Article Text

Abstract
Background Flash visual evoked potentials (VEPs) were abnormal in a cohort of 100 neonates exposed to maintenance methadone in utero. This prospective cohort study now describes clinical visual and electrophysiological outcomes at 6 months.
Methods Visual assessment included modified Atkinson test battery; strabismus, nystagmus, reduced visual acuity, delayed visual maturation or refractive error (>3 dioptres) defined a fail. Pattern-onset VEPs were recorded to 120′, 60′ and 15′ checks.
Results 81 drug-exposed and 26 comparison infants (79% and 52% of the original cohorts) were assessed at a median age of 27 weeks (range 26–30). 90% of drug-exposed infants had been additionally exposed to illicit drugs and 41% to excess alcohol in utero. 40% of the drug-exposed cohort failed clinical visual assessment: the relative risk of abnormal assessment was 5.1 (95% CI 1.3 to 20; p=0.02). Nystagmus was particularly common. VEP peak times were slower and amplitudes smaller in drug-exposed infants, of whom 70% had one or more abnormal VEP parameter. Abnormal visual outcome at 6 months was not associated with the pattern of additional drug exposure or a history of neonatal abstinence.
Conclusions Abnormal visual electrophysiology in infants born to drug-misusing mothers prescribed maintenance methadone persists to 6 months of age, and is associated with abnormal clinical visual assessment.
- Child Health (Paediatrics)
- Drugs
- Electrophysiology
Statistics from Altmetric.com
Introduction
Illicit drug use in pregnancy is a significant medical and social problem with an estimated 250 000–350 000 children of known problem drug users currently living in the UK.1 Management of maternal opioid misuse includes prescription of maintenance methadone, a synthetic opioid which stabilises lifestyle, lessens risk-taking behaviour and reduces the incidence of preterm birth and intrauterine growth restriction (IUGR).2–4
There is increasing evidence that maternal drug misuse during pregnancy has adverse effects on infant visual outcome.5–10 Reported visual abnormalities include nystagmus, strabismus, reduced visual acuity, delayed visual maturation (DVM), impaired voluntary eye movements and absent binocular vision5–10 but the majority of studies published to date have been small and confounded by the effects of IUGR and social deprivation.5–9 Visual evoked potentials (VEPs) can be used to assess the maturity and integrity of the visual system even in relatively uncooperative infants11 and in a prospective cohort study of 100 infants exposed to maintenance methadone in utero we demonstrated abnormal flash VEPs in the newborn period compared with non-exposed infants matched for birth weight and social deprivation.12 The objectives of this study were to describe the clinical visual outcomes and pattern VEPs at 6 months of age in this cohort.
Methods
This prospective cohort study was conducted at the Princess Royal Maternity in Glasgow. Eligible infants were recruited within the first 3 days of life from drug-misusing mothers prescribed substitute methadone during pregnancy, and were born between October 2008 and April 2010.12 Exclusion criteria were birth before 36 completed weeks of gestation, congenital ocular abnormality and/or significant neonatal illness. For comparative purposes, healthy, non-maternal drug-exposed infants were recruited from the postnatal wards of the same maternity unit. To correct for any potential confounding effect of birth weight, gestation or socio-economic status, the comparison infants were matched as follows: completed week of gestation, birth weight ±250 g and socio-economic group deprivation index score (DEPCAT) ±1.12 Data collected in the neonatal period included maternal and neonatal demographics and the incidence and severity of neonatal abstinence syndrome (NAS). Details regarding study size are given in the paper describing neonatal outcomes from this cohort.12 Infants underwent twice daily assessment for NAS by trained midwifery staff and were scored using a modified Lipsitz score.12 NAS was defined as symptoms severe enough to require pharmacological treatment as defined by local protocol. Ethics approval was obtained prior to study commencement and informed written parental consent obtained for all participants.
