Article Text

Abstract
Aims: To evaluate by impression cytology (IC) the expression of the MHC class II inflammatory marker HLA-DR by the conjunctival epithelium, the cytological modifications of the conjunctival surface according to the Nelson’s classification, and the eventual correlation between the two after severe ocular burns.
Methods: A total of 24 patients (24 eyes) who presented with severe ocular burns underwent IC. We compared them with 18 healthy eyes. HLA-DR expression was studied by flow cytometry as well as the conjunctival histology evaluated with the Nelson’s classification from 2–24 months after the onset of burns.
Results: There was a significant upregulation of the expression of HLA-DR in eyes with burns compared to the healthy population at 2 months (p<0.001), 6 months (p<0.001), 12 months (p = 0.019), 18 months (p = 0.0171) and 24 months (p = 0.01766). A significant difference was found between the Nelson grade in the pathological population and those of the healthy population at 2 months (p = 0.0157). HLA-DR upregulation was significantly correlated with the Nelson’s grades between 2 months (r = 0.69, p<0.0001) and 6 months (r = 0.61, p = 0.0001).
Conclusion: The IC technique can act as a useful tool for following-up ocular surface inflammation after severe ocular burns.
Statistics from Altmetric.com
Severe ocular burns (grade III to VI according to Dua’s classification; table 1)1 have major consequences upon ocular surface inflammation and can be complicated with collateral damage such as cataract and high intraocular pressure. The major complication is the onset of limbal stem cell deficiency secondary to the destruction of the limbus.2 Limbal grafting is the modern treatment approach in the event of subtotal limbal destruction. However, a question remains: when is the best time to perform limbal transplantation? The inflammatory state of the ocular surface plays an important role in achieving satisfactory results, especially when the graft is an autograft or comes from a living related donor).3–9 Persisting stromal and conjunctivo-limbal inflammation has been reported as being a poor prognosis factor of limbal stem cell transplantation4 as is a tear film of bad quality (in part due to the absence of the growth factors usually present in it: epithelial growth factor, tumour growth factor and hepatocyte growth factor).5 The inflammatory microenvironment through inflammatory mediators such as transforming growth factor β1, tumour necrosis factor α and interferon γ alters the inner functioning of limbal stem cells responsible for abnormal cellular proliferation, migration and adherence, and leads to their apoptosis.7 Meller et al reported that in the absence of proper anti-inflammatory treatment during the acute phase in severe ocular burns, the residual limbal stem cell population will decrease progressively leading to localised defects on the ocular surface.8 Puangsricharern et al suggested that stromal and conjunctivo-limbal inflammation also affected transplanted limbal stem survival.9
We conducted a prospective study in the Ophthalmology Department of Jean Bernard University Hospital, Poitiers, France. The first goal was to study the expression on the ocular surface of the MHC class II molecule HLA-DR (a non-specific marker of immune activation indicating exposure to certain pro-inflammatory cytokines expressed by conjunctival cells) with impression cytology in the conjunctiva of patients with severe ocular burns, compared with voluntary healthy subjects. The secondary goal was to analyse cytopathological alterations in the conjunctiva of burned patients compared to healthy subjects according to Nelson’s classification10 (table 2) and to ascertain if there is a correlation with HLA-DR expression.
METHODS
Inclusion criteria
This prospective study adhered to the tenets of the Declaration of Helsinki. Institutional Review Board of the University of Poitiers, Jean Bernard University Hospital, Poitiers, France approval was obtained and an informed consent was signed by every patient included in this study, according to French regulations. We included patients who presented with severe unilateral or bilateral ocular burns (grade III or over according to Dua’s classification1). These patients were compared to a group of 18 normal subjects with no ocular abnormality.
