Article Text

Abstract
Aims: To evaluate angiographic features of myopic crescents using fluorescein angiography (FA) and indocyanine green angiography (IA).
Methods: FA and IA angiograms of 88 highly myopic eyes (47 consecutive patients) were reviewed. The follow up period ranged from 5–28 years.
Results: FA revealed two zones of the myopic crescent: a consistently hypofluorescent inner zone and an outer zone with delayed choroidal filling. IA revealed dislocation of the Zinn-Haller ring to the border between the two zones. Myopic crescent enlargement occurred in 68.1%. Only the outer zone increased significantly in most of the eyes with enlarged crescents.
Conclusions: The inner zone might develop as a result of mechanical stretching, and the outer zone might be the result a secondary circulatory disturbance and mechanical stretching.
- myopic eyes
- fluorescein angiography
- indocyanine green angiography
Statistics from Altmetric.com
Peripapillary crescents surrounding the optic disc are a hallmark of eyes with highly myopic refractive error.1 Peripapillary crescents might cause glaucomatous visual field defects in highly myopic eyes; there is a high incidence of glaucomatous visual field defects in highly myopic eyes,2 myopic eyes with peripapillary crescents are more sensitive to intraocular pressure than non-myopic eyes,3 and increasing peripapillary atrophy is associated with progressive glaucoma.4 These findings suggest that large areas of peripapillary atrophy in highly myopic eyes are associated with optic nerve damage and visual impairment. To our knowledge there has been no examination of peripapillary crescents in highly myopic eyes.
We evaluated the angiographic features of myopic crescents using fluorescein fundus angiography (FA) and indocyanine green angiography (IA) in highly myopic patients, and evaluated how these angiographic findings change with the enlargement of peripapillary crescents.
PATIENTS AND METHODS
We retrospectively evaluated medical records and FA and IA angiograms of 47 consecutive patients (88 eyes) with high myopia. Patient age ranged from 12 to 67 years (mean 43.3 years). Refractive error ranged from −8.25 to −28.0 D (mean −15.7 D), and axial length ranged from 25.3 to 33.6 mm (mean 29.8 mm). All patients had peripapillary crescents wider than 0.5 optic disc diameter.
FA was performed using a Pro3 fundus camera (Kowa, Tokyo, Japan) after injecting 5 ml sodium fluorescein. Early phase was considered as up to 2 minutes after injection and late phase as after 7 minutes. IA was performed using a TRC 50IA fundus camera (Topcon, Tokyo, Japan) after rapidly injecting 50 mg indocyanine green dye. Early phase was defined as up to 2 minutes after injection; and late phase as after 20 minutes.
Photographs were scanned using an image scanner (Scanjet CX/T, Hewlett Packard; Palo Alto, CA), and exported to NIH Image software (version 1.62). The area of the peripapillary crescent was defined as the ratio of the total number of pixels of the crescent area divided by the number of pixels of the optic disc area (DA). FA and IA angiograms were overlaid using image analysis software (Photoshop, version 5.0; Adobe; San Jose, CA, USA) and analysed. The crescent enlargement ratio was defined as: (total number of pixels of crescent area at the final examination − total number of pixels of crescent area at the initial examination)/total number of pixels of crescent area at the initial examination. An enlargement ratio greater than 0.1 was considered significant. To ensure reproducibility, the number of pixels was independently measured five times for each eye, and the mean value was used for analysis.
