Article Text

Abstract
Purpose To assess Pentacam (Oculus, Wetzlar, Germany) Scheimpflug quantitative images in evaluating lens density and providing objective measurements to suggest optimal time of cataract surgery in the field of health examination.
Methods Two hundred and twenty-nine eyes with age-related cataract were enrolled. Lens density was measured using Pentacam. All Pentacam images were exported to ImageJ (NIH, Bethesda, Maryland, USA) for quantitative analysis. Average lens density (ALD) and nuclear lens density (NLD) were calculated. Lens density was also evaluated by built-in Pentacam Nucleus Staging (PNS) software. Slit-lamp microscopy was performed for cataract grading according to Lens Opacification Classification System III (LOCS III). The best-corrected visual acuity (BCVA) was measured. All measurements were compared between the cataract surgery and non-cataract surgery groups.
Results The measurements of Pentacam images significantly correlated with LOCS III for nuclear opalescence (NO) and nuclear colour (NC) grading (p<0.01). Pentacam ImageJ showed higher correlation than PNS. The mean NLD was most highly correlated with NO (r=0.8833) and NC (r=0.6815). The maximum ALD was most highly correlated with cortical opacity (r=0.5381). All Pentacam measurements of lens density and BCVA were significantly different between the cataract surgery and non-surgery groups (p<0.01). The optimised cut-off values to perform cataract surgery for mean NLD and maximum ALD were 26 and 74, respectively (p<0.01).
Conclusions The Pentacam ImageJ method provided objective measurements to evaluate cataracts needing surgery. The method has the potential to be generally applied in the field of health examination and is effective in screening patients with cataract.
- Imaging
- Lens and zonules
- Diagnostic tests/Investigation
- Public health
Statistics from Altmetric.com
Cataract classification systems have been created to characterise the different stages of cataracts, to guide surgical planning and to standardise cataract-related studies.1 As regular health examinations are becoming more common, the desire for the measurements available to monitor the development of cataracts, such as tumour marker, and to determine the proper time to perform cataract surgeries has been rising. As well known, the decision on whether to suggest cataract surgery depends on a number of considerations among which the increase of lens density is not the only and most important one. However, general doctors can counsel patients presenting with visual disability to visit ophthalmologists if objective measurements were applied in the field of health examination to provide lens density quantitatively.
The Lens Opacification Classification System III (LOCS III), which developed in 1993, is regarded as the standard grading system for evaluating cataract morphology and opacity.2 It consists of six slit-lamp images for grading nuclear colour (NC) and nuclear opalescence (NO), five retroillumination images for grading cortical cataract (C) and posterior subcapsular cataract.2 LOCS III has been validated and proven valuable in the previous clinical applications.1–4 However, it has several limitations inherent because it is a subjective method of assessing cataracts at slit-lamp examination or by standardised lens photographs. As with other subjective classification systems, concerns exist regarding observer bias and the reproducibility of within-observer and between-observer measurements.
Another widely studied method of cataract assessment is Scheimpflug imaging, based on the Scheimpflug principle that was first described over a century ago.5–7 Currently, new optical technologies such as Pentacam (Oculus, Wetzlar, Germany) acquire a total of 50 images in approximately 2 s by a rotating Scheimpflug camera measurement and offer objective images of the anterior segment structures including lens density evaluation.8 As to the measurement of lens density, the programme quantifies lens density on a scale of 0–100 (0=no cloudiness; 100=completely opaque lens) using the individual images. Peak values at one point of the lens nucleus of the individual image are measured, as well as mean and maximum densities. SD can be calculated automatically by the Pentacam lens densitometry programme for a specific area drawn on the Scheimpflug image. Pentacam Nucleus Staging (PNS), a built-in lens densitometry software, provides average and maximal lens density with a cataract grading score from 0 up to grade 5. The Pentacam Scheimpflug images can be exported to image analysis software like ImageJ (National Institutes of Health, Bethesda, Maryland, USA; available as a free download from http://rsb.info.nih.gov/ij/download.html, accessed 23 February 2012) as well, to analyse lens density.
