and MSVI.3–5 Only cross-sectional population-based representative studies were selected from which to extract data for a database of age-specific and sex-specific data of prevalence of four distance vision impairment categories (presenting and best-corrected). Unpublished data and data from studies using ‘rapid assessment’ methodology were added later. Despite extensive data seeking, data were not available for many countries and years, were reported using incomparable definitions of vision impairment or were representative of a subnational or community area only. Statistical methods were used to generate estimates of the prevalence and causes of presenting vision blindness and MSVI for each country and year, 1990–2010, in 190 countries nested in 21 Global Burden of Disease (GBD) subregions.3 We estimated the contribution of six causes of vision impairment and blindness: cataract, macular degeneration (including AMD, myopic maculopathy, macula hole and any other macular disorder), glaucoma (all types of glaucoma combined), diabetic retinopathy, trachoma and uncorrected refractive error (estimated as the difference between presenting and best-corrected vision impairment, including aphakia). We also estimated the fraction of visual impairment that had other causes. We made estimates for MSVI and blindness.
For the statistical analysis, we used DisMod-MR, an age-integrating Bayesian multilevel regression tool, for the calculation of cause fractions for major causes of vision impairment to calculate the fraction of vision impairment due to causes mentioned above.2 ,3 For the assessment of the cause fraction of uncorrected refractive error, the total prevalence of vision impairment and its uncertainty were estimated using prevalence data of blindness and MSVI based on presenting visual acuity and best-corrected visual acuity. This model estimated the difference between the prevalence of blindness (and of MSVI) based on presenting visual acuity and on best-corrected visual acuity prevalence, respectively. We interpreted this difference as the fraction of vision impairment caused by undercorrected refractive error. DisMod-MR produced 1000 draws for each country and by sex and age, for 1990 and 2010; we used 500 of these draws (for computational efficiency by selecting every second draw from the DisMod-MR output) to reflect uncertainty in the DisMod-MR estimates and the mean of the draws as the central estimate. These draws represent the vision impairment envelope’s uncertainty distribution and comprise predictions for each country/year/sex combination. We also extracted the central estimate and 500 draws of the proportion of vision impairment caused by uncorrected refractive error, as described previously. For the central estimate and each draw, we normalised the proportions attributable to six causes of best-corrected vision loss, cataracts, glaucoma, macular degeneration, diabetic retinopathy, trachoma and other vision loss, to sum to the remaining vision impairment not due to uncorrected refractive error. We applied the resulting cause fractions to previously estimated prevalence of blindness and MSVI by country, age, sex and draw. We presented uncertainty intervals in summary estimates as the 2.5th–97.5th centiles of the distribution of draws for both all-cause prevalence and also cause-specific prevalence. For presentation, we age-standardised prevalences using the WHO reference population. We used 5-year age groups from 0 to 89 years (ie, 0–4, 5–9,.…, 85–89 years), with the last age group being an open-ended age group starting at age 90 years. We also calculated the number of people with vision impairment by cause, calculated as the product of prevalence and population. The calculation was made by age, sex and country, and then summed to obtain regional totals.
The statistical analysis was carried out in three main steps. First, a series of regression equations were used to estimate the prevalence of blindness (visual acuity <3/60) and MSVI (visual acuity <6/18 but ≥3/60) when other definitions of vision impairment were reported. Second, two hierarchical logistic regressions were fitted to both presenting and best-corrected vision impairment data to estimate the prevalence of presenting MSVI and blindness by age, country and year. These models were also used to estimate the contribution of refractive error based on the estimated difference between presenting and best-corrected vision impairment. Third, separate models were fit to calculate the proportion of blindness and MSVI caused by cataract, macular degeneration (including AMD, myopic maculopathy, macular hole and any other macular disorder), glaucoma (all types of glaucoma combined), diabetic retinopathy, trachoma and uncorrected refractive error. Statistical uncertainty was estimated at each stage of the statistical analysis and is reflected in the final estimates of vision impairment prevalence by cause. The statistical methods have been described in detail previously.3 ,4
Results
Overall, out of 14 908 articles primarily searched by the GBD 2010, 243 studies described in 252 articles and reports remained after exclusion of ineligible studies and after further inclusion of unpublished data from population-based studies, government reports and rapid assessment surveys. A complete list of the 243 studies is available online.5 HIC/EC-Europe were the focus for 37 studies (table 1). All of the included studies were cross-sectional population-based investigations, and the visual acuity data were ascertained through clinical examination. The majority of studies (32/37) included a broad age range in the adult population. Out of the 37 studies, 27 were performed in urban regions, 3 studies in rural areas, and 7 investigations were carried out in rural and urban regions.