Drug exposure and toxicology
A confidential maternal interview was conducted immediately after study recruitment regarding drug use during pregnancy (LMcG). Maternal urine samples were collected routinely at the first antenatal hospital visit, usually at 12–16 weeks gestation, and infant urine and meconium were obtained as soon as possible after delivery. Maternal and infant urine samples were analysed using enzyme multiplied immunoassay technique assays run to Substance Abuse and Mental Health Services Administration guidelines on an Abbott Architect Analyser.13 Assays included methadone, opioids, benzodiazepines, amphetamines, cannabinoids and cocaine metabolites. Meconium samples were analysed in the Department of Forensic Medicine and Science at the University of Glasgow using ELISA screening plus solid phase and liquid–liquid extraction followed by GC-mass spectrometry (MS) and LC-MS-MS for selected positives.13 Infants were classified into one of five drug exposure groups (table 1); meconium samples were also analysed for fatty acid ethyl esters (FAEEs) to identify infants exposed to excess alcohol in utero. A cut-off value of >10 000 ng/g of meconium was used to signify excess alcohol consumption in pregnancy.14
Drug exposure group based on history and toxicology
Six-month assessment
All infants were invited for evaluation at 6 months of age, undertaken jointly by a paediatrician (LMcG) and one of two experienced optometrists. The latter was blinded to the infant's group and clinical course. Follow-up assessment included: measurement of weight and occiptofrontal circumference (OFC); clinical visual assessment; and pattern-onset VEPs. Clinical visual assessment was undertaken using a modification of the Atkinson test battery of child development for examining functional vision.15 The Atkinson battery is a series of visual tests providing an integrated assessment of infant and children's functional visual capacities drawn from practice in ophthalmology, orthoptics and developmental psychology. It provides normative data for various age groups and pass/fail criteria for each test, allowing normal visual development to be defined. Tests included: pupil response to light, diffuse light reaction, lateral tracking and observation for nystagmus, Hirshberg's test, lateral field testing by peripheral refixation, convergence of eyes to an approaching object, defensive blink to approaching object, visual following of a falling toy, batting and reaching, near (Mohindra) retinoscopy, dynamic retinoscopy and the Cardiff acuity card test based on fixation preference. Cardiff cards are used widely in UK orthoptic practice because the vanishing optotype design gives high success rates in difficult-to-test groups, and acuities agree well with grating tests.16 Normative Cardiff acuity data show binocular acuities of 0.3–1.0 logMAR (Snellen 6/12–6/60) in 6-month-old children.16 Cardiff cards use vertical fixation preference; consequently, horizontal nystagmus does not confound the visual acuity measurement. Non-cycloplegic near retinoscopy was used to screen for media opacities and refractive errors. Retinoscopy reflexes were neutralised with handheld lenses in a dark room.17 In addition, the amplitude of accommodation was assessed with dynamic retinoscopy in a dim room using an accommodative fixation target.18 Infants were classified as ‘pass’, ‘fail’ or ‘borderline’: those with a fail or borderline assessment were referred to a paediatric ophthalmologist. A fail was defined as the presence of strabismus, nystagmus, reduced visual acuity or a refractive error of greater than 3 dioptres which was later confirmed on cycloplegic refraction and required correction with glasses. Visual acuity from the comparison group was used to define normal acuity for this age group: median acuity was 0.70 logMAR, with a range of 0.50–0.90 logMAR (Snellen 6/30, range 6/19–6/48). The poorest visual acuity, 0.90 logMAR (Snellen 6/48), was defined as the lower limit of normal. A borderline assessment was defined as minor visual abnormalities, refractive error which could not be confirmed by an ophthalmologist due to failure to attend following referral or moderate refractive error confirmed by an ophthalmologist, but not prescribed glasses and remaining under follow-up. DVM was diagnosed retrospectively in infants who had absent visual responses from birth then subsequently developed normal visual behaviour in the first 6 months of life.
VEPs were recorded from the occipital scalp using silver-silver-chloride electrodes placed according to international standards.19 An Espion visual electrophysiology system (Diagnosys LLC, Lowell, Massachusetts, USA) was used to generate stimuli and record VEPs. Stimuli were black and white checkerboard onsets with check widths of 15′, 60′ and 120′ alternating with a diffuse grey background of equal luminance and colour presented at one reversal per second. Six-month-old infants with normal vision were expected to demonstrate a VEP to the smallest (15′) check size. Between 30 and 100 trials were acquired; this was repeated for each check size to assess reproducibility. All VEPs were independently assessed by an observer (RH) blinded to the infant's group and clinical course. VEPs were categorised as present or absent: if present, the amplitudes and peak times of the major peak of the onset VEPs (C2) were measured. Absent VEPs were accorded amplitudes of zero and a worst peak time to avoid favourable group bias by elimination (rounded up to the nearest 10 ms from the longest peak time when a peak was present). Normal limits were defined using 95% reference intervals of the parameters measured from the comparison infants’ onset VEPs.