So far, there has been no standardised principle of cataract evaluation by Pentacam Scheimpflug images in the literature. Peak values of the individual images, mean and maximum densities of selected areas, PNS values, and exported images to ImageJ software were used in previous reports.9–14 Herein, the current study was conducted to investigate the most strongly associated Pentacam Scheimpflug image measurements with LOCS III grading which is considered as a standard grading system clinically for cataract assessment. To the best of our knowledge, this is the first study to evaluate the agreement among the various Pentacam Scheimpflug image measurements including the PNS system and exported images to ImageJ software with LOCS III grading. Moreover, there is no previous study that has explored the validity of Pentacam Scheimpflug imaging as a tool for screening and grading measurement in patients with cataracts to determine whether cataract surgery is needed. Simply an accurate measurement of lens density might not be sufficient to make surgical decision for cataract; however, its use would be helpful in the field of preventive medicine because age-related cataract is a highly prevalent disease and the leading cause of reversible visual impairment and even blindness in the world.15 ,16
The purpose of the present study was to compare various Pentacam methods with LOCS III grading to diagnose cataracts and to investigate the usefulness of Pentacam Scheimpflug quantitative imaging of lens density in the field of health examination monitoring of cataract progression and determination of the optimal time for cataract surgery.
Patients and methods
From January 2012 to June 2012, 229 eyes from 229 patients with age-related cataracts with different degrees and types of cataract were enrolled in the study. All patients were Korean and had no previous ocular surgeries or laser treatments. Subjects with any history of ocular diseases other than age-related cataract were excluded. Ethics approval was obtained from the Samsung Medical Center Institutional Review Board and the current study was conducted in adherence with the Declaration of Helsinki. Patients underwent a standardised interview and ocular examination including logarithmic minimal angle resolution (logMAR) best-corrected visual acuity (BCVA) measurements. After maximal pupil dilation using topical 1% tropicamide and 2.5% phenylephrine HCl, lens density was evaluated by slit-lamp microscopic examination and the Pentacam device. Each measurement was defined as LOCS III, PNS or Pentacam ImageJ, and the following are the descriptions of each measurement in detail. Among the Pentacam Scheimpflug image measurements described above, automatically recorded peak densities of the individual images were not used in the analysis of the current study because the peak value of lens density was measured only at one point of the entire lens nucleus. Instead, the maximum value of PNS was considered to be sufficient to represent the peak density of the individual images. All images in the analysis were anonymised and rated in a randomised order.
Lens density assessment by LOCS III
Slit-lamp photography was taken with a digital slit-lamp camera (Topcon model SL-D7; Topcon, Tokyo, Japan). The slit beam was adjusted to completely fill the pupil and to vertically bisect the lens. The NO, NC and C of the slit-lamp photographs were assessed by a single trained grader (THK) at the Samsung Medical Center using the LOCS III based on a standardised protocol with standard lens photographs, together with a decimalised system. The scores ranged from 0.0 to 6.9 for NO and NC and 0.0 to 5.9 for C. Adjudication was provided for all images with positive findings for nuclear and cortical cataract by a senior ophthalmologist (DHL).
PNS measurements
Subsequently, the lens density was evaluated using the Pentacam device. All images were obtained in the same room for all patients with a consistent environment using the same device, after calibration of the equipment. The participant, with dilated pupil, sat in front of the Pentacam device and placed his or her chin on a chin rest. Next, the image of each eye was focused and centred manually. To reduce operator-dependent variables, the automatic release mode was used. Scheimpflug photography was taken and PNS measurements were automatically calculated (figure 1). The mean and maximum value of nuclear density ranged from 0 to 100, and grading score from 0 up to a grade 5 was recorded.

The image of Pentacam Nucleus Staging (PNS) measurement (PNS score=1; average Scheimpflug lens density=10.0%, maximum Scheimpflug lens density=41.2%).
