Article Text

Abstract
AIMS The aims of this study were to examine the influence of advanced recipient and donor age on the long term outcome of corneal transplantation.
METHODS Records of 1036 penetrating corneal grafts in recipients aged ⩾80 years at surgery (defined as the elderly subset) and 8092 donor corneas used for transplantation were obtained from the Australian Corneal Graft Register database. Kaplan–Meier graft survival plots were compared using log rank statistics.
RESULTS Elderly recipients constituted 15% of the recipient pool. The major indication for corneal transplantation in the elderly was bullous keratopathy. Graft survival fell with increasing recipient age (p < 0.00001); the major cause of graft failure was rejection (33%). The desired outcome in 51% of cases was to improve vision and in 42% of cases to relieve pain; 23% of elderly recipients achieved a Snellen acuity of 6/18 or better in the grafted eye and 66% recorded improved acuity after transplantation. Elderly recipients suffered more complications and comorbidities in the grafted eye than did younger recipients. Donor age (stratified in 10 year intervals) did not influence corneal graft survival significantly (p = 0.10).
CONCLUSIONS Elderly graft recipients fared less well after corneal transplantation than did younger recipients, but outcomes in terms of long term graft survival and visual rehabilitation were still good. Donor age did not affect graft survival.
- corneal transplantation
- recipient age
- donor age
- outcome
Statistics from Altmetric.com
In recent years, developments in anaesthesia and microsurgery have reduced the physiological stress and increased the predictability of corneal transplantation to a point where it can be offered to virtually everyone who might benefit. It is widely accepted that few geographic regions of the world have an excess of human corneas for transplantation,1 although concrete information on waiting lists for corneal transplantation is seldom published. Wherever patients are on waiting lists for surgery, the dual issues of fair allocation of donor corneas and of ethical methods of improving the number of donor corneas available for transplantation need to be addressed.23 Restriction of corneal transplantation to younger patients (who are possibly more likely to benefit from the procedure) and relaxation of age based criteria for donor selection may, in theory, alleviate some of the problems associated with insufficient donor supply.
Recipient age is seldom a barrier to corneal transplantation but the impact of age on outcome measures is undetermined. Age may potentially influence wound healing4 (although arguments have been mounted to the contrary5), immunological responsiveness,67 and the incidence of postoperative complications. Furthermore, successful corneal transplantation depends on patient cooperation and compliance with medication. The level of cooperation required may be difficult for older patients to achieve and this may be reflected in reduced graft survival. Finally, comorbidities may increase with increasing age, reducing the benefit that might otherwise be achieved though corneal transplantation.
Identification of an upper age limit for corneal donors is an important decision to be made in most eye banks. On the one hand, corneal endothelial cell loss is well known to occur with increasing age8 and some endothelial cell loss attendant upon corneal surgery is virtually inevitable.910 On the other hand, the substantial redundancy in endothelial cell number when compared with the number required to maintain stromal deturgescence means that many elderly corneas may function perfectly well.11
Using information collected prospectively into a large database of corneal grafts with follow up periods extending to 10 years, we sought to examine the long term results of corneal transplantation in elderly recipients. We investigated both Kaplan–Meier graft survival and visual outcome. Further, we examined the influence of increased donor age on long term graft outcome.
Methods
Grafts entered into the Australian Corneal Graft Registry are followed systematically and prospectively until the graft fails or the recipient dies or is lost to follow up. Graft survival, visual outcome, complications, and comorbidities are all recorded. Detailed descriptions of the operation of the registry have been published elsewhere.1213
PATIENT RECORDS
Information was available on a cohort of 7741 patients who had undergone penetrating corneal transplantation. The study period was 5 May 1985 to 14 May 1996 (11 years). In 1036 instances (13% of the cohort), the recipient was aged 80 years or more at the time of penetrating keratoplasty (hereafter referred to as the subset of elderly recipients). In the elderly recipient subset, 760 grafts had been followed on at least one occasion, 144 grafts had failed, 118 grafts had been lost to follow up, and in 114 instances the recipient had died. Data were also available on 8092 donor corneas used for penetrating and lamellar keratoplasty in the same time period.