Statistics
Categorical outcomes were compared between groups using χ2 tests or Fisher's exact tests where numbers were small. Numerical data were tested for normality using Anderson–Darling tests and found to be of skewed distribution; comparisons between groups were therefore done with Mann–Whitney tests and comparisons between subgroups done with Kruskall–Wallis tests with Dunnet's post hoc test comparisons. Logistic regression models were used to correct for the potential confounding effect of alcohol exposure on visual outcomes.
Results
A total of 107 infants were seen for assessment at 6 months of age: 81 drug-exposed infants and 26 comparison infants. This represented 79% and 52% respectively of the cohorts recruited at birth. Details of the neonatal outcomes of this cohort have been reported previously.12 Reasons for non-attendance included: parent/carer uncontactable (56%), did not attend a prearranged appointment on two or more occasions (24%), geographically unable to attend (7%) and declined follow-up participation (13%).
The birth demographic characteristics of those comparison infants who did not attend for follow-up did not differ from those of infants who were followed up: birth weight (two-sample t test p=0.45), OFC (two-sample t test p=0.71), gestation (Mann–Whitney test p=0.98), 5-min Apgar score (Mann–Whitney test p=0.26) and DEPCAT score (Mann–Whitney test p=0.26).
Median age at follow-up was 27 weeks (range 26–30) for both drug-exposed and comparison groups. Mean weight and head circumference at the 6-month follow-up were slightly less in the drug-exposed infants, but the differences were not significant: weight 7.52 kg (SD 1.05) versus 7.94 kg (SD 1.09) (comparison infants), two-sample t test p=0.11; head circumference 43.3 cm (SD 1.5) versus 43.8 cm (SD 1.9) (comparison infants), two-sample t test p=0.15.
Drug and alcohol exposure
The majority of the methadone-exposed infants (73/81; 90%) had also been exposed to illicit drugs in utero including opioids (75%), benzodiazepines (67%), cannabis (64%) and stimulants (26%). In all, 20 out of 46 infants tested (43%) and seen at 6 months of age had elevated FAEEs in meconium indicative of exposure to excess alcohol in utero.
Three comparison infants (3/18 tested, 17%) had elevated FAEEs in meconium and two infants’ samples tested positive for cannabis. No infant had a clinical diagnosis of fetal alcohol syndrome.
Visual assessment
Overall, 32 (40%) of the drug-exposed cohort failed the visual assessment (table 2). All infants had visual acuity measured in a standardised way and we were confident that any motor or developmental abnormalities did not interfere with this. Horizontal nystagmus was present in nine of the drug-exposed cohort (11%); it was manifest in five infants, and in four infants nystagmus had a latent component with associated strabismus (also known as fusion maldevelopment nystagmus syndrome). One of these nine infants with nystagmus had no opioid exposure other than methadone (study # 155) and one had no benzodiazepine exposure (study # 40). Strabismus was detected in 20 drug-exposed infants (25%) of whom 12 infants had an exotropia and eight had an esotropia. Reduced visual acuity (>0.90 logMAR) was detected in 18 drug-exposed infants (22%) and associated with other ophthalmic abnormalities in 11 of these infants. Confirmed DVM was present in two infants and presumed in eight infants (a history of visual inattentiveness given by the parents/carers).
In utero drug exposure, neonatal VEP finding and visual findings at 6 months for the 32 drug-exposed infants who failed the visual assessment
After correcting for excess in utero alcohol exposure using a logistic regression model, significantly more drug-exposed infants failed the visual assessment than comparison infants: 32/81 versus 2/26; p=0.007. The relative risk of an abnormal visual assessment in drug-exposed infants was 5.1 (95% CI 1.3 to 20, p=0.02) giving an attributable risk of 80%. There was no association between a failed 6-month visual assessment and NAS: χ2 test; p=0.239. There was no significant difference in the proportion of drug-exposed infants in each of the five different drug exposure groups who failed the visual assessment: χ2 test; p=0.528.