Pentacam quantitative imaging analysis using ImageJ
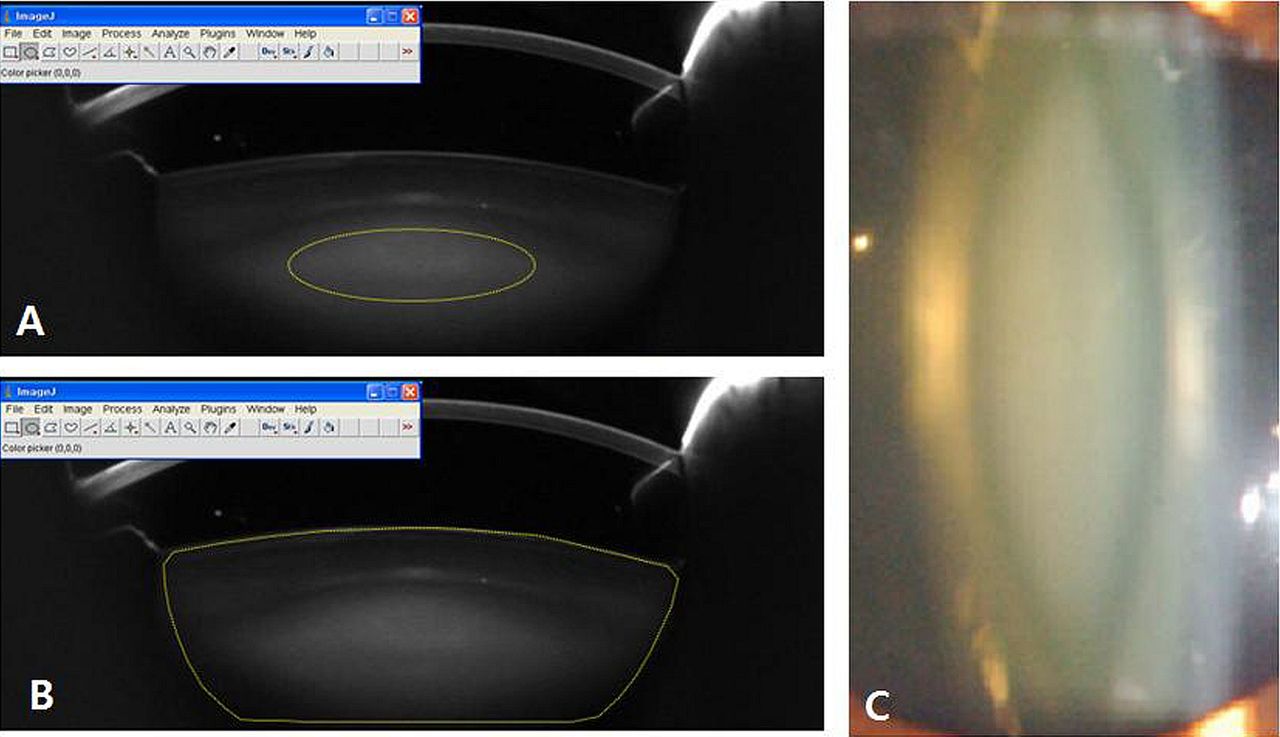
All Pentacam Scheimpflug images were exported to ImageJ software17 (National Institutes of Health) for quantitative analysis to obtain a homogenous comparison of overall lens density. The images were analysed according to a previously established method by Grewal et al.10 The nuclear lens density (NLD) was defined as the area covered by a standard elliptical mask to encompass as much of the lens nucleus as possible (figure 2A). A variable amount of outer nuclear shell was thus excluded from the portion of the nucleus sampled using this method. The average lens density (ALD) was calculated by marking the edges of the lens using the ImageJ software (figure 2B). The density of the selected area was measured in pixel intensity units on a scale of 0–255. Mean and maximum values of NLD and ALD were calculated.
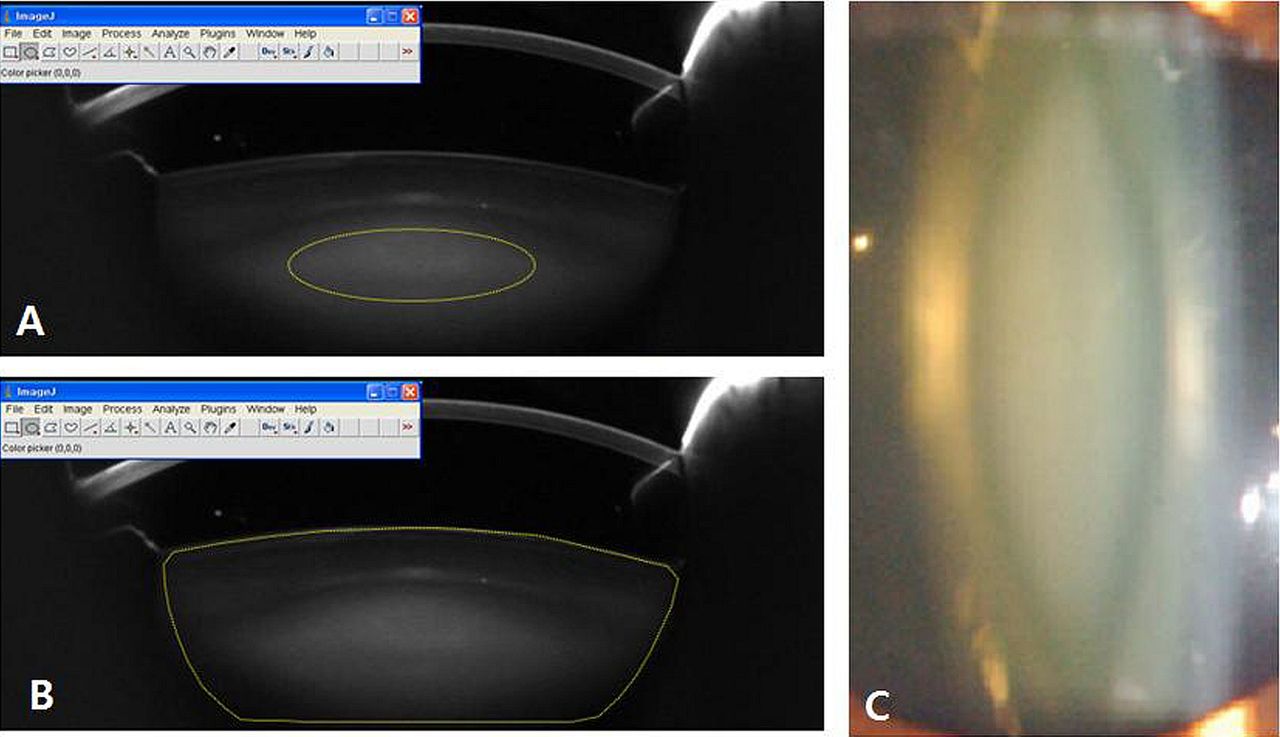
Scheimpflug image of the lens exported to ImageJ software for measuring the nuclear lens density marked by the elliptical mask (A), average lens density (B) and a digital slit-lamp photograph of the same lens (C).
Reproducibility of lens density assessment using Scheimpflug Images
For reproducibility testing, two consecutive images were captured from a subset of 30 eyes during the study. The interval among the measurements was 30 s, the time needed for the instrument to process the data, and each patient was asked to sit back and relax during the interval. Plots of the intraobserver differences against their mean values and the 95% limits of agreement (mean difference ±1.96 SD) were determined as suggested by Bland and Altman. Repeated measures analysis of variance (ANOVA) was performed, and intraclass correlation coefficient (ICC) and 95% CI were computed with SPSS software using the two-way mixed model and absolute agreement.
Comparison of lens density measurements between the cataract surgery group and the non-surgery group and establishing the cut-off values for cataract surgery
Whether cataract surgeries should be performed was decided by an independent, skilled surgeon (TYC) based on clinical diagnosis and ocular examinations at slit-lamp microscopy and funduscopy with BCVA measurement. The patients with complaints of decreased vision and visual disturbance such as blurred vision or monocular diplopia, which interferes with normal everyday functioning, were considered as candidates for cataract surgery. Preoperatively, the surgeon was masked to evaluate the results of the analysis for lens density according to the different measurements of LOCS III, PNS and Pentacam ImageJ. All surgeries were conducted in a way of phacoemulsification and posterior chamber intraocular lens implantation by the same experienced surgeon (TYC) using the same technique.