DEFINITION OF CORNEAL GRAFT FAILURE
Any existing graft that was replaced by another in the same eye, irrespective of graft clarity and for whatever reason, was classified as a failed graft. An example in this category would be a clear graft with an unacceptably high degree of irregular astigmatism, not improved by refractive surgery, which was then replaced. In all other cases, graft failure was defined as oedema and irremediable loss of clarity in a previously thin, clear graft. The day of failure was the first day the patient was seen with an oedematous, opaque graft that subsequently failed to thin and clear. Rejection was defined as the development of a rejection line (epithelial or endothelial) or a unilateral anterior chamber reaction with corneal infiltrates and spreading corneal oedema in a previously thin, clear graft.
INDICATIONS, COMPLICATIONS, AND COMORBIDITIES
Presenting diseases, indications for graft, postoperative complications, and reasons for graft failure were coded using theICD.9.CM system (US Department of Health and Human Services). Any development with the potential to compromise graft outcome was considered to be a complication. Postoperative complications were collected in two ways. Firstly, a number of specified complications (for example, rise in intraocular pressure, fixed, dilated pupil, cataract, rejection episode, herpetic recurrence, early changes of bullous keratopathy), refractive and related errors (anisometropia, ⩾5 dioptres of astigmatism) and factors potentially affecting visual outcome but unrelated to the graft (cataract, aphakia, amblyopia, retinal detachment, cystoid macular oedema, or senile macular degeneration) were listed, requiring a yes/no answer. Secondly, contributors were asked to specify any other relevant complications, information, or departures from their preferred treatment.
STATISTICAL ANALYSIS
Kaplan–Meier survival plots14 were constructed usingspida version 6.05 (Macquarie University, Armadale, NSW, Australia). For surviving grafts, trial time was calculated as the number of days between the date of graft and the date on which the patient was last seen. For failed grafts, trial time was calculated as the number of days between the date of graft and the date of failure. Kaplan–Meier plots were compared using log rank analysis.1516
Results
RECIPIENT AGE AT GRAFT
Recipient age at graft in the total cohort of 7741 patients undergoing penetrating corneal transplantation ranged from 27 days to 97 years (Fig 1). The proportion of elderly corneal graft recipients (defined as those ⩾80 years at graft) within the total cohort rose slightly from 9–10% in 1985–9 to 15–16% in 1991–5 (Fig2).

Distribution of recipient ages at graft in a cohort of 7741 patients undergoing penetrating corneal transplantation. NR = not recorded.

Number of corneal grafts in elderly recipients aged ⩾80 years at the time of graft compared with those age <80 years, showing the influence of calendar years in which the grafts were performed.
INDICATIONS FOR PENETRATING TRANSPLANTATION IN THE ELDERLY
The indications for penetrating keratoplasty in the subset of elderly recipients are shown in Table 1; indications for graft in the entire recipient cohort are provided for comparison. Bullous keratopathy (83% pseudophakic and 17% aphakic) was relatively more important and keratoconus less important as an indication for graft in elderly recipients than for the cohort as a whole.
Indications for penetrating keratoplasty in recipients aged ⩾80 years compared with those aged <80 years at the time of graft
EFFECT OF RECIPIENT AGE ON CORNEAL GRAFT SURVIVAL
The influence of recipient age on penetrating corneal graft survival in the whole cohort is shown in Figure 3: graft survival fell with increasing recipient age (p < 0.00001). There were too few patients in the subset of recipients aged 80 years or more with keratoconus (Table 1) for a survival plot to be generated specifically for this group. However, when grafts performed for keratoconus were examined in the whole cohort, Kaplan–Meier graft survival for the various age groups (including a group of those aged over 60 years) ranged from 94–98%, values which did not differ significantly from each other (p = 0.51), data not shown. Kaplan–Meier graft survival plots stratified according to the most common indications for penetrating keratoplasty in elderly recipients are shown in Figure 4: 5 year graft survival was 63% for recipients grafted for pseudophakic bullous keratopathy, 52% for aphakic bullous keratopathy, 28% for previous failed graft, 87% for corneal scars and opacities, and 57% for all other indications for graft combined.

Kaplan–Meier corneal graft survival plots stratified according to recipient age at graft. For each curve, n = number initially at risk.

