Article Text

Abstract
AIM It appears from the literature that no standardised examination exists for patients with functional nasolacrimal duct obstruction. The role of dacryocystography and lacrimal scintigraphy was compared in the diagnosis and management of these patients.
METHOD Patients who were clinically diagnosed as having unilateral or bilateral functional nasolacrimal duct obstruction were prospectively entered into the study and data collected over 12 months in Moorfields Eye Hospital and Whipps Cross Hospital, London. All cases had, on separate occasions, a standardised dacryocystogram with delayed erect films and a lacrimal drainage scintigram.
RESULTS 45 lacrimal systems of 32 patients (mean age 62 years; 59% male) fulfilled the inclusion criteria. Abnormalities were detected with dacryocystography in 93% of systems and with lacrimal drainage scintigraphy in 95% of systems. Based on the results of previous quantitative studies, the positive scintigrams were subdivided into those demonstrating prelacrimal sac delay (13%), delay at the lacrimal sac/duct junction (35%), or delay within the duct (47%). Combining the two imaging techniques increased the sensitivity to 98%.
CONCLUSIONS Both investigations are very sensitive at detecting abnormalities in patients with a clinical diagnosis of functional nasolacrimal duct obstruction. Lacrimal drainage scintigraphy is a slightly more sensitive test, but missed an abnormality detected by dacryocystography in two (4%) systems. A combination of the two techniques gives the highest sensitivity with maximum anatomical and physiological information but, in clinical practice, it is reasonable to perform a dacryocystogram initially and proceed to scintigraphy only if contrast radiography is normal.
- dacryocystography
- lacrimal scintigraphy
- nasolacrimal duct obstruction
Statistics from Altmetric.com
Epiphora is a common condition in ophthalmological practice, and many cases are found clinically to have an obstruction of the nasolacrimal system. There is, however, a subgroup of symptomatic patients in whom an increased tear line is associated with patent lacrimal systems on syringing, a status termed “functional” nasolacrimal duct obstruction (FNLDO). It appears from the literature that no standardised approach exists in the examination of such cases.1 The simplest clinical tests are primary and secondary dye testing, which point to a functional block if the primary dye test is negative but the secondary dye test is positive.2 Additional diagnostic imaging may, however, help to clarify the cause of the obstruction and provide information for further management. Dacryocystography is considered extremely useful at demonstrating the anatomy of lacrimal systems,3 4 while lacrimal scintigraphy is generally deemed to be a more “physiological” test5-7 and therefore probably more likely to be abnormal in patients with FNLDO. We present a prospective study to evaluate and compare dacryocystography and lacrimal drainage scintigraphy for the investigation of patients with a clinical diagnosis of FNLDO.
Patients and methods
Thirty two patients who attended the oculoplastic and adnexal clinics at either Moorfields Eye Hospital or Whipps Cross Hospital with a clinical diagnosis of FNLDO in at least one eye were entered prospectively into the study. To fulfil the inclusion criteria, there had to be symptoms of epiphora, normal lid position, adequate puncta, no ocular surface disease, normal nasal examination, and patent lacrimal systems on syringing. Our technique for syringing involves the use of a topical anaesthetic before introducing a lacrimal cannula into the lower punctum; normal saline in a 2 ml syringe is irrigated and we regard the lacrimal system as freely patent if there is minimal regurgitation of fluid at the puncta and ready flow of fluid to the throat, which the patient confirms as saline.
Patients were subsequently investigated with a standardised dacryocystography and lacrimal drainage scintigraphy.
DACRYOCYSTOGRAPHY TECHNIQUE
With the patient supine, a drop of topical anaesthetic was placed into the palpebral aperture of both eyes. A control film was taken after intubation of both lower puncta with Portex intravenous cannulae (“Portex” limited, size 27FG) which were fixed 5 mm into the lower canalicular systems by taping; a Nettleship punctum dilator was used if necessary. A volume of 1–2 ml of an iodised oil based contrast medium (Lipiodol Ultrafluid; Mallinckrodt Medical UK Ltd), was injected simultaneously into both lacrimal systems and a series of macroradiographs taken. The patient was then sat upright for 5 minutes before a final erect oblique radiograph.