Another independent physician (DHL) compared all Pentacam Scheimpflug image measurements between cataract surgery and non-surgery groups and cut-off values were determined by a statistical analysis.
Statistical analysis
Statistical analysis was performed using SPSS V.18 (SPSS, Chicago, Illinois, USA). Statistical tests were performed at the 95% CI with p<0.05 being considered statistically significant. The correlation among lens density measurements by LOCS III, PNS, and Pentacam ImageJ was analysed using the Spearman correlation analysis with Bonferroni correction. The comparison between surgery group and non-surgery group was performed using the Wilcoxon rank-sum test. The Cochran–Armitage trend test and the χ2 test with Bonferroni correction were performed to evaluate the optimised cut-off values for each variable. To find cut-off values for surgery, all possible boundary values of lens density measurements were investigated between the top 10% and bottom 10%, and the measurements with minimum p values in the range between the averages of the two groups were selected as the best cut-off values.18
Results
The mean age of the subjects was 59.92±10.76 years (range, 34–85). There were 116 men and 113 women. Only one eye in each subject was selected randomly for the analysis. The baseline patient characteristics are described in table 1. The mean NO score was 3.3±1.6, mean NC score was 3.2±1.5 and mean C score was 2.5±1.6. The distribution of the LOCS III scores for the 229 eyes is shown in table 2. The mean ALD by Pentacam ImageJ was 29.66±15.93 and the mean NLD was 29.64±19.33 (pixel intensity units). The average mean density PNS was 11.67±3.87. The PNS and Pentacam ImageJ measurements corresponding to each LOCS III grading of NO, NC and C are provided as online supplementary tables A–C. The successive Pentacam measurements demonstrated an ICC of 0.985 (95% CI 0.968 to 0.993) for mean ALD, 0.984 (95% CI 0.967 to 0.993) for maximum ALD, 0.998 (95% CI 0.997 to 0.999) for mean NLD, 0.990 (95% CI 0.980 to 0.995) for maximum NLD, 0.985 (95% CI 0.957 to 0.995) for mean PNS and 0.984 (95% CI 0.967 to 0.992) for maximum PNS. The results of repeated measures ANOVA showed no statistically significant differences for all Pentacam variables (p>0.05).