A further nine drug-exposed infants (11%) fulfilled criteria for borderline visual assessment; these were infants with refractive errors not assessed by an ophthalmologist (two infants), moderate refractive errors not prescribed glasses (three infants), exophoria (two infants), anisocoria (one infant) and absent blink response (one infant). Two infants (8%) in the comparison group failed the visual assessment: one infant had an intermittent esotropia and one had a refractive error.
VEPs
VEPs were recorded from 105/107 infants at 6 months of age (79 cases, 26 comparisons) (figure 1). VEPs to all three check sizes were present from all comparison infants. Three of the 79 (4%) drug-exposed infants had no VEP to 60′ checks (figure 2). The visual acuities in these three infants were 0.70, 1.20 and 1.92 logMAR (normal range 0.50–0.90 logMAR); two of these infants also had nystagmus (study # 61, 10 and 155, table 2). Overall, 19 drug-exposed infants (27%) had non-detectable VEP to 15′ checks (figure 2). Acuities of infants with absent 15′ VEPs did not differ significantly from those with 15′ VEPs present (medians of 0.80 vs 0.70 logMAR, Mann–Whitney U test, p=0.9). Two infants with absent 15′ VEPs had nystagmus (study # 147 and 14, table 2). The difference between drug-exposed infants and comparison infants with regard to the likelihood of having a VEP to the smallest (15′) check size was highly significant (51/70 vs 24/24, Fisher's exact test p=0.006).

Typical pattern-onset visual evoked potentials (VEPs) to each of the check sizes from comparison infants (top) and drug-exposed infants (bottom). The VEPs illustrated have parameters most closely matching the medians for each check size and group.

Comparison of presence of pattern-onset visual evoked potentials between cases and comparison infants. Error bars show the 95% CI of the proportion.
Drug-exposed infants had median VEP peak times 16, 9 and 20 ms slower than those of the comparison infants to 120′, 60′ and 15′ checks, respectively, and median VEP amplitudes were 2, 10 and 7 µV smaller to 120′, 60′ and 15′ checks, respectively (table 3, figure 3).
Pattern-onset VEPs: cases and comparisons

Pattern-onset visual evoked potential (VEP) data for cases (open circles) and comparison infants (grey circles). For each infant, C2 amplitude is plotted versus C2 peak time. Grey lines indicate the upper 97.5 centiles (peak times) and lower 2.5 centiles (amplitudes) of VEPs from comparison infants. Non-detectable VEPs are illustrated on the x-axis at zero amplitude and 210 ms.
Comparison infants’ VEPs were used to define limits of normality: an absent response to any check size was classified as abnormal and upper 97.5 centile VEP peak times and lower 2.5 centile VEP amplitudes were used as normative cut-off values (figure 3). Using these definitions, 19/67 (28%), 38/77 (49%) and 26/70 (37%) of drug-exposed infants had abnormal 120′, 60′ and 15′ VEPs, respectively. Overall, 55/79 (70%) drug-exposed infants had one or more abnormal VEP parameter.