Kaplan–Meier graft survival plots in recipients aged ⩾80 years at graft, stratified according to the most common indications for transplantation in this subset. For each curve, n = number initially at risk. Scars = corneal scars and opacities; ABK = aphakic bullous keratopathy; PBK = pseudophakic bullous keratopathy.
The main reasons for corneal graft failure in the elderly subset were irreversible rejection (33%), endothelial cell failure (24%), infection (14%), or glaucoma (6%). In recipients younger than 80 years, the most important reasons were rejection (32%), endothelial cell failure (20%), infection (14%), and glaucoma (8%).
VISUAL OUTCOME AFTER CORNEAL TRANSPLANTATION
The desired outcome of transplantation for the subset of elderly recipients and for the cohort of all recipients is shown in Table 2. Relief of pain (with or without improvement in vision) was a relatively more important outcome than improvement in vision alone in elderly recipients, when compared with desired outcome in younger recipients.
Desired outcome after corneal transplantation in recipients aged ⩾80 years compared with those aged <80 years at the time of graft
Visual outcome at the time of last follow up for all recipients aged ⩾80 years at graft compared with data for the entire cohort is shown in Figure 5. Data were unavailable for 11% of elderly recipients and for 11% of younger recipients. In the subset of elderly recipients, 14% achieved a best corrected Snellen acuity of 6/12 or better, 23% achieved 6/18 or better and 24% achieved less than 6/60, compared with 46%, 54%, and 19% respectively for recipients aged less than 80 years at graft.

Snellen acuity at the time of most recent follow up for elderly corneal graft recipients (⩾80 years) and for younger recipients (<80 years). CF = counting fingers at 1 metre; HM = hand movements; LP = light perception; NLP = no light perception; NR= not recorded.
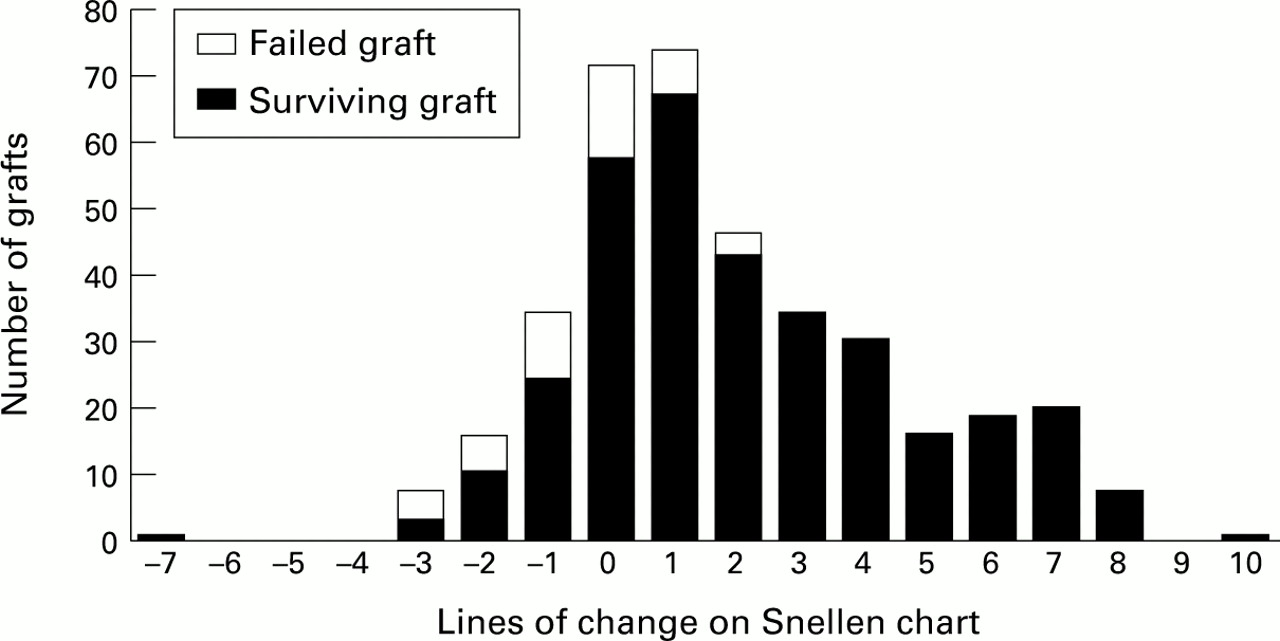
To determine whether any improvement in visual acuity had resulted from the transplant procedure, a comparison was made of preoperative Snellen acuity and the postoperative acuity at the time of most recent follow up. The number of lines of change in Snellen acuity after transplantation is shown in Figure 6; failed grafts in which acuity could not be expected to have improved are shown separately from surviving grafts. Overall, 34% of elderly recipients recorded no change in Snellen acuity or saw worse after graft, while 66% recorded one or more lines of improvement on the Snellen chart. These data compare with 19% and 81% respectively, in the cohort of patients aged less than 80 years.
