Article Text

Abstract
Background/objective In patients with conjunctival melanomas, surgery is the first choice of treatment, but no standard adjuvant therapy has been established. In this study, we evaluated prognostic factors for conjunctival melanoma in ethnic Chinese patients.
Methods Demographic data, known (published) prognostic factors, BRAF and KIT gene mutations, treatment strategies and outcomes were reviewed in 53 patients with pathologically confirmed conjunctival melanomas. Univariate and multivariate analyses of factors associated with survival were performed by the Kaplan–Meier method and a Cox proportional hazard model, respectively.
Results Univariate analyses for 50 patients in whom data were available showed that a higher T stage (p=0.041), greater tumour thickness (p=0.006), local resection (p=0.033) and no adjuvant therapy (p=0.006) were associated with a worse recurrence-free survival (RFS) and metastasis-free survival (MFS). Patients with more involved quadrants also had worse MFS (p=0.039), while a higher T stage (p<0.001), local resection (p=0.008), and no adjuvant therapy (p=0.028) were associated with worse overall survival (OS). However, BRAF or KIT mutations showed no correlations with RFS, MFS or OS. Patients who received high-dose interferon (HDI) adjuvant therapy had a better RFS (p=0.004), MFS (p=0.001) and OS (p=0.005) than those who did not. Multivariate analysis showed that adjuvant therapy and tumour thickness were significant predictive factors for RFS, and the T stage was a significant predictive factor for OS.
Conclusions Adjuvant therapy and tumour thickness are significantly associated with RFS and T stage is a significant predictor of OS in Chinese patients with conjunctival melanomas. Patients may benefit from adjuvant therapy with HDI.
- Neoplasia
- Conjunctiva
Statistics from Altmetric.com
Introduction
Conjunctival melanoma, a malignancy arising from melanocytes located in the basal layer of the conjunctival epithelium, accounts for 5–7% of all primary ocular melanomas.1 ,2 In recent years, the incidence of conjunctival melanoma has been found to be increasing.3 Early diagnosis of conjunctival melanoma is essential because therapeutic interventions can be curative in the early stages. The current therapeutic strategy for conjunctival melanoma is surgical excision of the tumour either alone or in combination with adjuvant therapy, including radiation, cryotherapy, chemotherapy and interferon,4–7 although the optimal choice of adjuvant therapy remains to be established.
Known (published) prognostic factors for conjunctival melanoma include distinct tumour locations such as the non-bulbar conjunctiva (palpebral conjunctiva, fornices, caruncle), increased tumour thickness, local tumour recurrence, a high mitotic rate, epithelioid cells and lymphatic invasion.8–10 However, most remain controversial, except for tumour location and thickness.
In the US, conjunctival melanomas almost occur exclusively in white people and African Americans account for less than 1% of cases,11 which means that racial differences may lead to different features and outcomes. Partly due to the rarity of the disease in Asia, the currently available literature on conjunctival melanomas in Asian patients is relatively limited.
The aim of the present study was to undertake a retrospective analysis of the prognostic factors for conjunctival melanoma in ethnic Chinese patients with pathologically confirmed disease by documenting the clinical presentation and the outcome of active treatments. In recent years, knowledge of genetic mutations underlying ocular melanomas has grown, and it has been reported that BRAF and KIT gene mutations in conjunctival melanoma may play a role in the development of the disease.12–14 Therefore, BRAF and KIT gene mutations were also included in the analysis of prognostic factors in this study.
Methods
Data resource
Known (published) prognostic factors and the demographic data of patients with pathologically confirmed conjunctival melanomas, including their characteristics, treatment and follow-up, were retrieved from the database of the Beijing Cancer Hospital (BCH), which is the largest melanoma centre in China. The design and establishment of this database have been described in a previous article.15 Acquisition and analysis of the patient data were only undertaken following approval of the study by the Institutional Review Board of BCH.