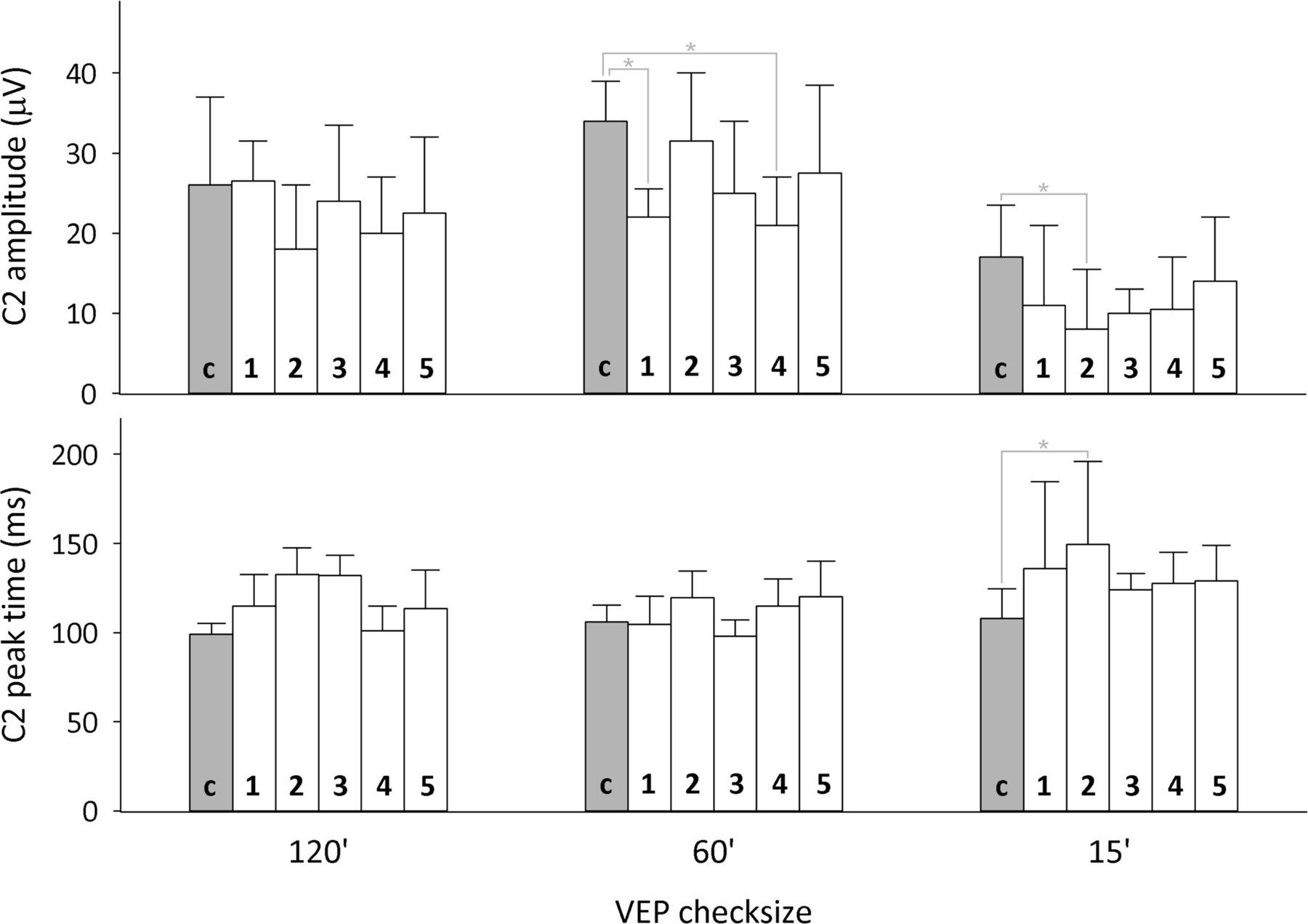
VEP parameters were compared between infants in the five different drug exposure groups with the comparison infants added as a sixth group. Group differences existed for 60′ VEP amplitude, 15′ VEP amplitude and 15′ peak time (Kruskal–Wallis, p=0.03, p=0.03 and p=0.01, respectively). Post hoc Mann–Whitney comparisons with Bonferroni corrections revealed significant differences only between the comparison group and drug-exposed groups 1, 2 and 4 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Median pattern-onset visual evoked potential (VEP) data for each drug group (labelled 1–5) and for comparison infants (labelled c) are plotted for each check size. Amplitudes are shown in the upper panel and peak times in the lower panel. Error bars are median absolute deviations. Significant group differences are indicated with an asterisk. Absent VEPs from cases are treated as having amplitudes of 0 µV and C2 peak times of 210 ms for 60′ (N=3) and for 15′ check sizes (N=19).
VEP abnormalities were no more common in infants who had developed NAS (24/41) than those who did not (31/40) (Fisher exact test, p=0.1), nor did group median amplitudes or latencies differ between those drug-exposed infants who had developed NAS and those who did not.