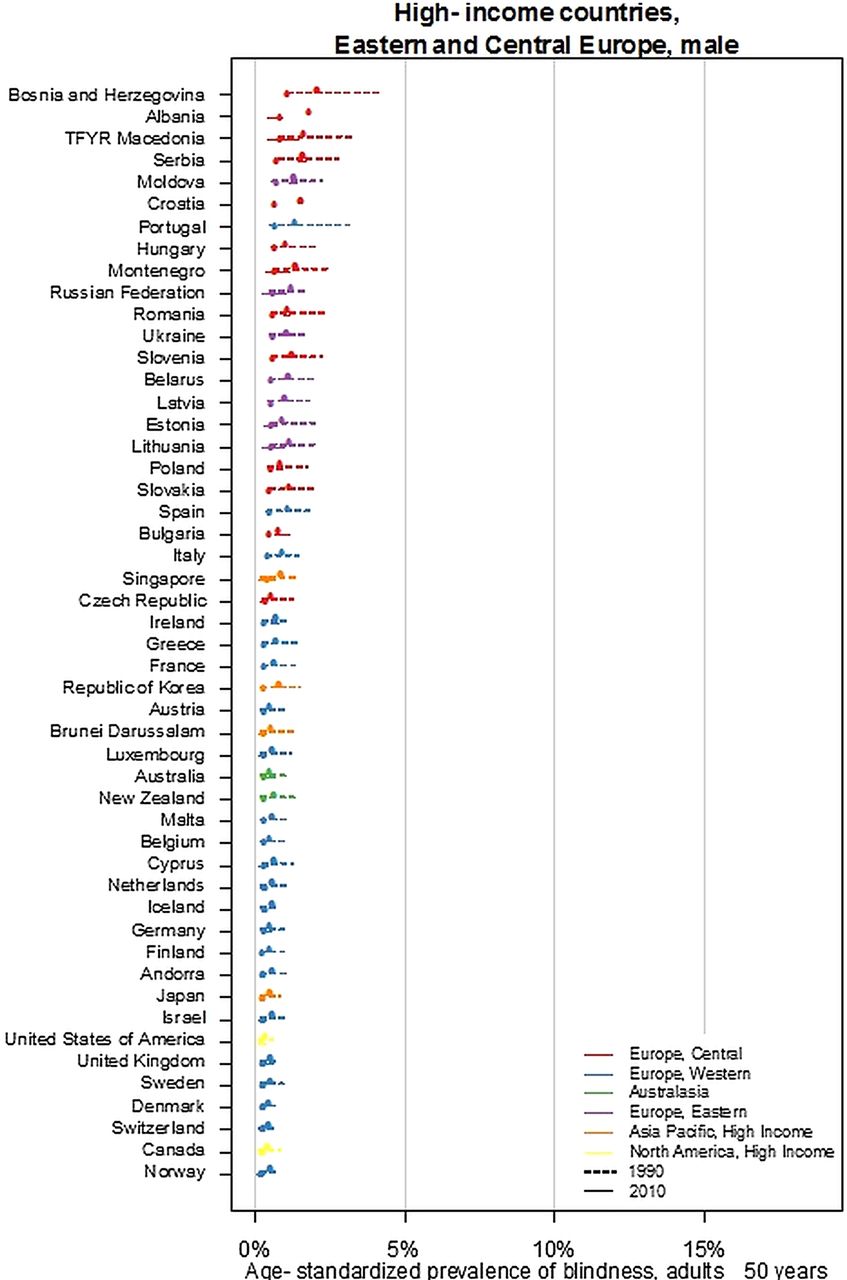
From 1990 to 2010, the age-standardised prevalence of blindness for all ages and for adults aged 50+ years decreased from 0.2% to 0.1% and from 0.8% to 0.4% (table 2; figure 1), respectively, and the age-standardised prevalence of MSVI decreased from 1.6% to 1.0% and from 6.0% to 3.8%, respectively (figure 2). These figures were markedly lower than the figures for the global population (table 2). The overall prevalence of blindness and the number of people affected were generally higher among women than among men across all regions and for both 1990 and 2010, as was the overall prevalence of MSVI (tables 2 and 3). The top causes of blindness changed from 1990 to 2010 (table 4). In 1990, cataract, followed by macular degeneration, was the most frequent cause of blindness in all subregions. Due to a significant decrease in the proportion of blindness due to cataract and an increase in AMD, macular degeneration became the most frequent cause of blindness in 2010 in the high-income countries of Asia Pacific, Australia, Western Europe and high-income North America, while only in Eastern and Central Europe did cataract remain the leading cause. In the high-income regions, uncorrected refractive error was the second cause of blindness, with cataract the third most frequent cause. In 1990 and 2010, the ranking of glaucoma (fourth) and diabetic retinopathy (fifth) remained unchanged for all subregions examined.
Age-standardised prevalence of moderate and severe vision impairment (MSVI; presenting visual acuity <6/18 but ≥3/60) and blindness (presenting visual acuity <3/60) by sex and year in high-income countries (HIC) and Eastern and Central Europe (Europe) for 1990 and 2010