Baseline patient characteristics including lens density by Lens Opacities Classification System III (LOCS III) scores, Pentacam Scheimpflug quantitative analysis using ImageJ software and the Pentacam Nucleus Staging (PNS) system (n=229)
Distribution of Lens Opacities Classification System III (LOCS III) scores (n=229)
All Pentacam measurements significantly correlated with LOCS III NO and NC grading, especially the mean NLD which was most highly correlated with NC and NO. The mean NLD correlated with NO grade (r=0.883; p<0.001) and NC grade (r=0.682; p<0.001) and mean ALD correlated with NO grade (r=0.770; p<0.001) and NC grade (r=0.629; p<0.001). The mean PNS value correlated with NO grade (r=0.722; p<0.001) and NC grade (r=0.584; p<0.001). Pentacam ImageJ measurements showed better correlation than PNS. Otherwise, the grade of cortical cataract was mostly correlated with maximum ALD (r=0.538; p<0.001). The correlation coefficients of Pentacam measurements with LOCS III variables, including NC, NO, C grade and logMAR BCVA, are presented in table 3.
Correlation coefficients (CC) of Pentacam measurements for lens density with Lens Opacities Classification System III (LOCS III) scales including nuclear opalescence (NO), nuclear colour (NC), cortical cataract (C) grade and logarithmic minimal angle resolution (logMAR) best-corrected visual acuity (BCVA)
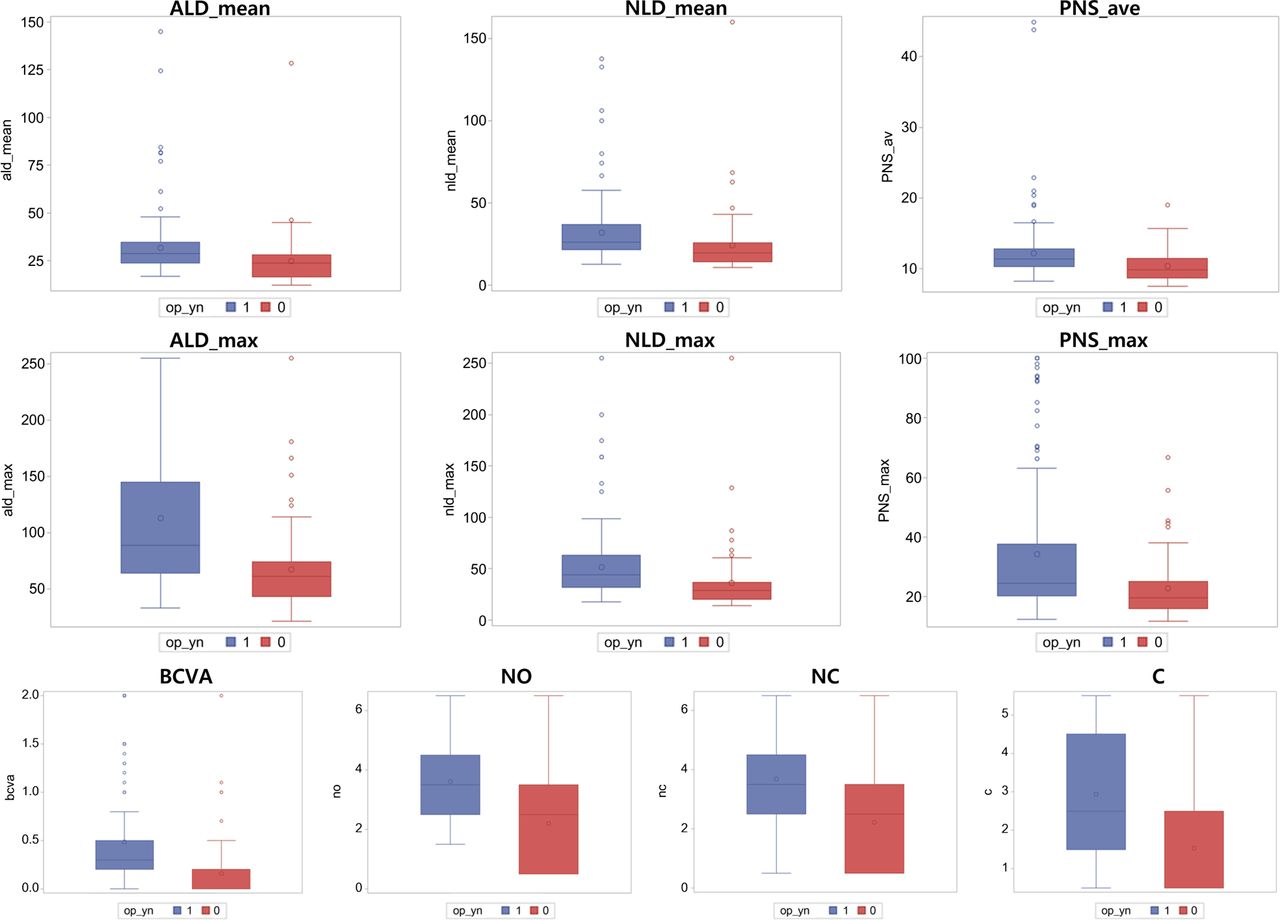
One hundred and sixty-two patients among the total 229 underwent cataract surgeries. In the subgroup analysis, BCVA and all Pentacam and LOCS III measurements were significantly different between cataract surgery and non-surgery groups (Wilcoxon rank-sum test, p<0.01). The optimised cut-off value was assessed by Cochran–Armitage trend test and χ2 test with Bonferroni correction (all p values <0.01). The cut-off value of mean NLD, which showed the highest correlations with NC and NO, was 26. Furthermore, the cut-off value of maximum ALD, which showed highest correlation with C, was 74. The differences in measurements between cataract surgery and non-surgery groups and optimised cut-off values are shown in table 4. The proportions of subjects above and below each threshold in table 4 to see how these thresholds separate subjects into surgery versus no surgery groups are presented as Box-Whisker plots in figure 3.