Discussion
Substitute methadone is currently the recommended treatment for pregnant opioid-dependent women,1 ,4 with advantages for mother and baby including stabilisation of maternal lifestyle and reduced incidence of IUGR.2–4 The disadvantages of methadone use during pregnancy include an increased incidence of NAS3 ,4 and likely detrimental effects upon infant visual development.5–9 ,12 The latter has been reported only relatively recently, mostly in small case series, and has not been properly quantified to date.5–7 ,9 ,12 This follow-up study of 81 maternal drug-exposed infants is the first cohort study to have comprehensively assessed visual development in infancy and to have been able to explore associations between specific in utero drug and alcohol exposure and early infant visual development.
The most common abnormalities detected were strabismus (25%), reduced visual acuity (22%) and nystagmus (11%) and the fivefold increased risk of failing the 6-month visual assessment for drug-exposed infants persisted after correcting for excess alcohol exposure in utero. The prevalence of strabismus is 2.1% in 3-year-old children,20 10-fold lower than in our drug-exposed group. Nystagmus is rare in the general population with an estimated incidence of 0.24% in the UK.21 The majority of nystagmus cases in early infancy are associated with visual impairment, neurological or retinal disease and the incidence of idiopathic infantile nystagmus extremely low at only 1.9 cases per 10 000 population (0.019%). In general, nystagmus presenting in an infant before 6 months of age is mainly due to congenital idiopathic nystagmus or anterior visual pathway abnormalities. Both sensory deprivation (eg, due to bilateral cataracts or macular maldevelopment) and abnormality of the optic nerve or chiasm will generate nystagmus due to reduced vision. Posterior visual pathway abnormalities do not tend to be associated with nystagmus. It should be noted however that population estimates of nystagmus do not capture cases of fusion maldevelopment nystagmus syndrome if the nystagmus is latent (present only with uniocular viewing).21 Even after excluding cases with latent nystagmus the incidence of manifest infantile nystagmus in infants exposed to methadone and/or other substances of abuse in utero was 300-fold higher than in the general population. We found no association between visual outcome and the pattern of drug exposure in utero, suggesting that all drug-exposed infants are at risk although the common factor in all these cases was in utero methadone exposure. Comprehensive toxicology indicated that only eight of the 81 cases were exposed to methadone alone, two of whom failed the visual assessment (study # 56 and 92, table 2). These data are too few to determine whether methadone alone might cause visual abnormalities.
The fact that VEP abnormalities previously reported in the newborn period persisted to 6 months of age in conjunction with clinical visual abnormalities suggests a teratogenic effect of prenatal drug exposure on the developing visual system. It is unlikely that absent or abnormal VEPs resulted from reduced acuity with the pattern stimulus beyond the infant's resolution threshold, as acuities did not differ between those infants with absent or present VEPs to the smallest checks. Furthermore, drug-exposed infants’ VEPs—when present—demonstrated smaller and slower peaks than those of the comparison infants. Although nystagmus alters the pattern VEP, the choice of pattern-onset VEPs rather than pattern-reversal VEPs is likely to have minimised this effect.22 It appears therefore that the VEP abnormalities noted are not a direct consequence of reduced acuity, and that in utero drug exposure has altered the functioning of visual pathways and/or cerebral sources of VEPs.
The high prevalence of strabismus, coupled with the preponderance of fusion maldevelopment nystagmus, suggests that affected infants have impaired development of binocular fusion.23 Loss of binocular connections within striate cortex (area V1) causes fusion maldevelopment nystagmus,24 and could explain the smaller neonatal VEPs seen in the current drug-exposed cohort shortly after birth.12 Binocular vision was absent in 42% of a similar cohort of drug-exposed children at 5 years of age,9 and further follow-up of the current cohort will investigate binocular vision.