When the patients were first seen at BCH, their tumour tissue samples were analysed for mutations in exons 9, 11, 13, 17 and 18 of the KIT gene, and exons 11 and 15 of the BRAF gene in genomic DNA by PCR amplification and Sanger sequencing, as described previously by Si et al16 and Kong et al17 in studies performed at our centre. The BRAF and KIT gene mutation statuses were recorded and included in the BCH database, and were subsequently retrieved for the present analysis of prognostic factors.
Patients and staging evaluation
The American Joint Committee on Cancer (AJCC) staging system for conjunctival melanoma (7th edition) was used for either clinical or pathological staging.10
Data analysis
The patients’ recurrence-free survival (RFS), metastasis-free survival (MFS) and overall survival (OS) were calculated by the Kaplan–Meier method. RFS was defined as the time from the end of surgery until a documented local recurrence. MFS was defined as the time from the end of surgery until a documented distant metastasis. OS was calculated from the date of the pathological diagnosis of melanoma until death or the date of the last follow-up visit for patients still alive.
A Mantel–Cox log-rank test stratified by each factor was applied to compare the Kaplan–Meier curves for survival. Multivariate analyses of prognostic factors for OS, RFS and MFS were performed using a Cox proportional hazard model. Variables with a p value <0.10 in the univariate analyses were included in the multivariate analysis.
Results
Patient characteristics
The records of 53 patients with conjunctival melanomas who were treated at our centre from January 2006 to April 2014 were retrieved from the BCH database and reviewed. The characteristics of patients are shown in table 1.
Characteristics of the patients (at diagnosis) and their clinical outcomes
Disease staging
There were 16 patients (30%) with T1 disease (bulbar lesions), 30 patients with T2 disease (palpebral, forniceal or caruncular lesions) and 13% (n=7) with T3 disease. None of the tumours exhibited central nervous system invasion (stage T4).
At the time of diagnosis, local lymph node metastasis (N1 stage) was found in one patient (2%) and distant metastases were seen in two (4%). Both of the latter patients had liver metastases (100%) and one also had a lung metastasis (50%).
Tumour thickness and quadrants involved
Three subgroups were divided according to the thickness of the primary tumour. Twenty-one (40%) presented with tumours ≤0.5 mm thick, 22 (42%) with tumours >0.5–1.5 mm thick and 10 (18%) with tumours >1.5 mm thick. The numbers of patients with primary conjunctival melanomas distributed in 1, 2, 3 and 4 quadrants of the affected eye were 21 (40%), 28 (53%), 4 (7%) and 0 (0%), respectively.
BRAF and KIT gene mutations
KIT gene mutations were detected in the tumour tissue samples of 6 patients (11%), but were not found in the other 47 patients (89%). One of the six patients with KIT gene mutations had a D496N mutation in exon 9, one had a G565E mutation in exon 11, one had a H630H mutation in exon 13, one had a L656R mutation in exon 17, one had a L862L mutation in exon 18, and one had an E583E mutation in exon 11 and a R830stop mutation in exon 18.
BRAF V600E mutations in exon 15 were detected in 4 patients (8%), but were not found in the other 49 patients (92%).
Treatment of the primary disease
All except three patients (two with distant metastases and one with local lymph node metastasis) underwent complete resection of their conjunctival melanomas; 23 (46%) had an extended excision and 27 (54%) had a local excision. Among the three patients who did not undergo surgery for their primary tumours, one with stage M1 disease was found to have a BRAF V600E mutation and received treatment with a BRAF inhibitor (vemurafenib), while two received chemotherapy.