RESULTS
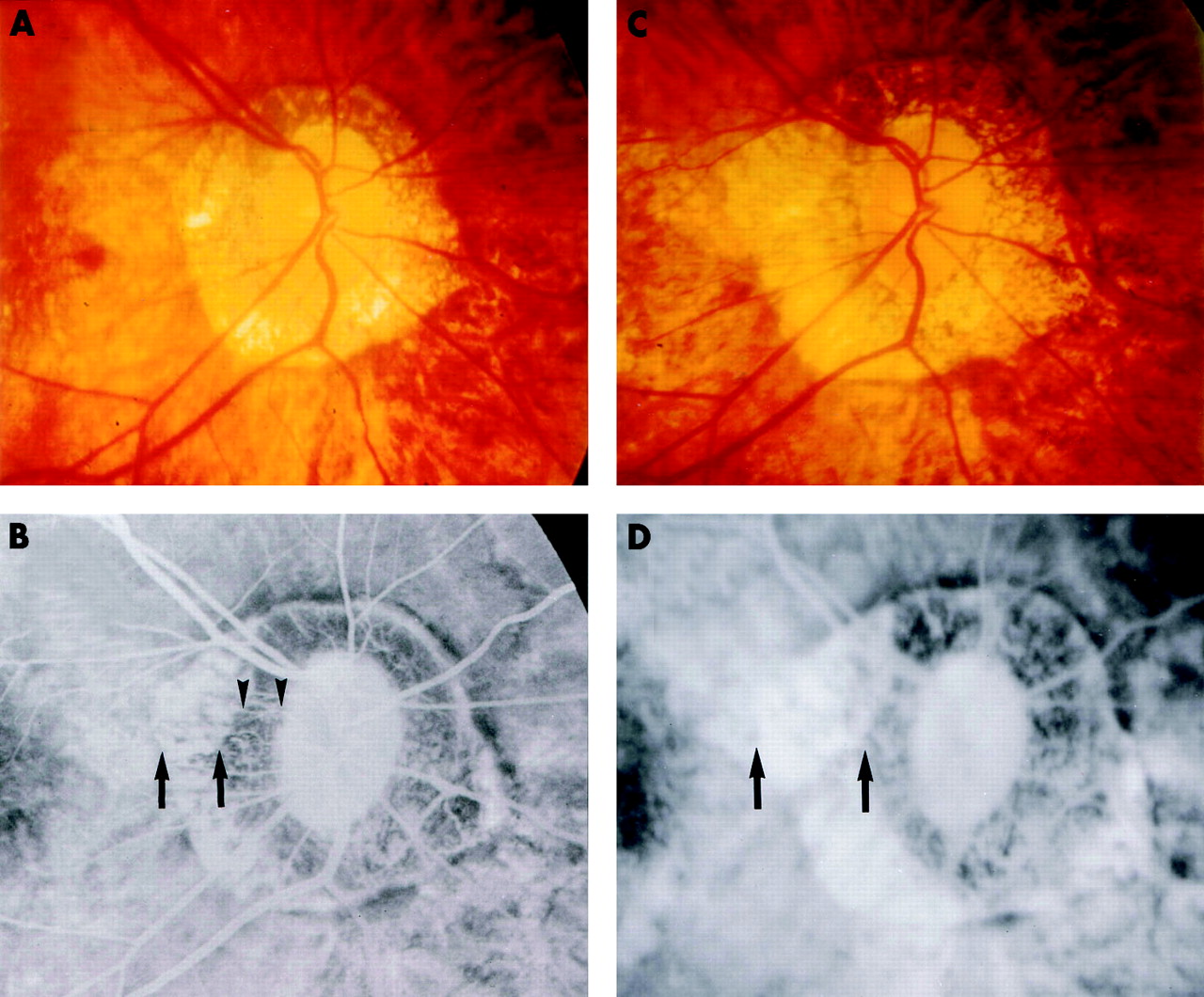
At the initial examination, the area of myopic crescents in 88 eyes ranged from 0.48 to 13.0 DA (mean 3.21 DA). In the FA early phase, there was consistent hypofluorescence across the entire crescent (Fig 1B). In the late phase, the crescent was divided into a hyperfluorescent outer zone and hypofluorescent inner zone in 77 of 88 eyes (87.5%; Fig 1C). IA showed areas of hypofluorescence in the crescent throughout the entire angiographic phase (Fig 1D, E). The Zinn-Haller ring was clearly observed with IA in 64 of 88 eyes (72.7%) (Fig 1D). The overlay technique revealed that the Zinn-Haller ring was located exactly at the border of the outer and inner zones, which were differentiated by FA (Fig 1F).