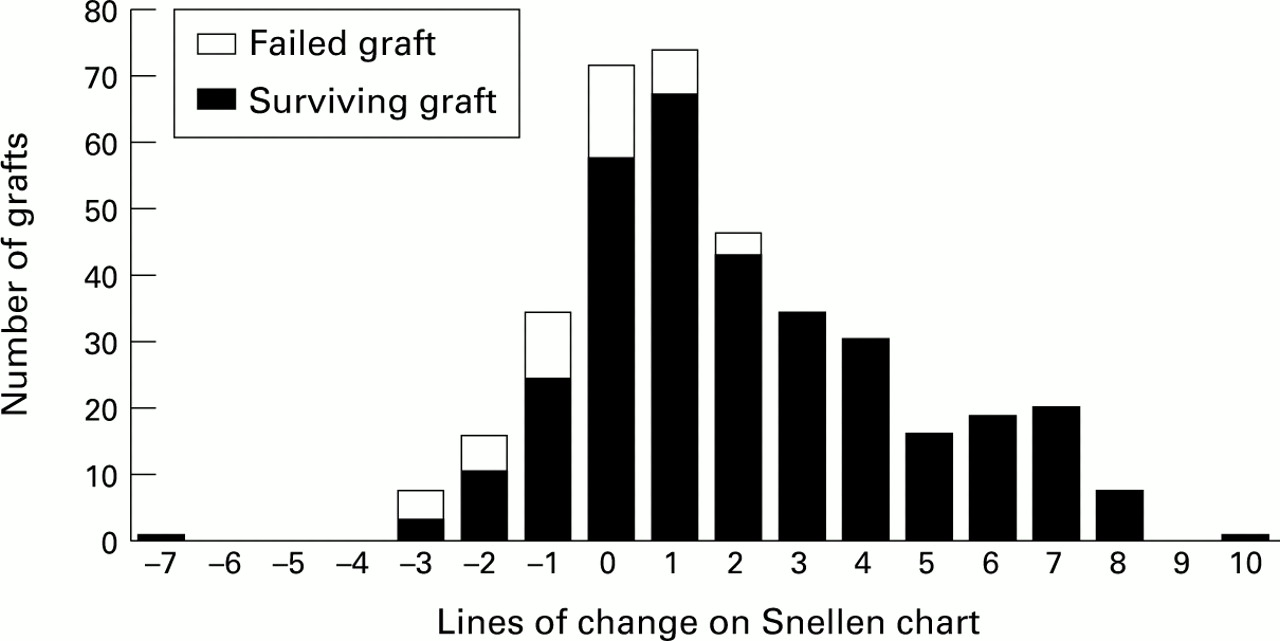
Number of lines of change on the Snellen chart at the time of most recent follow up, compared with Snellen acuity immediately before corneal transplantation, for elderly corneal graft recipients (⩾80 years).
COMPLICATIONS AND COMORBIDITIES AFFECTING VISUAL OUTCOME
Complications and comorbidities in the grafted eye assessed as having a negative influence on the visual potential of the grafted eye are shown in Table 3. Elderly patients suffered from more comorbidities than did younger recipients, with vision in one in four grafted eyes in the elderly subset being compromised by a retinal disorder.