Adjuvant therapy
Among the 50 patients who underwent resection of their tumours, 30 (60%) received adjuvant therapy, including 3 with radiation (2 had radioactive plaque brachytherapy and 1 had stereotactic radiotherapy), 9 with chemotherapy (dacarbazine or temozolomide based regimens) and 18 with high-dose interferon-α2b (HDI) treatment (15 MIU/m2/day intravenously 5 days per week for 4 weeks, then 9 MIU/m2 subcutaneously three times per week for 48 weeks). The patients made the choice to receive or not receive HDI adjuvant therapy themselves based on their own comprehensive assessments of the adverse effects of interferon, its costs, and the convenience of treatment.
Clinical outcomes
The median follow-up time for the entire group of patients was 37 months (range 3–101 months). In total, 16 (30%) patients developed recurrent disease and 24 (45%) developed metastases during the follow-up period. The most common sites of metastases were the lung (11 patients), skin (7), liver (4), bone (3), brain (2), distant lymph node (2) and spleen (1).
Recurrences and metastasis status according to TNM stage, thickness and involved quadrants of melanoma, type of surgery, adjuvant therapy and gene mutation status are shown in table 1.
Survival analyses
The overall 5-year RFS, MFS and OS rates for all patients with conjunctival melanoma were 58.3%, 51.3%, and 65.5%, respectively, see table 2.
Analyses of 5-year RFS, MFS and OS rates and their correlation with the clinical characteristics of patients with conjunctival melanoma
Tumour thickness and survival
With the escalation of tumour thicknesses (from ≤0.5 mm to >0.5–1.5 mm and >1.5 mm), the 5-year RFS, MFS and OS rates decreased, but differences in the 5-year OS rates were not significant.
Involved quadrants and survival
For subgroups divided by the numbers (1, 2 or 3) of quadrants involved by melanoma, the differences in the 5-year RFS and OS rates were not significant, but the differences in the 5-year MFS rates were (58.7%, 52.4% and 0%, respectively; p=0.039) (table 2).
T stage and survival