Exclusion criteria
Patients who presented with a grade II or under according to Dua’s classification1 were excluded from the study, as well as contact lens wearers and patients with a history of chronic ocular surface inflammation (Sjögren’s syndrome, chronic allergic conjunctivitis). Patients with grade VI of Dua’s classification or with an insufficient amount of supero-bulbar epithelium on day 1 for proper IC performance were also excluded. For the healthy subjects in the control group, the following were excluded: those with a history ocular trauma, conjunctivitis, dry eye, contact lens wearers, keratitis less than 2 months before the study and those who had been treated with either topical or systemic anti-inflammatory/antibiotic drugs for at least a month before recruitment. Similarly, patients under chronic antiglaucoma treatment were excluded from the study.
Initial treatment
Every patient received an extensive prolonged irrigation with buffered saline solution. They were then hospitalised, receiving a standardised medical treatment during the acute phase consisting of the topical administration of atropine 2% (twice a day), topical ciprofloxacin antibiotic therapy prophylactically (4 times a day), dexamethasone (4 times a day), non-preserved lubricant eyedrops (hourly during the first 12 h and then 6 times a day), doxycyclin (100 mg twice a day), vitamin C (1000 mg/day), and a combination of paracetamol (800 mg) and dextropropoxyphen (60 mg) (3 times a day) was given orally. All patients underwent early amniotic membrane transplantation (between 24 and 48 h after the onset of the burn) according to the technique previously described by Joseph et al11 (the amniotic membrane covering the entire ocular surface, sutured to the limbus and lid margins with 10–0 monofilament nylon with the epithelial surface up and mesenchymal surface in contact with the eye). Dexamethasone and ciprofloxacin eyedrops were tapered off within 2 weeks. Patients stayed on non-preserved lubricant eyedrops (4–6 times a day) up to 24 months. No patient underwent limbal transplantation during the observation period.
Sample collection and handling
Impression Cytology was performed in each patient, according to the technique previously reported by Brignole et al12 2, 6, 12 and 24 months after the onset of the burn. At least 15 min after topical anaesthesia (one drop of 0.04% oxybuprocaine; Novartis Ophthalmics, Bulach, Switzerland), two pieces of filter, 13×6.5 mm in size (polyethersulfone filter, 0.20-μm pores, 13 mm in diameter; Supor, Gelman Sciences, Ann Arbor, Michigan, USA), were applied with forceps to the bulbar conjunctiva (one on the superotemporal and one on the superonasal area) without exerting any pressure for 15–20 s. Specimens were then dipped into tubes with cold, freshly prepared phosphate-buffered saline (PBS) with fixative (0.05% paraformaldehyde). Flow cytometry analysis was performed on the same day on conjunctival cells that were extracted by gentle agitation for 30 min and then centrifuged at 1600 rpm for 5 min.
IC specimens for Nelson’s grading were taken from the superior bulbar conjunctiva by applying with forceps one piece of filter 13×6.5 mm in size (0.22 μm cellulose acetate filter; Millipore, Gelman Sciences, Michigan, USA), taking care not to overlap with the region where the IC intended for the flow cytometry study had been performed. The impression was then transferred by uniform gentle pressure on a glass slide and fixed with 95% ethanol and 1% formalin. The slides were stained with periodic acid Schiff, Wright, haematoxylin-eosin, and Giemsa stains. The same IC procedure was performed once in each voluntary healthy test subject.
Antibodies and flow cytometry processing
Two sets of monoclonal antibodies were used: fluorescein isothiocyanate (FITC)-conjugated mouse IgG1 pan cytokeratin-specific antibody (clone CK3-6H5, Miltenyl Biotec, Bergish Gladbach, Germany) for conjunctival epithelial cells staining and phycoerythrin (PE)-conjugated mouse IgG1 anti HLA-DR (BD Pharmingen, San Diego, California, USA). Five sets of antibodies were used for control: FITC-conjugated mouse anti IgG1, PE-conjugated mouse anti-IgG1, allophycocyanin (APC)-conjugated mouse anti-IgG2, PE-conjugated mouse anti-IgG2a and PE-conjugated rat anti-IgG2a (BD Pharmingen, San Diego, California, USA). Antibodies were used diluted in PBS with 1% bovine serum albumin. After incubation, cells were centrifuged in PBS (1600 rpm, 5 min) and then resuspended in 100 μl of PBS. The specimens were studied on a FACSCalibur™ flow cytometer (Becton Dickinson, Mountainview, California, USA) and data analysed with the Cell Quest™ (BD Pharmingen, San Diego, California, USA) software for Macintosh. For each antibody investigated, a minimum of 2500 conjunctival cells were acquired on a biparametric histogram showing side scatter (cell size) versus forward scatter (cell granulometry). Gates were set around this population to exclude cellular debris. For each of the antibodies tested, results were given in percentages of positive cells.