Differences in Pentacam measurements for lens density, visual acuity, and Lens Opacities Classification System III (LOCS III) grading between the cataract surgery group and the non-surgery group

{kind=link}
{kind=link}
{kind=link}
The proportions of subjects above and below each cut-off values in the cataract surgery group and the non-surgery group were presented as Box-Whisker plots (blue=cataract surgery group; red=no surgery group; top left=ALD_mean; top centre=NLD_mean; top right=PNS_ave; middle left=ALD_max; middle centre=NLD_max; middle right=PNS_max; bottom left=BCVA; bottom second=NO; bottom third=NC; bottom right=C). ALD_max, maximum value of average lens density; ALD_mean, mean value of average lens density; BCVA, best corrected visual acuity; C, cortical cataract; logMAR, logarithm of the minimum angle of resolution; NC, nuclear colour; NLD_max, maximum value of nuclear lens density; NLD_mean, mean value of nuclear lens density; NO, nuclear opalescence; PNS, Pentacam nucleus staging; PNS_ave, average value of Pentacam nucleus staging; PNS_max, maximum value of Pentacam nucleus staging.
Discussions
Cataracts are the leading cause of blindness and visual impairment worldwide, and the burden of cataract surgery is a major public health issue.19–22 The lack of objective measurements of lens opacity is an obstacle to conducting clinical studies on cataract formation and growth and to establishing the optimal time for cataract surgery.23 Although LOCS III has been validated in the previous clinical applications, concerns still exist because of its subjective property.1–4 When applying LOCS III to grading slit images with the LOCS III standard transparency, one must use the instrument settings described in the LOCS III instructions to secure usable photographs and make valid grading. However, to measure lens opacities according to strict LOCS III standards for grading is hard in the clinical setting and even in the research areas. A standardised grading system for cataracts is required to accurately reflect the severity of a cataract. Such a grading system would be especially useful in longitudinal studies on nuclear cataracts.