Functional nasolacrimal duct obstruction was diagnosed if there was poor emptying, such that residual contrast was present in the lacrimal sac or nasolacrimal duct of the delayed radiograph (Fig 1). Each dacryocystogram was also carefully evaluated, in a masked fashion, by an experienced observer (GER) to specifically look for and grade reflux from the upper canaliculus, measure the sac width (mm) and nasolacrimal duct calibre (mm), and comment on the presence of any filling defects or diverticuli. Finally, a subjective estimate was made for each abnormal dacryocystogram to determine whether the area of chief “hold up” was in the canalicular system, at the lacrimal sac/duct junction, or within the nasolacrimal duct.

Delayed erect radiograph demonstrating retained contrast in the right lacrimal system; the left system is normal.
A subgroup of 12 dacryocystograms (19 systems) were subsequently evaluated three more times on separate occasions in order to check for intraobserver variation.
LACRIMAL DRAINAGE SCINTIGRAPHY TECHNIQUE
This required the patient to be sitting upright in front of the pinhole collimator of an IGE Maxi 400ZS camera in Whipps Cross Hospital or an IGEStar cam camera with a hexagonal collimator in Guy’s Hospital (Moorfields’ patients). A drop of technetium-99m pertechnetate was placed into the inferior fornix of both eyes and the patient is requested to remain still, but to blink normally. A dynamic study is performed initially, with the tracer distribution imaged every 10 seconds for the first 160 seconds (Fig 2). Static views were then taken routinely at 5, 10, 15, and 20 minutes.

Normal lacrimating scintigram with rapid clearance of tracer in dynamic study (pictures at 10, 20, 90, and 100 seconds).
Quantitative studies, which involve plotting time-activity curves, have demonstrated large variations in the transit time for normal asymptomatic individuals.8 9 It is possible, however, to find broad agreement for the expected timing of certain stages of the lacrimal scintigram. Using this information the scintigrams were subdivided into three groups: those with “presac delay”, defined as hold up at the inner canthus or failure of the tracer to reach the lacrimal sac by the end of the dynamic study (Fig 3); “preductal delay”, with early filling of the lacrimal sac, but no sign of sac emptying on the first static image at 5 minutes (Figs 4A and B: right lacrimal system); “intraduct delay”, evidenced by nuclide in the upper part of the nasolacrimal duct at 5 minutes, but no further drainage over the next 15 minutes (Figs 4A and B: left lacrimal system).

Dynamic study showing system with “presac delay”.

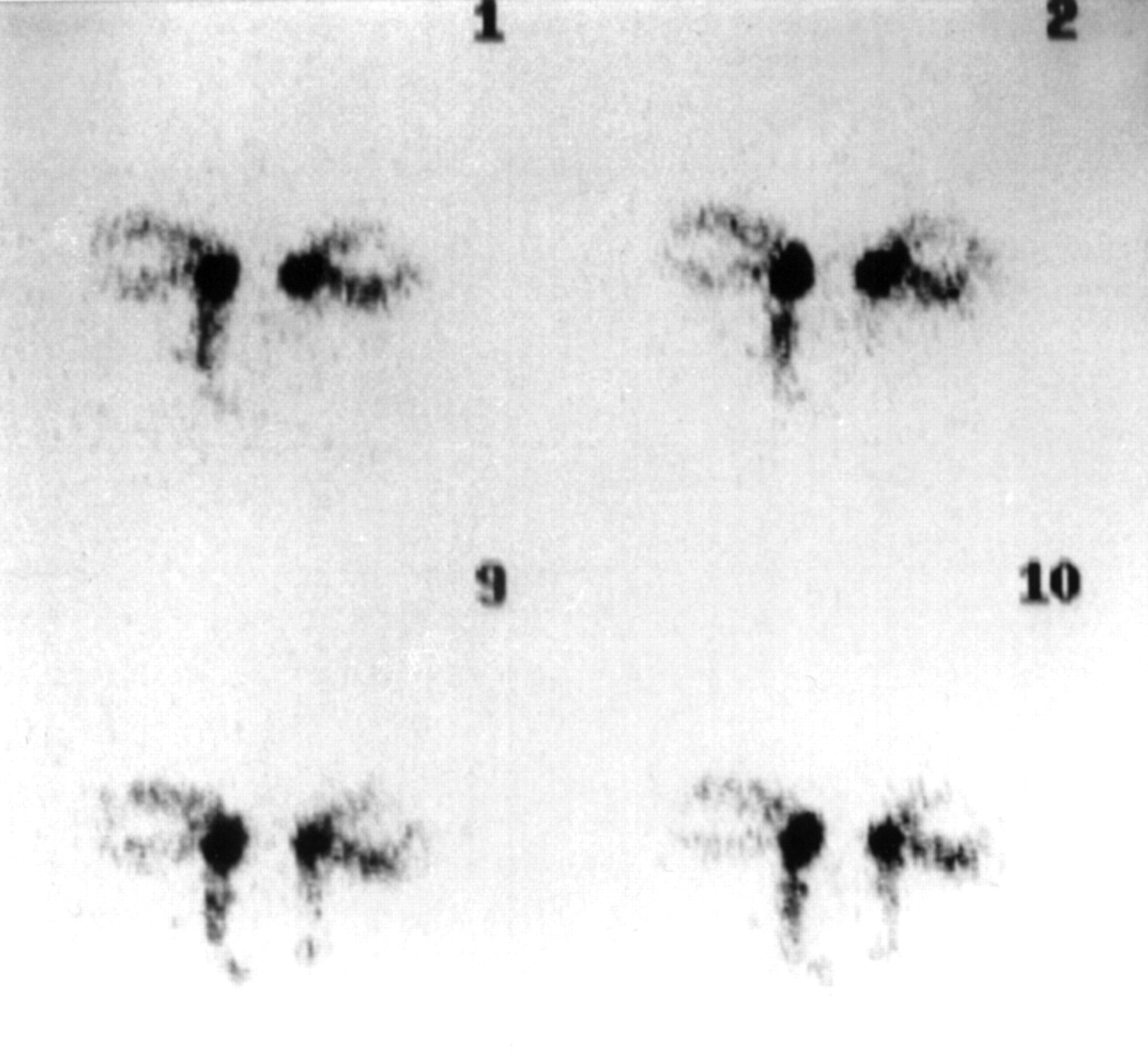
(A) Dynamic study with rapid entry of tracer into the lacrimal sac on the right and upper nasolacrimal duct on the left. (B) Static films (same patient as (A)) confirming “preductal delay” on the right and “intraduct delay” on the left.
The transit time through the distal part of the nasolacrimal duct and into the nasal space is extremely variable in normal individuals7 10 and was, therefore, not used in this study.