Statistical analysis
Statistical comparisons for qualitative data were performed with the Pearson χ2 test. Statistical comparisons for quantitative data were performed with the non-parametric Mann-Whitney U test. The correlation between HLA-DR expression and Nelson’s grade was studied by Spearman’s correlation coefficient (r). The level of significance was chosen at 0.05 (Statistica 6.0 for Windows, http://www.statsoft.com/index.htm).
RESULTS
The ocular burns group consisted of 24 patients (22 males, 2 females; 24 eyes). The mean age was 43.71±17.8 years. The control group was made up of 12 patients including 5 females and 7 males (18 eyes). The average age was 32±8.24 years. A total of 11 eyes presented with a grade III burn (45.83%), 11 with a grade IV (45.83%) burn, and 2 with a grade V burn (8.34%). The chemical agents responsible for the burns were alkali for 21 eyes (87.5%) and acids for 3 eyes (12.5%). A total of 6 eyes (25%) presented with clinical limbal stem cell deficiency (LSCD), including 2 total LSCD (8.3%) involving all 12 clock h (CH) and 4 partial (16.6%) (1 with 1 CH, 1 with 4 CH, 1 with 9 CH, and 1 with 10 CH). The mean time for the onset of LSCD was 3.83±2.4 months. All patients (100%) with Dua’s grade V and 36.36% of patients with grade IV developed LSCD compared to no patients with grade III.
HLA-DR expression
The level of expression of HLA-DR on the surface of the conjunctival epithelial cells was significantly higher compared to the healthy population at 2 months (p<0.001), 6 months (p<0.001), 12 months (p = 0.019), 18 months (p = 0.0171) and 24 months (p = 0.01766) after burn (fig 1). There was no statistical correlation between the type of chemical (acidic/alkali) of the burn and the HLA-DR expression rate.

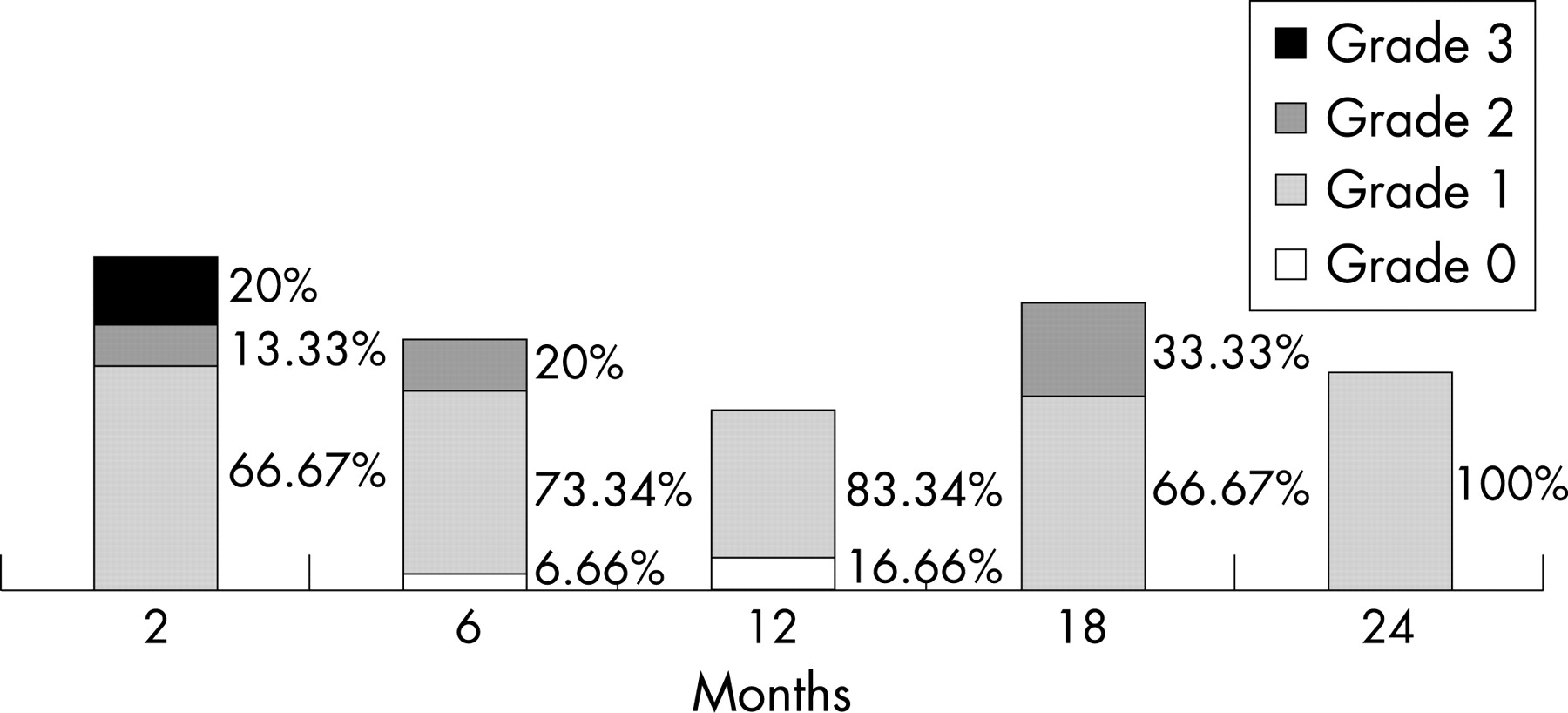
GRADES ACCORDING TO NELSON’S CLASSIFICATION
There was a significant difference between the grade of Nelson in the pathological population and those of the healthy population at 2 months (p = 0.0157). This difference was not significant any more at 6, 12, 18 and 24 months (p>0.05) (fig 2).
HLA-DR/NELSON STATISTICAL CORRELATION
Among burned patients, the level of expression of HLA-DR correlated with the Nelson’s grade to a significant degree 2 months (r = 0.69, p <0.0001) and 6 months (r = 0.61, p = 0.0001). This correlation was no longer significant after 12 months (r = 0.34, p>0.005), 18 months (r = 0.30, p>0.005) and 24 months (r = 0.22, p>0.005) (figs 3, 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The expression of HLA-DR is tightly linked with inflammatory reactions, making it a good marker of the ocular surface inflammation.7 13 14 Recent studies have shown that HLA-DR was overexpressed in various ocular pathologies (dry eye,12 Goujerot-Sjögren,15 chronically treated patient with glaucoma16). Our study compared 24 burned eyes with 18 healthy control eyes. All our patients were evaluated according to the Dua classification, though