Absolute numbers of people affected by moderate and severe vision impairment (MSVI; presenting visual acuity <6/18 but ≥3/60) and blindness (presenting visual acuity <3/60) by sex and year in high-income countries (HIC) and Eastern and Central Europe (Europe) (all ages) for 1990 and 2010
Percentage of blindness (presenting visual acuity <3/60) by cause, regions and the world, 1990 and 2010, all ages


Ladder plot showing the age-standardised prevalence of blindness and change in men (A) and women (B) aged 50+ years for 1990 and 2010.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ladder plot showing the age-standardised prevalence of moderate to severe visual impairment (MSVI) and change in men (A) and women (B) aged 50+ years for 1990 and 2010.
Uncorrected refractive error was the leading cause of MSVI in both 1990 to 2010. It was followed by cataract and macular degeneration, then by glaucoma and diabetic retinopathy, without any major difference between the subregions (table 5).
Proportion of moderate and severe vision impairment (MSVI; presenting visual acuity <6/18 but ≥3/60) by cause, regions and the world, 1990 and 2010, all ages
In 2010, the number of blind people of all ages was about 473 000 in high-income North America (cataract: 60 100 (12.7%) people; uncorrected refractive error: 66 700 (14.1%); macular degeneration: 77 600 (16.4%); glaucoma: 50 600 (10.7%); diabetic retinopathy: 18 400 (3.9%) people). The number was 956 000 blind people in Western Europe (cataract: 131 900 (13.8%) people; uncorrected refractive error: 133 800 (14.0%); macular degeneration: 153 900 (16.1%); glaucoma: 101 300 (10.6%); diabetic retinopathy: 40.200 (4.2%) people). In the whole region of HIC/EC-Europe, the number of blind people declined by 17.4%, from 3.314 million in 1990 to 2.736 million in 2010.