Complications and comorbidities affecting the visual potential of the grafted eye in recipients aged ⩾80 years compared with those aged <80 years at the time of graft
INFLUENCE OF DONOR AGE ON CORNEAL GRAFT SURVIVAL
A histogram of age at the time of death for donors of corneas used for both penetrating and lamellar corneal grafts is shown in Figure 7. In 4% of cases, donor age was not reported. Donor age ranged from less than 1 year to over 90 years (median 64 years), with 66% of donors being in their sixth, seventh, or eighth decade and 6% being aged over 80 years at death. Only 2.5% of corneas were collected from multiorgan, brain dead donors but the median age for these donors was 39 years. Kaplan–Meier survival of penetrating corneal grafts stratified according to donor age (in 10 year intervals) is shown in Table 4: donor age exerted no significant effect on graft survival (p = 0.10).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of penetrating and lamellar corneal grafts performed using tissue from corneal donors of different ages, stratified in 10 year intervals. NR = not recorded.
Graft survival stratified according to donor age in 10 year intervals
Discussion
Recipients aged 80 years or more constitute an important subset of patients referred for corneal transplantation. Within our database, the proportion of elderly recipients undergoing surgery has increased over a 10 year period and now appears stable at 15–16%. The relative proportions of most indications for corneal transplantation are similar in older and younger recipients, except that bullous keratopathy becomes relatively more important, and keratoconus much less important, in elderly recipients.
Corneal graft survival falls significantly in recipients aged 60 or more years when compared with outcome in younger patients. However, there is no particular difference in survival between those aged 60–79 and those aged 80 years or more. Plainly, the indications for surgery are different in young and older graft recipients and this difference appears to account for most if not all of the difference in graft survival. Older patients tend to suffer from pseudophakic or aphakic bullous keratopathy, or a failed previous graft, indications which are acknowledged to compromise outcome at least when compared with keratoconus or the corneal dystrophies. Importantly, we found no significant effect of recipient age when first ipsilateral grafts for keratoconus were considered, and the survival of grafts performed for Fuchs’ dystrophy or corneal scarring in the elderly subset was excellent. These findings suggest that advanced recipient age is of itself no particular barrier to corneal graft survival.
The immune system deteriorates with increasing age,6 so one might expect irreversible rejection to be less of a problem in elderly recipients than in younger patients. This was not found to be the case and, in fact, the reasons for graft failure in the elderly were very similar to those operating in younger patients.
The desired outcome after corneal transplantation was certainly different for elderly graft recipients when compared with younger recipients. Not surprisingly, given the importance of bullous keratopathy as a major indication for transplantation in the elderly subset, relief of pain was a desired outcome in over 40% of cases. Improvement in vision was also an important desired outcome in the elderly, and in 66% of instances where both preoperative and postoperative Snellen acuities were available for comparison, at least some improvement in Snellen acuity was observed after corneal transplantation. However, less than 25% of elderly recipients achieved a best corrected Snellen acuity of 6/18 after graft, compared with over 50% in younger recipients. Part of the reason for the generally poorer acuity in older patients may lie with the finding that this subgroup suffers from more retinal comorbidities in the grafted eye than do younger recipients.
Some care is required when translating these findings to the clinical setting. Although graft survival may be decreased in older patients, so too is life expectancy. Further, the level of vision required may in many cases be less than that required by a younger person. Thus, a graft which survives 5 years and allows a reasonable degree of vision to be maintained in the absence of pain may materially help a patient for the remainder of his or her life. Our findings support the use of donor corneas in elderly recipients.
Recent studies have suggested that corneas from quite elderly donors may be acceptable for transplantation provided that corneal endothelial cell density and appearance are normal as judged by specular microscopy.17-19 We1213 and others2021 have previously shown no significant influence of increasing donor age on graft survival. Our current data are important primarily because we have examined long term graft survival within relatively small age ranges (intervals of a decade) in a large database and still failed to find a significant influence of donor age. That donor age does not influence graft survival at up to 10 years postoperatively encourages a widening of the criteria for donor suitability. Even very elderly donors may provide corneas which function long term without compromise.
Acknowledgments
This work was supported by: NH & MRC of Australia, AMHAC, the Ophthalmic Research Institute of Australia.
We gratefully acknowledge the voluntary contributions made by 405 ophthalmologists and other professionals to the Australian Corneal Graft Registry.
References
Linked Articles
- Editorial