the majority of the publications still use the classification of Ropper Hall,2 which seems insufficient because it does not consider the conjunctival involvement that plays a major role in the prognosis.1 Some burns classified grade III according to Ropper Hall can correspond to a grade IV or V according to Dua.1 We chose to study patients presenting burns of grade III or above, because we consider that the burns of grade II involve few complications and a different initial management; ambulatory treatment without amniotic membrane transplantation in the acute phase. In our study, the early amniotic membrane transplantation meant that only six patients presented with LSCD. None of the grade III patients developed LSCD, 2 out of the 11 grade IV patients presented with partial LSCD and both grade V patients developed total LSCD (including one complicated by a late onset corneal perforation). These results are similar to the ones previously reported by Meller et al8 The amniotic membrane provides a good substrate for cell migration and attachment: it contains growth factors (epidermal growth factor, hepatocyte growth factor, basic fibroblast growth factor) that helps in corneal reepithelialisation,17 it reduces the conjonctivo-limbal stromal inflammation via the action of antiproteases (α1 antitrypsin, α2 macroglobulin, α2 antichimotrypsin, α2 plasmin inhibitor),18 and it might also inhibit the synthesis of different chemokines by stromal keratocytes.19 As previously reported, these actions help in a rapid reduction of the inflammation and restore the ocular surface of grades II and III of Ropper Hall.8 In our study this was also true for grade III and most of grade IV by Dua. Meller et al8 as well as Joseph et al3 reported corneal epithelialisation failure in patients with grades IV of Ropper Hall, and we similarly experienced total LSCD due to an insufficient remaining limbal stem cell pool in our grade IV patients. In severe ocular burns some level of chronic inflammation remains even after amniotic membrane transplantation. Our study shows that the conjunctival epithelial cells overexpress HLA-DR for up to 12 months after the burn. The peak of this expression happens between 2 and 6 months. HLA-DR then decreases around 12 months. However, there is still a significant overexpression compared with the control group even after 18 and 24 months. Despite normal slit lamp clinical appearances in 86.21% of the patients who did not develop LSCD, there was persisting chronic inflammation long after the acute phase, tending to disappear after 18 months. But it is to be noted that between 2 and 12 months, HLA-DR expression was significantly higher in patients with grade IV and V compared to those with grade III, the very population who did not develop LSCD.