Angiographic features of myopic crescents in a 32 year old man. (A) Left fundus showed a temporal peripapillary crescent. Refractive error = −13.0 D, axial length = 28.2 mm. (B) The early phase fluorescein angiogram showed hypofluorescence in the entire crescent area. (C) In the late phase fluorescein angiogram, the crescent was divided into a hyperfluorescent outer zone (arrows) and hypofluorescent inner zone (arrowheads). (D) The early phase indocyanine green angiogram showed hypofluorescence in the crescent area. The Zinn-Haller ring was clearly delineated (arrows). (E) The late phase indocyanine green angiogram showed consistent hypofluorescence in the crescent area (arrowheads). (F) Overlaid photograph of (C) and (D) revealed that the Zinn-Haller ring (arrows) was located at the border of the outer and inner zones.
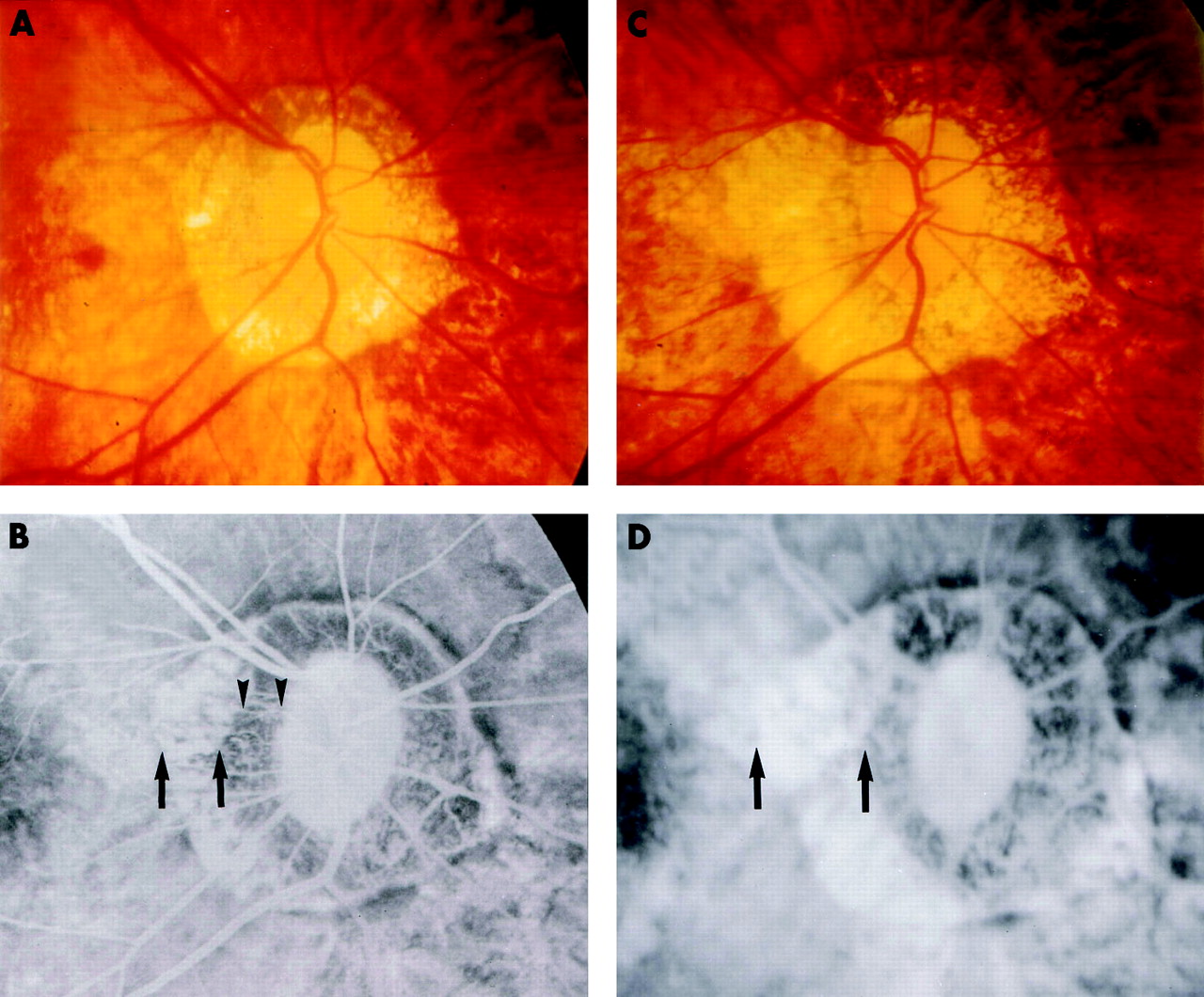
The follow up period ranged from 5 to 28 years (mean 12 years). A significant myopic crescent enlargement (enlargement ratio >0.1) was detected in 60 of 88 eyes (68.1%). The calculated enlargement ratio ranged from 0 to 1.72 (mean 0.38). Crescent enlargement was analysed based on the outer and inner zones. There was a significant enlargement of only the outer zone in 43 of 60 eyes (71.7%; Fig 2B and D), an enlargement of only the inner zone in seven eyes (11.7%), and an enlargement of both in 10 eyes (16.6%).
{kind=link}
{kind=link}
Enlargement of the myopic crescent in a 57 year old woman. (A) Right fundus at the initial examination showed an annular peripapillary crescent. Refractive error = −19.0 D, axial length = 29.4 mm. (B) The late phase fluorescein angiogram at the initial examination clearly showed a hyperfluorescent outer zone (arrows) and hypofluorescent inner zone (arrowheads). (C) Seven years later, the peripapillary crescent had enlarged. (D) The late phase fluorescein angiogram at that time showed that the outer zone of the crescent (arrows) had enlarged significantly.
DISCUSSION
Differential fluorescence between the outer and inner myopic crescent occurred only in the late phase FA angiograms. The outer zone was thought to represent delayed choroidal filling. In contrast, the inner zone was thought to represent the complete loss of choroidal vessels.