The results of the two investigations were analysed individually and then compared to look for the relation between various abnormal findings.
Results
Fifty five lacrimal systems in 32 patients (19 males, 13 females) fulfilled the inclusion criteria and were investigated using both imaging techniques, the mean age was 62 years (median 61) with a range of 33 to 88 years. Two patients (three systems) had previously had a three snip procedure for punctal stenosis and four patients (six systems) had undergone a successful lateral canthal sling for lower lid ectropion.
The sensitivity for the lacrimal drainage scintigraphy was 52 positive systems (95%) and for the dacryocystography 51 positive systems (93%) (Table 1). There were three systems (6%) which were considered abnormal on scintigraphy but normal on dacryocystography; interestingly, however, the dacryocystogram detected delayed clearance in two systems (4%) which were negative on scintigraphy. Both tests were negative together in only 1/55 systems and combining the investigations gives, therefore, a sensitivity of 98%.
Results of dacryocystography compared with lacrimal drainage scintigraphy in the investigation of functional nasolacrimal duct obstruction
Using our criteria, the abnormal lacrimal drainage scintigrams were further subdivided in order to try and differentiate between those with a failure of the upper lacrimal system and those with an abnormality or dysfunction of the nasolacrimal duct. Seven systems (13%) had prelacrimal sac delay, 19 (35%) had hold up at the sac/duct junction, and 26 systems (47%) were shown to have intraduct delay. Comparing the area of maximum hold up of radiographic contrast with the results of isotope scintigraphy (Fig 5), there was a 59% (29/49) agreement on the main area of hold up in systems where a block was detected using both investigations. In 33% (16/49) of systems the scintigram detected a block at a higher (more proximal) level in the lacrimal system: one “level” higher in 12 (25%) cases and two levels higher in four (8%) cases. In 8% (4/49) of systems the hold up on scintigraphy was lower (more distal) compared with dacryocystography.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graphic representation of main site of delay in dacryocystography and lacrimal scintigraphy.
Certain features of dacryocystography, found to have a low intraobserver variation, were compared with the lacrimal drainage scintigraphy results to look for more specific associations between the two investigations. No significant kappa (κ) agreement between tests was found, however, for reflux via the upper canaliculus (κ=0.4), nasolacrimal duct diameter (κ=0.5), or location of contrast in the lacrimal system in the delayed erect film (κ=0.7). Using the dacryocystography data in isolation, no significant association (either direct or inverse) was detected between the lacrimal sac diameter with the nasolacrimal duct diameter (p=0.3).
Discussion
The dacryocystogram is the traditional radiological investigation for epiphora. In 1972 Rossomondo and colleagues6introduced lacrimal scintigraphy, a radionuclide method of imaging the lacrimal drainage system that avoids intubation and allows a more physiological assessment of tear flow dynamics. Since then several reports in the literature have compared the two tests and discussed their role in the diagnosis of epiphora. Chaudhuriet al 11 assessed the diagnostic accuracy of the two techniques and concluded that there was good correlation, although the scintigraphy was marginally superior; this statement was based on the dacryocystogram being unlikely to detect an abnormality in patients with FNLDO. Other authors agree that, when considering all cases of epiphora, the scintigram is a more sensitive investigation and should always be done first.12Hurwitz et al 8 felt, however, that unless scintigraphy is used with quantitative analysis it is of limited value, and acts merely as a complementary test to dacryocystography.
Unlike previous reports, we have concentrated on a subgroup of patients with a clinical diagnosis of FNLDO. This term has been ill defined in the past, but we consider it to mean a patient who has symptomatic epiphora, a lacrimal system patent to syringing, and no detectable cause of epiphora external to the lacrimal drainage system—that is, with no cause for lacrimation and no lid abnormality. The majority of cases in this series had clinically bilateral FNLDO (72%); most abnormalities of the lacrimal system, whether congenital or acquired, tend to affect both sides.4 A recent questionnaire survey demonstrated that the examination of these patients by clinicians with a special interest in this field was extremely variable, and that technetium scans and dacryocystograms were only used by 13% and 10% of the respondents respectively.1
Opinion in the literature suggests that a normal lacrimal scintigram obviates the need for dacryocystography, as there are no instances when the latter would uncover a significant abnormality.12Interestingly, we found in FNLDO that, although both investigations were extremely sensitive (lacrimal scintigraphy 95%, dacryocystography 93%) at detecting abnormalities, there were two systems (4%) normal on scintigraphy but abnormal on dacryocystography, with retained contrast in the delayed radiograph. The high sensitivity for dacryocystography, which is superior at providing anatomical detail of the lacrimal system, results from performing an additional late radiograph in the erect position—specifically to look for failure of the gravitational drainage of contrast from the system, which might reasonably be expected in FNLDO; although the dacryocystogram involves injection of contrast under pressure, the erect film introduces a “physiological” element to the procedure. Confounding factors to this test of “physiological” clearance may arise from dilatation of the system by the high pressure injection of contrast and the different viscosities and surface tensions of water based or oil based contrast media. It is our clinical experience, however, that Lipiodol Ultrafluid disappears almost immediately from the normal nasolacrimal duct on assuming an erect posture.
The main level of blockage in the lacrimal system was easier to detect objectively with lacrimal scintigraphy although, for an experienced observer, reproducible results were demonstrated with dacryocystography. The chief region of lacrimal drainage delay was in agreement for 59% (29/49) of the abnormal systems and, where different, the scintigram usually detected an obstruction at a higher (more proximal) level (35% or 16/49) compared with dacryocystography. It is, therefore, likely that the pressure needed to inject the contrast during dacryocystography tends to dilate lesser degrees of more proximal stenosis in the system. There was no significant relation between specific dacryocystography features, such as upper canalicular reflux or nasolacrimal duct diameter, and the location of isotope retention with scintigraphy; this probably reflecting the very different underlying basis for the tests.
The differentiation of abnormal scintigrams into presac, preductal, or intraductal delay may provide additional information of value in clinical management. Many cases with presac retention may have a primarily canalicular problem, whereas those systems with preductal or intraductal delay have fast transit of tracer into the sac, but an abnormally functioning nasolacrimal duct; these latter patients should have a better prognosis with dacryocystorhinostomy.
Newer radiological imaging techniques, which may advance our understanding and management of FNLDO, include computed tomographic dacrocystography, which uses topical application of a water soluble contrast medium and there are encouraging reports of this method.13 14 These methods are, however, expensive, time consuming, and not widely available. Based on this study, for patients with a clinical diagnosis of FNLDO, we recommend performing oil based contrast macrodacryocystography with a delayed erect film—being reasonably cheap and readily available—and then proceed to lacrimal drainage scintigraphy if contrast radiography is non-contributory.
Acknowledgments
Presented at the 16th meeting of the European Society of Ophthalmic Plastic and Reconstructive Surgery, Budapest, October 1998.