With increasing T stages, the 5-year RFS, MFS and OS rates were all significantly decreased (RFS analysis: p=0.041; MFS analysis: p=0.028; OS analysis: p<0.001; see figure 1 and table 2).

Kaplan–Meier analyses of the recurrence-free survival (RFS), metastasis-free survival (MFS), and overall survival (OS) of patients with conjunctival melanoma according to the T stage (T1, T2, T3). (A) RFS (p=0.041); (B) MFS (p=0.028); (C) OS (p≤0.001).
Surgery and survival
The MFS rates of patients who underwent extended versus local resection were 69.4% versus 32.3% (p=0.061), while their 5-year RFS (78.3% vs 36.5%; p=0.033) and OS rates (84.8% vs 48.2%; p=0.008) were significantly different.
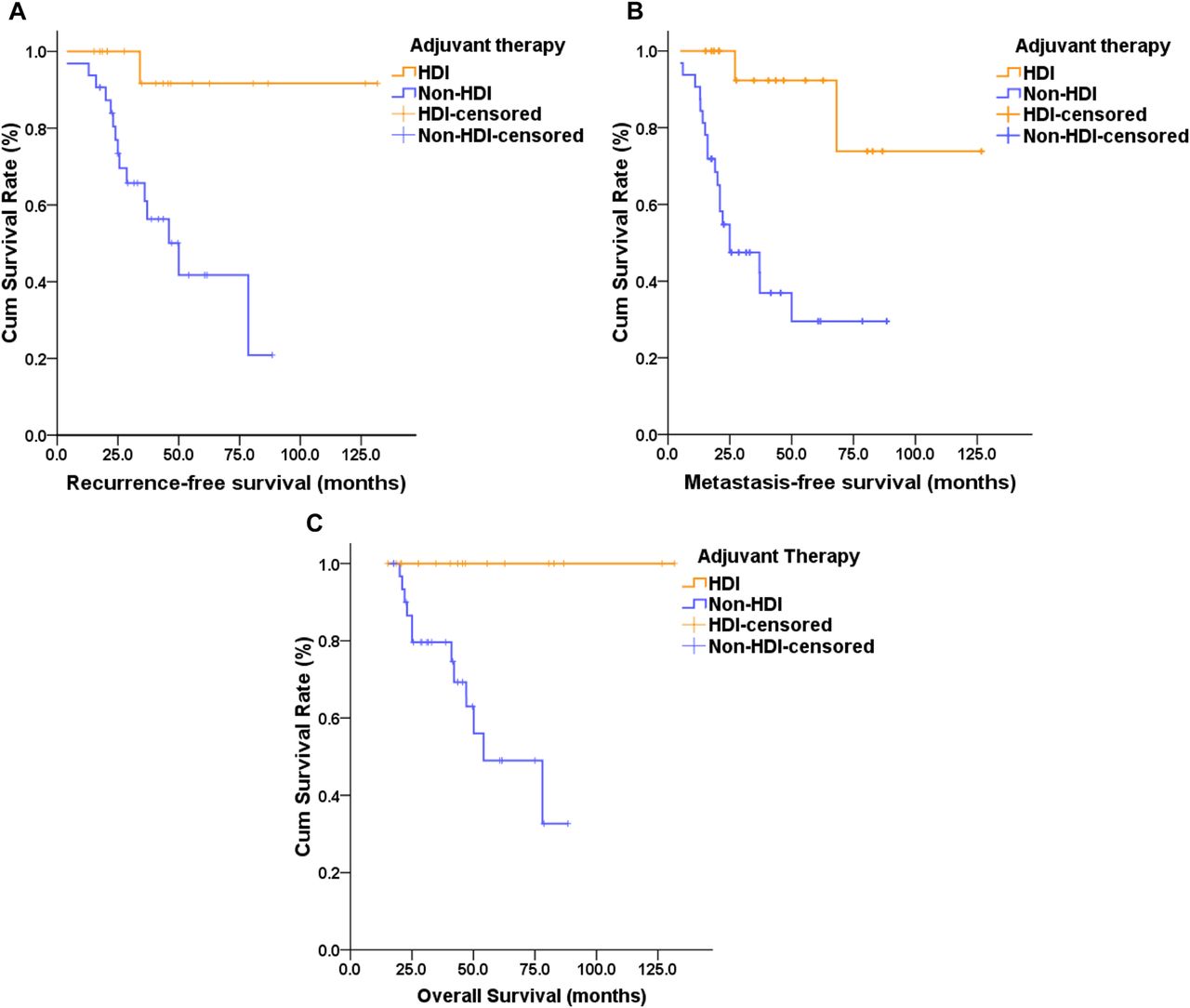
Adjuvant therapy and survival
Comparisons of the overall 5-year RFS, MFS and OS rates between patients who received the different types of adjuvant therapies showed significant differences (tables 2 and 3). Patients who received adjuvant therapy had higher 5-year RFS, MFS and OS rates than those who did not. Among them, the patients who received HDI therapy had significantly better survival than those who did not, whether for the 5-year RFS, MFS or OS rates (figure 2). The 5-year RFS rate in patients who received adjuvant chemotherapy was worse than for those who did not.
Impact of different adjuvant therapies on the 5-year RFS, MFS and OS rates of patients with conjunctival melanoma
{kind=link}
{kind=link}
Kaplan–Meier analyses of the recurrence-free survival (RFS), metastasis-free survival (MFS) and overall survival (OS) of patients with conjunctival melanoma according to whether they received adjuvant high-dose interferon (HDI) therapy or not (Non-HDI). (A) RFS (p=0.004); (B) MFS (p=0.001); (C) OS (p=0.005).
Survival analyses for age group, gender, BRAF or KIT mutation status, and the eye affected (left vs right) showed no significant value in predicting RFS, MFS and OS in the univariate analyses (table 2).
Prognostic factors
Potential prognostic factors for RFS, MFS and OS indicated by a significant value or a trend (p<0.10) in the univariate analyses described above were further analysed in a multivariate analysis to identify independent prognostic factors (table 4).