We chose Nelson’s classification10 to evaluate the morphology and the degree of metaplasia of the ocular surface cells. Our results showed a cellular metaplasia with a deficit in goblet cells that varied with time. The degree of metaplasia was significantly different compared to the control group, which was significant at 2 months, with 3 with grade 3, 2 with grade 2 and 8 with grade 1. This difference was no longer significant at 6, 12, 18 and 24 months compared to the healthy population.
The conjunctival surface epithelium, according to Nelson’s classification, was back to normal around 6 months whereas the level of expression of HLA-DR became close to the level of the control group after 12 months. Cytological recovery preceded the return to normal of HLA-DR expression. However, at 12, 18 and 24 months, the majority still showed a slight abnormality (grade 1).
The correlation between the rate of expression of HLA-DR and Nelson’s grade, in dry eye and Goujerot-Sjögren’s Syndrome has been reported.12 Our results showed a correlation between the rate of expression of HLA-DR and Nelson’s grade at 2 and 6 months. This correlation no longer existed at 12, 18 and 24 months. We think that chronic ocular surface inflammation in ocular burns shares some physiopathological mechanisms with dry eye because the deficit in goblet cells after the burn induces a disturbance of the mucin layer of the tear film resulting in a xerophthalmia.20 Postchemical injury inflammation could therefore be perpetuated by dry eye induced inflammation.20–22
LSCD treatment in chemical injury by limbal autograft or allograft (from cadaver or living related donor eyes) have reported good success.23 24
However, chronic inflammation is known as a bad prognosis factor for limbal grafting. Therefore, it is useful to know when inflammation is the lowest in order to perform the limbal graft while maximising the chances of success.4–25 This issue is of great importance when doing an autograft or an allograft from a living related donor.25 Thus, this study shows that evaluating HLA-DR expression by IC is a good method to monitor inflammation and determine when is the best time for limbal stem cell transplantation.
Clinicians have recommended that 12–18 months be allowed to lapse before limbal stem cell transplantation following acute burns.25 This is to avoid transplanted tissue being destroyed by the inflammatory process. This study provides a scientific basis for that clinical practice.
REFERENCES
Footnotes
Competing interests: None.
This prospective study adhered to the tenets of the Declaration of Helsinki. Approval was obtained from the Institutional Review Board of the University of Poitiers, Jean Bernard University Hospital, Poitiers, France and an informed consent was signed by every patient included in this study, according to French regulations. None of the authors have any commercial interest in the products that are mentioned in this manuscript.
- Abbreviations:
- FITC
fluorescein isothiocyanate
- IC
impression cytology
- LSCD
limbal stem cell deficiency
- PAS
periodic acid Schiff