The number of people with MSVI was 3.102 million in North America (cataract: 403 300 (13.0%) people; uncorrected refractive error: 1 492 100 (48.1%); macular degeneration: 170 600 (5.5%); glaucoma: 105 500 (3.4%); diabetic retinopathy: 86 900 (2.8%) people). The number of people for Western Europe was 7.490 million (cataract: 1 033 600 (13.8%) people; uncorrected refractive error: 3 542 800 (47.3%); macular degeneration: 404 500 (5.4%); glaucoma: 254 700 (3.4%); diabetic retinopathy: 224 700 (3.0%) people). In the whole region of HIC/EC-Europe, the number of people with MSVI decreased by 12.6%, from 25.362 million in 1990 to 22.176 million in 2010.
Discussion
Summarising data published in available epidemiological studies between 1980 and 2012, our study model suggested that the high-income countries, including the USA, Western Europe, Australia and Japan, have a relatively low prevalence of blindness and MSVI. While cataract was the most frequent cause of blindness in 1990, in the last 20 years the situation has changed, and now macular degeneration, including AMD and myopic macular degeneration, has become the most common cause of blindness. Only in the countries of Eastern and Central Europe does cataract remain as the leading cause of blindness, although our model also suggested that there was a marked decline in cataract blindness in these countries (table 4). The causes for MSVI remained unchanged for the period from 1990 to 2010 with uncorrected refractive error as by far the most frequent cause of visual impairment (table 5). The findings obtained in the high-income regions were different from those from other world regions, in which the prevalence of visual impairment and blindness was markedly higher than in the high-income countries and in which cataract remained the most frequent cause of visual impairment and blindness. The findings of our study have public health implications for hospital planning, resource allocation, training of eye-care providers and public education.
The prevalence of age-related blindness and MSVI in older people (50 years and above) in the high-income regions was markedly lower than the figures for the global adult population. It shows the inverse association between the level of socioeconomic background and prevalence of visual impairment. In absolute percentage points, the decrease in age-related blindness and MSVI in older people was lower in the high-income regions (decrease from 0.8% to 0.4% and from 6.0% to 3.8%, respectively) than globally (decrease from 3.0% to 1.9%; and from 14.3% to 10.4%, respectively (table 2)).6–14 In relative terms, however, blindness decreased by 50% in HIC/EC-Europe while it decreased by only 37% globally. Similarly, MSVI decreased by 37% in HIC/EC-Europe versus 27% globally. The high-income regions showed a higher prevalence of blindness and MSVI for women than men (tables 2 and 3).15 This difference has been found in most regions and may reflect differential use or access to services, although the increased life expectancy will also play a role with the use of broad age categories for age-related conditions. Future public health measures may have to address providing equal opportunity in having good vision for both genders in all age groups.
In 2010, ‘macular degeneration’ as a group has replaced cataract as the most frequent cause of blindness in high-income regions. This change may have been due to a further increase in the number of cataract surgery, an increased life expectancy leading to an increased prevalence of AMD, and it may reflect the challenges in treatment of AMD. The increased importance of macular diseases in the Asia-Pacific region may also be associated with AMD, 16 as well as high rates of myopia with the risk of myopic macular degeneration.17 ,18 This trend is important as both AMD and myopic macular degeneration are now increasingly treatable (eg, with antivascular endothelial growth factor (VEGF) therapy), and strategies to increase patient awareness, improve access to these new therapies and appropriate training of eye-care specialists in these areas will be increasingly important.19 In some countries such as Denmark and Israel, the introduction of anti-VEGF therapy has led to a decline in prevalence of visual impairment due to macular degenerations such as AMD or myopic maculopathy.20
The most frequent cause of MSVI, and the third most common cause of blindness, was uncorrected refractive error (tables 4 and 5). It shows that even for the highly developed countries one of the most effective, cheapest and safest ways of improving vision loss by providing adequate spectacles for correcting refractive errors is being overlooked.