Peripapillary atrophy in glaucoma is divided into a central zone beta and a peripheral zone alpha.5 According to Funaki and co-workers,6 zone alpha demonstrates hyperfluorescence due to a window defect, and zone beta remains consistently hypofluorescent by FA. Comparison of these angiographic features indicated that zone beta in glaucomatous eyes and the inner zone in our study had the same FA features. The outer zone of the myopic crescents was hypofluorescent in the early phase and became hyperfluorescent in the late phase in contrast with the consistent hyperfluorescence of zone alpha in glaucomatous eyes.5 One major difference between zone alpha and the outer zone in our study was the size of the area. When the area of delayed choroidal filling is limited, the early hypofluorescence tends to be missed because of rapid dye leakage from the surrounding choriocapillaris. Thus, the FA observations of peripapillary crescents in highly myopic eyes are similar to those in glaucomatous eyes with normal axial length. A previous study also described choroidal circulatory disturbances in eyes with normal pressure glaucoma.7
The recent advancement of IA technology allows for observation of the Zinn-Haller ring in vivo.8 In the present study, the Zinn-Haller ring was dislocated at the border between the outer and inner zones. Dislocation of the ring might be caused by mechanical stretching around the optic disc, suggesting that the inner zone of the myopic crescent also develops as a result of mechanical stretching around the optic disc.
During the follow up, 60 of 88 eyes (68.1%) had significant enlargement of the myopic crescent. Further analysis revealed that in most of these eyes only the outer zone enlarged significantly. The finding that the outer zone might represent a choroidal circulatory disturbance suggests that progression of choroidal circulatory disturbances, as well as mechanical stretching, contribute to crescent enlargement in highly myopic eyes.
Acknowledgments
Supported in part by research grant 14571659 from the Japanese Ministry of Education, Culture, Sports, Science and Technology.