Strengths of this study include the large sample size, the prospective nature of data collection and the comprehensive pattern of drug exposure obtained. This is especially relevant as the majority of studies investigating longer-term outcomes in infants exposed to drug misuse in utero rely on retrospective collection of drug exposure data. Objective assessment of excess in utero alcohol exposure, via meconium FAEE analysis, allowed us to correct for any potential confounding effect of alcohol exposure on visual and developmental outcomes. The optometrist undertaking the visual assessment and medical physicist analysing the VEPs were blinded to the infant's drug exposure and neonatal course, thus minimising any bias in interpretation of results. The extensive toxicology undertaken during pregnancy and in the newborn period meant that each infant's drug exposure could be accurately defined, reducing the errors inherent in maternal history taking. The bias of loss to follow-up was minimised by the high retention rate of drug-exposed infants; although there was a higher loss to follow-up of comparison infants, there were no significant differences in demographic characteristics between those comparison infants who were followed up and those who could not be followed up. The incidence of visual abnormalities described in our comparison population is very similar to that described in larger populations,20 ,21 supporting the validity of our testing techniques. Drug-exposed and comparison infants were not significantly different in terms of sex, gestation, weight and OFC at 6 months of age, thus excluding the confounding effects of preterm birth and IUGR. It is possible that our comparison group were at a higher risk of visual abnormalities than the general infant population due to the history of maternal social deprivation, smoking and alcohol consumption in pregnancy. This may have had an effect of underestimating the degree of visual system damage in the drug-exposed population.
We propose a cause–effect relationship between in utero drug exposure and infant visual abnormalities, which is supported by the strength of association (relative risk 5.1).25 A cause–effect relationship is also biologically credible: several animal studies have demonstrated a detrimental effect of prenatal methadone exposure on cerebral neurotransmitters and nerve growth factor which could have an adverse effect on early visual processing.26–28 Our findings are also consistent with other published studies in the literature, using different methods, geographic settings and populations.5 ,6 ,9 Assuming this causal effect of in utero drug exposure, over 80% of clinical visual abnormalities could be potentially eliminated if infants were not prenatally exposed.
Buprenorphine is a synthetic opiate, which has been shown to be an effective intervention for use in the maintenance treatment of heroin dependence.29 It has theoretical advantages over methadone in the treatment of opiate addiction in pregnancy due to reduced placental transfer, ceiling effect at higher doses and lesser withdrawal symptoms. Published data on the use of buprenorphine in pregnancy suggest a good safety profile and reduced length of hospital stay and duration of treatment for NAS compared with methadone maintenance.30 There is some evidence to suggest a potential advantage for buprenorphine in terms of infant neural development:31 Whitham et al described pattern-reversal VEPs recorded at 4 months of age in infants who had been exposed to methadone or buprenorphine in utero compared with control infants and found that the methadone-exposed infants had significantly delayed latencies compared with both buprenorphine-exposed infants and controls. Possible explanations for this include differing effects on embryonic neurotransmitter systems and differing placental transfer of the two drugs.
In summary, infants born to drug-misusing mothers prescribed maintenance methadone during pregnancy are at increased risk of visual problems in infancy, particularly fusion maldevelopment nystagmus syndrome, strabismus and reduced visual acuity. Early visual assessment should be undertaken for all infants born to drug-misusing mothers, although the optimal timing of this assessment is not clear. Future studies should investigate alternatives to methadone for maintenance treatment of pregnant opiate-dependent women. Studies comparing maintenance methadone versus maintenance buprenorphine for pregnant opiate-dependent women must take into account comprehensive long-term visual outcomes for the infant.
Acknowledgments
We wish to thank Gail Cooper, Huda Hassan and Bill Borland for analysing the toxicology samples for this study. We are grateful to Angie Groundland and Michelle McIntosh for performing the visual assessments. We also wish to thank Mr Richard Boulton for his help with VEP recordings and data management.
References
Footnotes
-
Contributors LMcG was involved in study design, recruited all patients, collected samples and data, undertook assessments, analysed results and drafted the manuscript. RH and DLMcC were involved in study conception and design, analysis and interpretation of data and drafting/revising the manuscript. JMacK and MB were involved in study conception and design and revising the manuscript. HM was involved in study design, interpretation of data and revising the manuscript. All authors have approved the final version of the manuscript and revised manuscript.
-
Funding Yorkhill Children's Charity (formerly the Yorkhill Children's Foundation), Tenovus Scotland.
-
Competing interests None.
-
Ethics approval West of Scotland research ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.