Furthermore, the rising demand for health examination has been a considerable factor. Ophthalmologists will make the final decisions whether the cataract surgery should be conducted or not on the basis of clinical criteria including patient expectation, symptoms or even economics. However, the significance of objective measurements to screen cataract cannot be denied. A standardised grading system may suggest a guideline to recommend visiting ophthalmologists for cataract check-up or treatment. Currently, the Pentacam rotating Scheimpflug imaging system provides measurements of lens density that are more objective, quantitative and obtainable than those achieved with LOCS III using a slit-lamp microscope independently of the examiner's skill.9–13 ,24 ,25
Pentacam imaging is rapid, simple to perform, relatively fast to learn and the procedure is more acceptable to patients. Several studies have validated the high intraobserver and interobserver repeatability and correlation with LOCS III scales of Pentacam Scheimpflug lens densitometry.9 ,10 ,25 Although the ordinal scale in LOCS III grading may be inadequate for detecting small changes in longitudinal studies, Pentacam Scheimpflug images can provide an evenly focused representation of a section of the lens and an objective measurement of lens density. In our studies, the measured nucleus density ranged from 0 to 255 units in Pentacam ImageJ and 0 to 100 in PNS measurements. With a more dynamic range and high measurement repeatability, it is conceivable that Pentacam may serve as a sensitive tool to detect longitudinal changes in lens density. Thus, Pentacam Scheimpflug images may be used for lens opacity assessment in large epidemiological studies, as well as, potentially, for mass screening for cataracts, for clinical trials evaluating potential preventive approaches for age-related cataracts and for precise nuclear cataract phenotypical definition in genetic research.26–29
As described above, the Pentacam Scheimpflug images show quantitatively measured lens density, including automatically calculated mean, maximum value and SD of nuclear density for selected areas by Pentacam lens densitometry programme, peak density at one point of the lens nucleus of an individual image and PNS measurements. The Pentacam Scheimpflug images can be exported to ImageJ software for analysis. However, these Pentacam measurements have not been uniformly standardised. Pei et al9 adapted automatically recorded Pentacam peak values of lens density to determine their correlation with LOCS III grading. They claimed that the peak value of each individual image may be considered as a representative index of the whole nucleus because nuclear opacity is likely to be homogenous and it is reasonable to suppose that visual impairment in nuclear cataract patients is most likely dependent on the opacity of the central nucleus rather than mean opacity. The peak value and the mean value of the lens density were useful in demonstrating changes in a nuclear cataract, but not in cortical or posterior subcapsular cataracts.30
In contrast, Grewal et al10 analysed the Pentacam Scheimpflug images exported to ImageJ software. They calculated the ALD and NLD and investigated their correlations with LOCS III grading. Magalhães et al14 used the peak value of Pentacam densitometry and PNS measurements to compare lens density with LOCS III grading and reported that PNS scores in the five stages showed great variability among the six LOCS III groups. Meanwhile, both the Pentacam lens densitometry programme and the PNS mean values were useful to evaluate age-related nuclear cataracts up to LOCS III grade 5, but not grade 6.
Nixon12 reported effective clinical application of PNS scores without adapting other mean or maximal values of Pentacam Scheimpflug images. They also found that preoperatively adjusted phaco parameters based on PNS scores helped improve overall efficiency by reducing the amount of energy and fluid used in the eye and reducing overall phaco time. Patrício et al13 studied the correlation between PNS grading and phaco time in phacoemulsification using peristaltic and venturi pumps. However, Kim et al11 applied mean lens density of Pentacam Scheimpflug images on phacodynamics in cataract surgery, rather than PNS scores.
The present study is the first report to compare different methods for evaluation of lens density among the different quantitative Pentacam Scheimpflug measurements. To the best of our knowledge, no studies exist that have looked specifically at Pentacam measurements of lens density and compared it with other methods of quantifying cataracts. In the current study, all Pentacam measurements, including ALD, NLD in Pentacam ImageJ and PNS, had significantly positive correlations with clinically used LOCS III grading, and the correlation was higher in the Pentacam ImageJ method with clinical availability although PNS measurements showed statistically significant correlations with LOCS III variables as well (table 3). Among the measurements, mean NLD was mostly related to NO and NC grade of LOCS III (r=0.883; p<0.001 and r=0.682; p<0.001, respectively), so that the variable has the potential to be used as a rather objective measurement of lens density. Because Pentacam measures white lens scatter through a greyscale Scheimpflug image, mean NLD is represented as a proxy for NO, rather than NC as a measure of colour. We demonstrated that the Pentacam ImageJ method is highly repeatable, has good agreement with the LOCS III method and correlated with clinical cataract assessment. Also, the mean NLD showed a stronger correlation to logMAR BCVA compared with other Pentacam variables.