Multivariate analyses of prognostic factors for RFS, MFS and OS in patients with conjunctival melanoma
The results of this analysis showed that the thickness of the primary melanoma and postoperative adjuvant therapy were significant predictive factors for RFS, but the type of surgery, T stage and quadrants involved by the primary tumour had no significant prognostic value for RFS. While the T stage was a significant predictive factor for OS, the type of surgery and adjuvant therapy had no prognostic value for OS.
Discussion
The recurrence rate for conjunctival melanomas in this study was 30%, which is within the range of 23.5–62% reported in other published studies.18–20 However, the metastasis rate (45%) was higher than that reported by Yousef and Finger.21 Possibly, the higher proportion of tumours >0.5 mm thick in our study (60%) in comparison with the study of Yousef and Finger21 (45%) may have played some role in the higher metastasis rate. Alternatively, the limited knowledge of conjunctival melanomas in China may have resulted in later recognition and a delay in the diagnosis of the condition, leading to micrometastases in the circulation which eventually became the source of distant metastases. In a nationwide study of conjunctival melanoma in the Netherlands, Missotten and colleagues22 reported that the 5-year survival rate was 86.3%, which is higher than that (65.5%) in the present study. The higher metastasis rate and the higher proportion of tumours thicker than 0.5 mm may have contributed to the lower 5-year OS rate in our patients.
Since the release of the seventh edition of the AJCC staging system in 2010,10 other studies have demonstrated the predictive value of this staging system for conjunctival melanoma.20 Our multivariate analysis showing that the T stage and tumour thickness were independent prognostic factors for OS and RFS, respectively, of patients with conjunctival melanoma, and verified the value of the new staging system.
The surgical technique was a potential prognostic factor on the basis of the univariate analysis of the association between extended or local resection and the patients’ RFS and OS. The preferred surgical approach for management of conjunctival melanoma, as with most other malignant tumours, is total surgical excision.23 In the present study, several different surgical methods were used: removal of only the primary melanoma; ensuring a safety margin of 3–5 mm along with removal of the primary tumour; scleral/conjunctival resection after considering possible invasion of the corneoscleral limbus or sclera; and exenteration of the orbital contents in some patients with advanced disease (eg, deeply invasive and multifocal tumours). Due to the limited sample size of the study, we divided our patients into two groups for statistical conciseness. Patients who underwent methods 1 and 2 (above) were included in the 'local resection’ group, while those who underwent methods 3 and 4 were included in the ‘extended resection’ group. In general, the choice of extended or local resection depended on the anatomical positions of the primary melanoma, rather the surgeon's opinion. More than half of the patients (54%) underwent local resection, which may have contributed to the high metastasis rate and low 5-year survival rate in our patients. However, the surgical technique was not found to be a prognostic factor for RFS and OS in the multivariate analysis. This may be explained by the high proportion of patients with tumours >0.5 mm thick in our study, and the fact that advanced (eg, deeply invasive) cases often result in systemic spread, and extended resection in these cases, including exenteration of the orbital contents, has no effect on survival.19
To provide better local control and eradication of tumour cells, surgical excision is usually combined with adjuvant therapy, including radiation, cryotherapy and chemotherapy, but the optimal choice of adjuvant treatment remains to be established. In the current study, we found that radiation had no impact on RFS and MFS compared with no radiation, and chemotherapy was even associated with a worse RFS in these patients compared with no chemotherapy (see table 3). Because of the limited sample size of our study, the role of radiation and chemotherapy as adjuvant therapy needs to be demonstrated further.