Finally, the impending epidemic of diabetes on blindness and vision loss should be addressed.21 It is estimated that there will be more than 100 million people with diabetic retinopathy and possibly 30 million will be at risk of severe sight-threatening retinopathy.22 Importantly, many people with diabetes are not only at risk of diabetic retinopathy but also cataract and glaucoma23; thus, the impact of diabetes is multifold. Strategies to screen for diabetic retinopathy and provide timely treatment access are critical to prevent this condition from having a greater impact on blindness prevalence in the future.
The limitations of our study include the following: First, that there were very few to no national studies, so we were making inference from community studies. Second, some studies were inconsistent about including nursing homes, which are home to many older blind people and therefore were important to include. Third, some data sources did not report prevalence by age, so we had to impute age-specific cause fractions.3 Fourth, there were only three surveys available for Central and Eastern Europe, so country-years remained without data or only had only subnational data.3 This may be a major limitation in view of the significant challenges the countries in Eastern and Central Europe went through during the period under consideration. Fifth, the group ‘macular degeneration’ included AMD and myopic macular degeneration, so we could not differentiate between the two latter entities. It may be of importance for high-income countries in East Asia, where myopic macular degeneration ranked among the three most common causes for vision impairment and blindness.17 ,18 ,24 Sixth, the basic studies varied in the definition of the diseases such as glaucoma,25 and unidentified or ‘other’ causes generally represented about 20–30% of the causes for MSVI and approximately 20–35% of the causes of blindness. Seventh, the protocols of most population-based studies required only one cause of vision impairment to be given as the main reason for an individual examined in that particular study in order to arrive at the causal prevalence. When there were multiple disorders contributing equally to visual loss, only the ‘most readily curable’ or the ‘‘most easily preventable’ was recorded.26 Eighth, near vision was not considered, so uncorrected presbyopia-related visual impairment was not effectively taken into account. Last but not least, one may consider that the prevalence of blindness for adults in 1990 was 0.8% in the high-income countries, so the maximum possible reduction could have been only 0.8%. It indicates that in absolute terms it was easier for other regions to reduce their prevalence of blindness since they started at a higher level. This may not hold true if the changes in the prevalence of blindness and MSVI are calculated in relative terms.
In conclusion, macular degenerations, which includes AMD and myopic macular degeneration, have replaced cataract as the most important cause of blindness in highly developed countries, showing the necessity to develop strategies to increase access to new therapies, such as anti-VEGF therapy. Importantly, even in rich countries, uncorrected refractive errors are the leading cause of visual impairment, so measures to provide adequate access to correction of refractive errors including presbyopia appear to be the easiest, safest and cheapest to decrease vision loss in the general population. However, the last 20 years has seen substantial decreases in both the prevalence and the number of blind and visually impaired in countries in this region.
Acknowledgments
Benita J O'Colmain assisted with the incorporation of microdata from several large population-based studies. The principal investigators of these and other studies are thanked for authorising unpublished study data to be used in this project. Catherine Michaud and Colin Mathers greatly assisted in the communications between the GBD Core Group and the GBD Vision Loss Expert Group. Donatella Pascolini kindly assisted in retrieval of some unpublished data sources. Gretchen Stevens was responsible for the statistical analysis.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
-
RRAB and JBJ share the first authorship.
-
GAS, SR and HRT share the senior authorship.
-
Collaborators Group information: A list of the Vision Loss Expert Group members appears at http://www.anglia.ac.uk/ruskin/en/home/microsites/veru/other_research_areas/global_burden_of_diseases.html.
-
Contributors All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, and gave final approval of the version to be published. RRAB, JBJ, SR and HRT were responsible for drafting the article or revising it critically for important intellectual content.
-
Funding This study was partially funded by the Bill & Melinda Gates Foundation, Fight for Sight, Fred Hollows Foundation and the Brien Holden Vision Institute. The results in this paper are prepared independently of the final estimates of the Global Burden of Diseases, Injuries, and Risk Factors study. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
-
Provenance and peer review Not commissioned; externally peer reviewed.