It has been shown that the Pentacam measurements can detect nuclear cataracts, but not cortical cataracts.9 ,10 In our study, the maximum ALD showed the highest correlation with C grade of LOCS III (r=0.538; p<0.001), while other measurements showed relatively weak correlations. The lower correlation coefficient value in comparison with NO or NC can be explained by non-uniform distribution of cortical opacities in the lens. All cortical cataract manifest high polar asymmetry, and slit measure of ALD would be expected to vary significantly with the orientation of the slit beam.
Because nuclear and cortical cataracts are two of the most prevalent type of cataract in the aged population, Pentacam ImageJ measurements could have a significant impact in improving cataract screening.
From a clinical perspective, Pentacam lens densitometry measurements were applied in phacodynamics preoperatively for efficient cataract surgery.11–13 They evaluated the relationship between lens density measured using the Pentacam Scheimpflug imaging system and phacoemulsification time and energy. In the current study, we have compared various lens density measurements in the cataract surgery group and non-surgery group and analysed the results in the view of preventive medicine. The cut-off values were investigated for screening patients with cataract and determining timing of cataract surgeries. All variables calculated from Pentacam Scheimpflug quantitative image analysis were significantly different between cataract surgery and non-surgery groups (Wilcoxon rank-sum test, p<0.001). The cut-off values of mean NLD and maximum ALD, which were the representative variables for nuclear cataract and cortical cataract, were 26 and 74 (χ2 test with Bonferroni correction, p<0.01). They were assessed by subgroup analysis based on whether cataract surgery was done or not. These optimised cut-off values might be useful to provide screening guidelines in health promotion examinations although the cut-off values should be validated to be applied in the general population. As given the wide SD in table 4, the cut-off values are not very discriminatory although they showed statistical significant difference. A large cohort to examine sensitivity and specificity is required.
One of the limitations of the Pentacam Scheimpflug imaging system in practical use is that pupil dilation is required to maximise lens exposure. Any signals from behind the iris cannot be received by the Pentacam device. Further studies addressing whether Pentacam measurements in the not-dilated eyes are equivalent to the results from dilated eyes are required to ensure that Pentacam Scheimpflug images are practically used for mass screening.
Furthermore, measurements of lens density at the posterior cortex and posterior capsule could be difficult, even if the subject's pupil is completely dilated.31 The limitation may be particularly important in certain geographical area like India, in which the prevalence of posterior capsular cataract is high. Therefore, attention is required to recommend surgery which depends only on the Pentacam measurements. In the clinical practice, visual acuity assessment carries an important meaning. For sure, clinicians know that the decision to proceed with cataract surgery is based on several criteria, the most important of which is whether the patient is experiencing a significant amount of cataract-related visual disability. Lacking presentations or evidence of visual disability most surgeons would counsel patients to defer cataract surgery regardless of lens density measurements. The patients with posterior capsular cataract usually complain of severe visual impairments. We should counsel patients about visiting ophthalmologist with the possibility of posterior subcapsular cataract, even if the Pentacam measurements showed negative results. Using both Pentacam measurements and assessment of functional impairment through visual acuity measurement may help to screen patients with cataract more effectively and objectively. They should be complementary to screen cataract severity.
In the current study, we could not investigate the ability of Pentacam measurements to evaluate cataract progression because the data were obtained only once. The use of objective Pentacam measurements would be helpful in conducting researches on cataracts, particularly in longitudinal studies aiming to document nuclear cataract progression. Further studies estimating Pentacam ability to evaluate cataract progression will be in need.
In conclusion, the current study confirmed the strongest positive correlation between the lens density measurements taken by Pentacam ImageJ and LOCS III. The mean NLD of Pentacam ImageJ method showed mostly high correlations with NO and NC, and maximum ALD showed a high correlation with C. Furthermore, the Pentacam variables were significantly different between the cataract surgery group and the non-surgery group, and cut-off values were provided for use in screening patients and recommending cataract surgery in health examinations. Herein, the objective and repeatable Pentacam Scheimpflug measurements of lens density could allow this method to be used in research or studies on nuclear and cortical cataracts and may serve as a new paradigm to evaluate cataract density in clinical practice and in health promotion examinations to screen for cataracts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Presented at the meeting of the American Society of Cataract and Refractive Surgery (ASCRS) annual meeting, San Francisco, CA, USA, April 2013.
-
Contributors DHL and E-SC involved in conception and design; DHL, THK, T-YC and E-SC in conduct of the study; DHL and THK in collection, management and interpretation of data; DHL in data analysis and writing the article and DHL, T-YC and E-SC in preparation, review and approval of the manuscript.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Samsung Medical Center Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance