Article Text

Abstract
Aims: To evaluate the clinical significance of macular hole closure types assessed by optical coherence tomography (OCT).
Methods: This study involved 34 eyes of 32 patients who had undergone anatomically successful idiopathic macular hole surgery. The closed macular holes were categorised into two patterns based on OCT; type 1 closure (closed without foveal neurosensory retinal defect) and type 2 closure (closed with foveal neurosensory retinal defect). Association between visual prognosis, type of hole closure, and possible prognostic factors were analysed.
Results: 19 eyes (61.3%) were classified into the type 1 closure and 12 eyes (38.7%) into the type 2 closure. The extent of postoperative visual improvement of type 1 closure group was larger than that of type 2 closure group (p=0.002). The preoperative macular hole size of type 2 closure group was significantly larger than that of type 1 closure group (p=0.006). The duration of symptoms was positively correlated with the preoperative macular hole size (p=0.01). Recurrence of macular hole occurred only in the type 2 closure group.
Conclusion: The type of macular hole closure, which was influenced by the preoperative hole diameter, was associated with postoperative visual prognosis. Early detection and intervention in macular hole should be emphasised.
- macular holes
- optical coherence tomography
Statistics from Altmetric.com
The macular hole is a full thickness defect of the retinal tissue involving the anatomical fovea. Although much progress has been made towards an understanding of macular hole, significant controversy still exists regarding the pathogenesis, management, and prognosis of this lesion. Since the application of vitrectomy combined with gas tamponade to seal macular holes was performed by Kelly and Wendel,1 vitreous surgery has become the standard treatment for macular holes. At present, the anatomical closure rate of macular holes is more than 90% with vitrectomy and adjuvant therapy such as internal limiting membrane peeling or endophotocoagulation.2–4 A number of possible prognostic factors such as the duration of symptoms, preoperative macular hole size, preoperative visual acuity, axial length, age, and sex have been reported.5–7 However, there have been contradictory results regarding the prognosis of macular hole surgery.
Optical coherence tomography (OCT) is a non-invasive diagnostic tool providing high resolution cross sectional images of the macula, and is valuable for several macular disorders including macular hole. The OCT has provided a lot of information regarding the pathogenesis, classification, and diagnosis of macular hole. In addition, the OCT helps to measure the hole diameter and to identify the anatomical status after macular hole surgery.
The closure of macular holes is usually defined as a flattened and reattached hole rim along the whole circumference of macular hole.8 However, the complete disappearance of macular holes after surgery is not an infrequent occurrence. It was reported that postoperative visual prognosis was related to the morphological appearance of a sealed macular hole.9 In this study, we classified the sealed macular hole into two types with OCT; complete sealing of the macular hole without bare retinal pigment epithelium (RPE), and incomplete sealing of the macular hole with bare RPE. The purpose of this study was to find out whether two types of macular hole closure would show different prognoses and to identify which perioperative factors would be associated with different types of macular hole closure.
PATIENTS AND METHODS
This study consisted of a retrospective consecutive series of patients who were operated for idiopathic macular hole in our hospital from January 2001 to April 2002. A total of 36 eyes had undergone operation for idiopathic macular hole during this period. Among them, 34 eyes of 32 patients with closed macular hole after the initial operation were included in this study. The follow up period was 3 months or more for inclusion in the study.
All patients underwent complete preoperative ophthalmological examination including intraocular pressure measurement, lens clarity evaluation, refraction, axial length measurement (Ultrasonic biometer model 820, Humphrey, San Leandro, CA, USA), and biomicroscopic examination of fovea and vitreous. Best corrected visual acuity (BCVA) was measured with the Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity chart. Most of the patients underwent preoperative and postoperative OCT (Humphrey Instrument, San Leandro, CA, USA) examination of the macular lesion, including the measurement of the macular hole diameter. The macular hole diameter was acquired by averaging the vertical and horizontal diameter which was determined at the minimal extent of the hole.
The surgical procedure consisted of standard pars plana vitrectomy, removal of posterior cortical vitreous, indocyanine green dye assisted peeling of the internal limiting membrane around the macular hole, and a total fluid-gas exchange. For Gass stage 2 holes, 25% SF6 gas was injected. For Gass stage 3 or 4 holes, 15% C3F8 gas was injected. If lens opacification was going to significantly impair the visualisation of fundus detail, phacoemulsification and intraocular lens implantation was jointly performed (seven eyes). All of the patients took a facedown position for more than 10 days postoperatively.
Follow up examinations were performed at 2, 4, 8, and 12 weeks after operation, and at an interval of 2 or 3 months thereafter. For the postoperative analysis, we used the BCVA and the OCT scan that were taken 12 weeks after operation. BCVA measurement and OCT scan on the macula were performed by independent observers.
The successful closure of the macular hole was defined as a postoperative biomicroscopic appearance in which the rim of the macular hole disappeared or was attached to the underlying RPE with flattening of the cuff of retinal detachment around the hole.
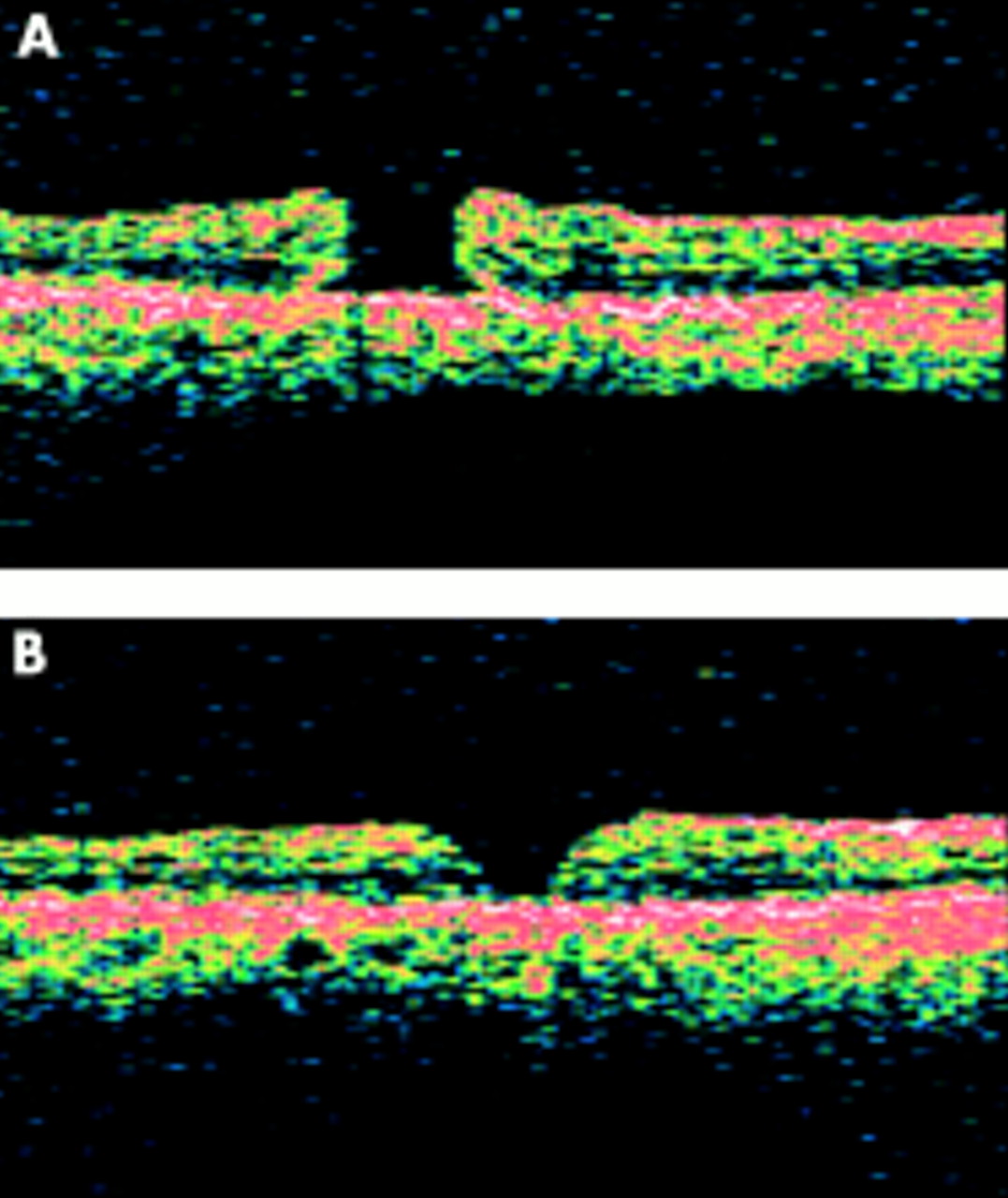
On the basis of postoperative OCT findings we classified the closed macular holes into two groups; type 1 and type 2 closure. Type 1 closure indicates that the macular hole is closed without foveal defect of the neurosensory retina (Fig 1). Type 2 closure indicates that a foveal defect of the neurosensory retina persists postoperatively although the whole rim of the macular hole is attached to the underlying RPE with flattening of the cuff (Fig 2).

Postoperative optical coherence tomography (B) representing type 1 closure, which indicates that there is no interruption in the continuity of foveal tissue above the retinal pigment epithelial layer after the surgery for macular hole. The normal foveal contour is usually encountered in type 1 closure. The symptom duration in this case (patient 28 in Table 1) was 1 month and the hole diameter measured at the preoperative optical coherence tomography (A) was 319 μm.

The postoperative optical coherence tomography (B) representing type 2 closure, which indicates that there is an interruption in the continuity of foveal tissue after macular hole surgery. Thus, the retinal pigment epithelial layer is denuded. The hole edge is thinned and attached to the underlying retinal pigment epithelial layer. The symptom duration in this case (patient 17 in Table 1) was 4 months and the hole diameter measured at the preoperative optical coherence tomography (A) was 727 μm.
In the type 2 closure group, the postoperative macular hole diameters were measured in OCT scans.
Correlations between the amount of postoperative visual improvement and possible perioperative prognostic factors (age, sex, duration of symptom, preoperative BCVA, axial length, refractive error, preoperative macular hole size, type of postoperative macular hole closure) were statistically analysed. Correlations between the postoperative macular hole closure type and the possible preoperative prognostic factors described above were also analysed. Visual acuity measurements were converted to the logMAR scale in analysis.
RESULTS
The clinical characteristics and demographics of the patients are included in Table 1. The patients ranged from 32 to 75 years of age (mean 64.6 years). Five patients were male and 27 patients were female. The duration of symptom ranged from 1 month to 5 years (mean 14.2 months). The follow up period after operation was ranged from 3 to 18 months (mean 9.7 months).
Characteristics of patients with idiopathic macular hole
Among 31 eyes with OCT scan taken 3 months after operation, 19 eyes (61.3%) were classified into the type 1 closure group and 12 eyes (38.7%) were classified into the type 2 closure group.
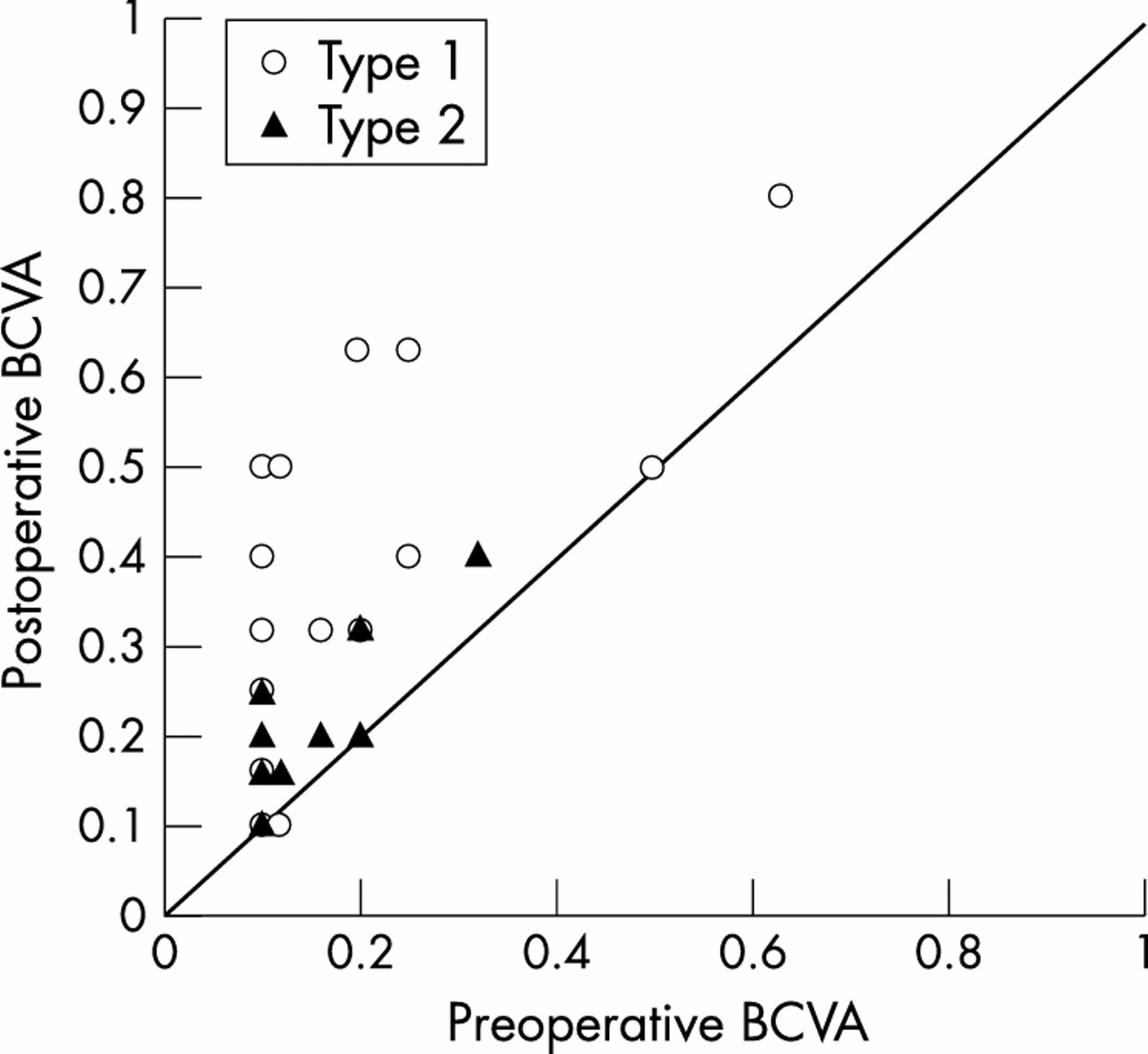
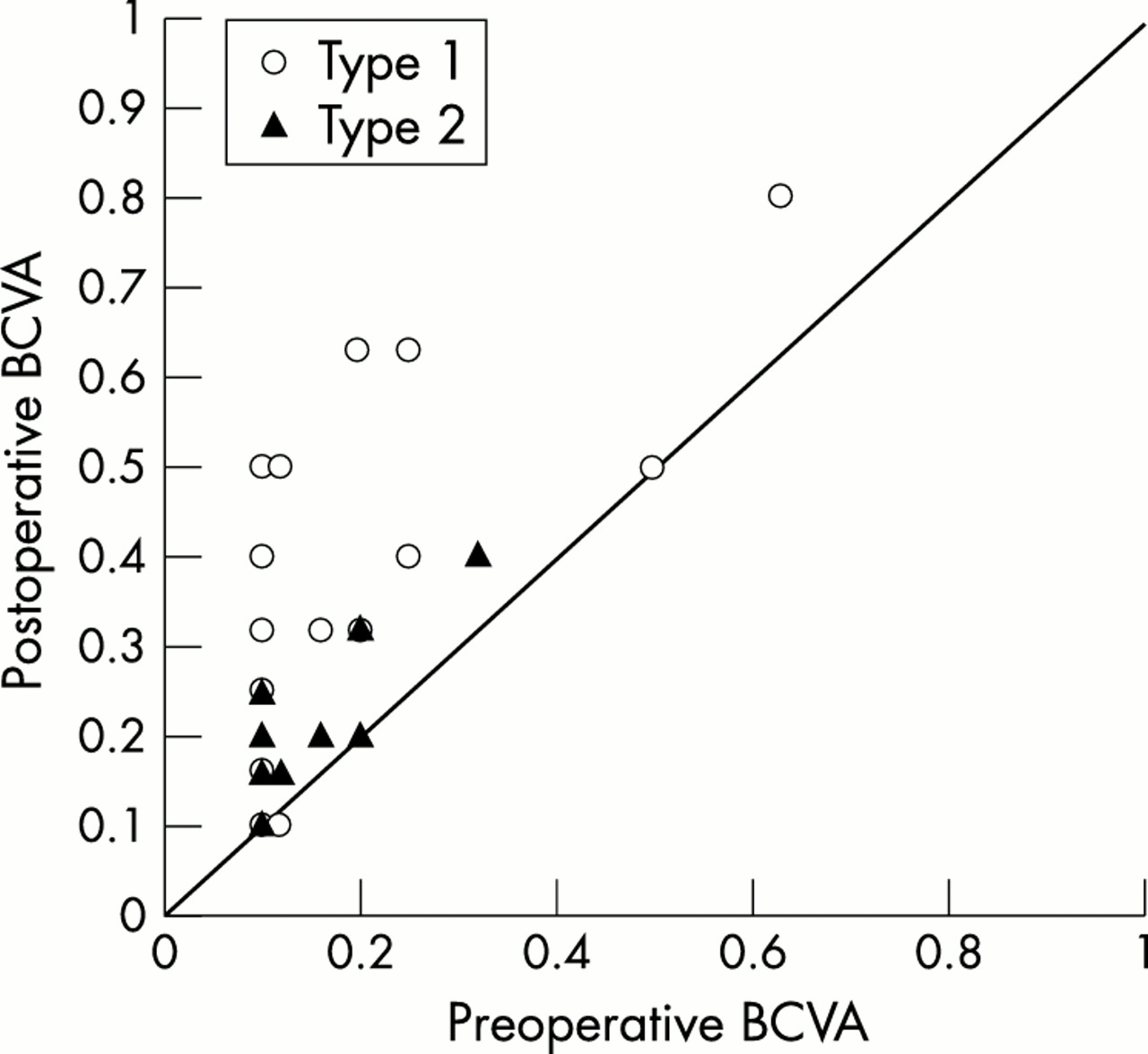
The range of preoperative BCVA measured 3 months after operation was counting fingers to 0.63, with a mean of 0.17. The mean preoperative BCVA was 0.18 in type 1 and 0.15 in type 2. No significant difference of preoperative BCVA existed in each type of closure (p=0.656, Mann-Whitney test). The range of postoperative visual acuity was 0.02 to 0.8, with a mean of 0.33. The mean postoperative BCVA was 0.41 in type 1 and 0.21 in type 2, and this difference was significant (p <0.05) (Fig 3). There was no difference between hole closure types in the incidence of cataract extraction during or after macular hole surgery.
{kind=link}
{kind=link}
{kind=link}
The change of best corrected visual acuity (BCVA) according to the type of macular hole closure.
The mean amount of postoperative visual improvement was 3.03 lines of ETDRS visual acuity chart (p<0.0001). The mean amount of visual improvement was 3.84 lines in the type 1 closure group and 1.62 lines in the type 2 closure group; this difference was also significant (p=0.002, t test). No correlation between preoperative and postoperative vision was noticed.
The range of axial length was 21.20–25.96 mm, with a mean of 23.30 mm. The range of spherical equivalent was −5.5 D to +3.0 D, with a mean of −0.46 D. The preoperative macular hole diameter was measured in 24 cases with OCT. The range of preoperative macular hole diameter was 130–900 μm, with a mean of 551 μm. The axial length, spherical equivalent, preoperative macular hole diameter, age, sex, and duration of symptoms were not significantly correlated with the postoperative visual improvement (Table 2).
Multiple regression analysis of variables with visual improvement
The preoperative macular hole diameter in the type 2 closure group (mean 674 (SD 163) μm) was significantly larger than that in the type 1 closure group (mean 469 (208) μm) (p=0.006). Other possible prognostic factors such as age, sex, axial length, spherical equivalent, duration of symptoms, and preoperative visual acuity were not significantly correlated with the type of closure (Table 3).
Multiple regression analysis of variables with the type of postoperative hole closure (SD)
The postoperative hole diameter was smaller than the preoperative diameter in all cases (nine cases) of the type 2 closure group with both preoperative and postoperative OCT scans, and it was statistically significant (p<0.001, paired t test). The duration of symptoms was positively correlated with the preoperative macular hole size (p=0.01, Spearman’s correlation analysis).
There were no postoperative complications such as endophthalmitis, retinal detachment, or choroidal neovascular membrane formation. Minor complications such as corneal erosion and transient elevation of intraocular pressure were found in some eyes, but these complications were easily controlled by appropriate management.
Cataract extraction after macular hole surgery was performed for two patients (patients 19 and 24 in Table 1) who developed significant lens opacity. In two cases (patients 23 and 30 in Table 1), the macular hole recurred. The macular hole edge was redetached and the subretinal fluid cuff had reformed on the postoperative second and fourth month, respectively. Both cases belonged to the type 2 closure group before the reopening of macular hole. Laser photocoagulation to the bed of the macular hole and total fluid-gas exchange were performed for these cases of recurrence. After these additional procedures, the reopened macular holes were sealed. The reclosed macular holes of both cases also belonged to the type 2 closure group.
DISCUSSION
Although the surgical technique of macular hole has been improved and the hole closure rate after operation has recently been reported to be about 90%, the postoperative visual outcome is not always satisfactory even in eyes with anatomical success.10 Many possible prognostic factors were evaluated in previous reports. Recently, the relation between the vitreoretina and the underlying RPE has been clearly demonstrated through the OCT. The OCT enables us to speculate the preoperative and postoperative macular status. In this study, we found that the type of macular hole closure determined by OCT was significantly correlated with postoperative visual improvement (type 1 > type 2). It was reported that further improvement in visual acuity continued for 2 years after macular hole surgery.11 Considering that only a small number of patients had undergone cataract extraction postoperatively and that the visual acuity was assessed 3 months postoperatively, our cases would have shown better visual results with a longer follow up period. However, we think that the difference in the visual outcome between the two types of hole closure may still persist even after a longer follow up period.
One may raise the question whether the type 2 closure in our study would represent unsuccessfully repaired macular hole. The flattened hole edge, which corresponds to type 2 closure in our study, has been regarded as an anatomical end point after the successful macular hole surgery in previous reports.8,9,12 All cases of type 2 closure in our study showed the reduction of hole diameter as well as the flattening of the hole edge in the postoperative OCT examination. In addition, the improvement of postoperative vision was verified in the type 2 closure group. Hence, we speculate that type 2 closure should be regarded as a kind of successfully repaired macular hole.
Based on ophthalmoscopy or biomicroscopic examinations, the anatomical status of the macula after macular hole surgery was classified by Tornambe et al9 into three types. They suggested that flat and closed outcomes have a better visual prognosis than flat and open outcomes. Imai et al12 categorised the successfully repaired macular hole into three patterns with OCT; U-type (normal foveal contour), V-type (steep foveal contour), and W-type (foveal defect of neurosensory retina). The authors reported that postoperative visual acuity was well correlated with these patterns (U > V > W). Type 1 closure in our study may correspond to a U or V pattern, and type 2 closure to a W pattern. The visual results obtained from the two types in our study were also similar. Because the borderline between the U and V pattern in the aforementioned study was sometimes unclear, and because the ophthalmoscopic appearance of postoperative macular hole status would be easily matched with one of the two types of closure in our study, our classification system seems more clinically relevant.
Our study also proved that the extent of postoperative visual improvement was greater in the case of hole closure without neurosensory retinal defect (type 1 closure) than in closure with neurosensory retinal defect (type 2 closure). The reason for this may be because more residual neurosensory retina indicates a better preserved visual function.5
Several previous reports suggested that the preoperative macular hole size was correlated with anatomical success and visual improvement.5,13–17 Our study results indicate that determination of hole closure type depends strongly on the preoperative macular hole diameter among other possible prognostic factors. In other words, larger macular holes tend to result in type 2 closure postoperatively and smaller macular holes to type 1 closure. Considering that the natural course of stage 2 macular hole will usually develop an enlarged hole and decreased visual acuity18 and that visual benefit was only marginal after operation for stage 3 and 4 macular hole,10 early intervention for full thickness macular hole should be emphasised.
Recently, accurate measurement of macular hole size has been feasible with the development of OCT. Previous reports showed that preoperative analysis and measurement of macular hole size with OCT might help delineate postoperative expectations for successful anatomical closure of the macular hole, visual acuity, and long term closure.15,19 They also reported that late reopening was seen only in macular holes that were 400 μm or larger when measured by OCT.15 In support of the above study, two reopened cases in our study showed a preoperative macular hole diameter of 545 and 668 μm, respectively; these belonged to the type 2 closure group before the recurrence. In this regard, we speculate that type 2 closure is an incomplete form of macular hole sealing, and it lies in between type 1 closure and opened macular hole.
The macular hole sealing process is not clearly delineated. After relief of traction applied to the macular hole, the hole edge approximates as it was demonstrated in all cases of the type 2 closure group in our study; some sort of wound healing process including glial proliferation may commence. The neural tissue defect is relatively small even in apparently larger full thickness macular hole. According to one report, the histopathology of an eye that had undergone macular hole surgery indicated that only a 16 μm defect of the external limiting membrane was detected in a completely sealed macular hole even though the preoperative hole size was much larger.20 In cases with small neurosensory retinal defect, it would be easy to form a glial tissue bridge that connects to the macular hole edge. Previous experience suggests that small retinal holes such as one made by a 41 gauge needle are known to seal up after intraocular tamponade without laser photocoagulation.21 It may represent the sealing process of type 1 closure in our study. Our study results also indicate that the macular hole size is correlated with the preoperative symptom duration. Because the degeneration of the neural tissue at the fovea is obviously advanced owing to the chronicity of disease process in a large macular hole, the absolute diameter of the neural tissue defect in the case of a large macular hole would be accordingly large. The glial bridging or plugging of the relatively large neural defect might be harder, and the macular hole resulted in type 2 closure postoperatively. Because type 1 closure of a macular hole implies a better prognostic sign than type 2 closure, it seems worthwhile to develop a means to promote the complete sealing of the macular hole. This would be the case especially in macular holes with a relatively large diameter.
Although some previous studies reported that shorter axial length was one of the significant variables favouring visual improvement after the surgery,13,14 axial length and spherical equivalent were not correlated with postoperative visual improvement in our study. As both idiopathic and myopic macular hole cases seemed to be included in the previous studies, their cases could not represent idiopathic macular hole. While it is possible to reason the correlation of axial length and visual improvement even in idiopathic macular hole, the demographics and surgical outcomes of idiopathic macular hole differed from those of myopic macular hole.22
The duration of symptom is the possible prognostic factor in idiopathic macular hole surgery. While several reports revealed that the shorter duration of symptoms was correlated with better postoperative visual improvement,2,13,15,16,23 other reports did not.7,17 Our study result showed that the duration of symptoms was not significantly correlated with postoperative visual improvement. However, an important point regarding this issue is that many patients who suffered from macular hole cannot remember exactly the onset of symptoms especially in elderly patients with a healthy contralateral eye.
Preoperative visual acuity was not a determinant factor of macular hole closure type in our study. Although there has been a controversy over the correlation between preoperative and postoperative visual acuity,2,13,17 our study result did not support the correlation. Other parameters such as age or sex were not associated with the postoperative visual improvement and the type of closure in this study.
In summary, the shorter duration of symptoms is associated with the smaller preoperative macular hole size which, in turn, will probably result in the complete sealing of the macular hole without bare RPE after operation. And the complete sealing of the macular hole without bare RPE is associated with better visual acuity, more visual improvement and less recurrence postoperatively. Our results indicate that the smaller the macular hole, the more likely it will benefit from the surgery. Thus, it is thought that early detection and intervention should be encouraged for patients with full thickness idiopathic macular hole. Further studies to promote the complete sealing of macular hole without bare RPE are warranted.