Conjunctival melanomas are quite similar to cutaneous melanomas as regards clinical features, prognosis, treatment and genetics, which differentiate these melanomas from uveal melanomas.24 As interferon-α2b has been used successfully in the adjuvant treatment of cutaneous melanomas, it has been tried as adjuvant therapy in conjunctival melanomas and shown to be effective.5 In the present study, the 5-year RFS rate of the 18 patients who received HDI adjuvant therapy was significantly higher than in those who did not receive HDI (91.7% vs 41.7%; p=0.004). This finding has encouraged us to perform a prospective study of HDI as adjuvant therapy of conjunctival melanoma in the future.
In a recent study, BRAF mutations were identified in 23 of 78 (29%) conjunctival melanomas.24 In contrast, Kong et al17 found mutations of the KIT gene (receptor tyrosine kinase) in only 1 of 13 (7.7%) conjunctival melanomas in Chinese patients. In the present study, the mutation rates of BRAF and KIT genes were 8% and 11%, respectively. In addition to the small sample size of this study which may have influenced its findings, the current study showed that the BRAF and KIT mutation status had no impact on survival in terms of the patients’ RFS, MFS and OS, although they may play a role in the initiation of melanocytic tumours.14 Thus, further molecular biology investigations may be needed to help us better understand conjunctival melanoma.
We did not include the histological grade in this study for the following reasons. First, despite the once widespread use of the term primary acquired melanosis (PAM) in the literature, problems with this classification have been identified, including the fact that the classification itself is broad, the criteria are ambiguous, and the grades of atypia are subjective and show poor reproducibility. Second, according to the seventh edition of the AJCC T-staging system for conjunctival melanoma, melanoma in situ (including PAM) is staged as Tis, but there were no patients with Tis stage disease in our study (see table 1). Third, the postoperative pathological reports did not describe the histological classification, including de novo melanoma arising from PAM and/or naevus, for every patient in our study.
Finally, the limitations of this study also need to be recognised, including its small sample size which possibly introduced bias into the analysis of recurrences and metastatic events and the choice of treatments. In addition, other factors such as sentinel lymph node biopsy (SLNB) were not taken into account. SLNB may be of prognostic value in identifying micrometastatic disease, and the current indications for performing SLNB include a tumour thickness of ≥2.0 mm.25 Many of our patients (28.6%) had a tumour thickness ≥1.5 mm, but the micrometastatic status of these patients was unknown as SLNB has not been widely used in the management of conjunctival melanomas in China, although it is employed in several tertiary referral hospitals.
Conclusion
In patients with conjunctival melanomas, the T stage is an independent prognostic factor for OS, and the thickness of the primary tumour and adjuvant therapy are prognostic factors for RFS. Chinese patients may benefit from the use of adjuvant therapy with HDI which appears to reduce the risk of recurrences after surgery, but further prospective clinical trials of this adjuvant therapy will be necessary to confirm this finding. Although BRAF and KIT gene mutations were detected in the Chinese patients with conjunctival melanomas, the preliminary findings of this study suggest no correlation between the BRAF or KIT mutation status and patient survival.
Acknowledgments
We wish to thank Dr Wei Wen-bin, Beijing Tongren Eye Center, Beijing Tongren Hospital, Beijing, who provided valuable assistance in performing this study. We also thank Content Ed Net, Shanghai Co who provided editorial assistance with the manuscript.
References
Footnotes
XS and SL contributed equally to this work and are co-first authors.
Contributors XS and SL contributed equally to writing the manuscript and are the co-first authors. All authors participated in the study's design and in data collection, analysis, and interpretation. XS, SL and JG participated in editing and proofreading of the manuscript. All authors read and approved the final version for submission.
Funding This work was supported by grants from the National Natural Science Foundation of China (81172196, 81102068, 81272991), the Doctoral Fund of the Ministry of Education of China (20110001120070, 20120001110048), the Beijing Nova Program (Z121107002512042), and the Major State Basic Research Development Program of China (2013CB911004).
Competing interests None.
Ethics approval Approval for the study was obtained from the Institutional Review Board of Beijing Cancer Hospital prior to the acquisition and analysis of any patient data.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance