Article Text

Abstract
Purpose To present the long-term results of Ahmed glaucoma valve (AGV) implantation.
Methods Consecutive case series of 94 eyes with AGV implantation over 7 years. Temporary tube ligation with C3F8 gas fill was used in high-risk eyes (group G&L) and compared with standard implantation in both phakic (group A) and pseudophakic/aphakic eyes (group B). Success was intraocular pressure (IOP) of 6 mm Hg or greater and 21 mm Hg or less and/or IOP reduction of 20% or greater.
Results Average follow-up was 28.9±20.3 months. The mean preoperative IOP changed from 30.8±8.2 to 19.7±7.6 mm Hg and mean preoperative medications changed from 3.3±1.2 to 1.2±1.1 at the final visit. Cumulative probability of survival at 1 and 4 years was 89.1% and 72.9%. There was no statistically significant difference in success between the three groups, but complications due to postoperative hypotony (six eyes) only occurred in group B. Other complications were corneal decompensation (three eyes), tube erosion (six eyes) and aqueous misdirection (four eyes).
Conclusions AGV implantation offered good long-term IOP control with a success rate of 78.7%. The authors recommend C3F8 gas fill and temporary tube ligation in eyes at high risk of postoperative hypotony and the use of donor sclera or human pericardial patch to prevent tube erosion.
- Ahmed glaucoma valve
- aqueous humour
- aqueous shunts
- C3F8
- intraocular pressure
- postoperative hypotony
- suture ligation
- treatment surgery
Statistics from Altmetric.com
- Ahmed glaucoma valve
- aqueous humour
- aqueous shunts
- C3F8
- intraocular pressure
- postoperative hypotony
- suture ligation
- treatment surgery
Glaucoma tube implants (aqueous shunts) are used for the surgical treatment of uncontrolled intraocular pressure (IOP) in eyes with refractory glaucoma, and reported success rates are between 60 and 82% at 2 years,1–5 with a reported 10% per year failure rate.6 The most serious immediate complications of aqueous shunts are those related to postoperative hypotony, including shallow and flat anterior chambers, choroidal detachments and suprachoroidal haemorrhage (SCH).7–9 Erosion of the tube through the conjunctiva is a potential hazard of aqueous shunts and may lead to endophthalmitis.10 Corneal endothelial failure (CEF) has been described as the principal long-term complication.6
To avoid postoperative hypotony non-valved shunts are now implanted with a temporary ligature of the tube. The Ahmed glaucoma valve (AGV; Rancho Cucamonga, California, USA) has a silicone elastomer membrane held in a polypropylene or silicone body forming a non-obstructive valve that should prevent excessive aqueous drainage and anterior chamber collapse. However, postoperative hypotony has been reported in up to 29% of cases1 4 5 11–13 of AGV implantation, causing flat anterior chambers in up to 10% of eyes and SCH in up to 5% of eyes.1 2 11 13–15
We report an audit of consecutive cases of AGV implanted from 2002 to 2008 by one surgical team, highlighting our attempts to reduce the incidence of serious complications such as postoperative hypotony and tube erosion. Sudden hypotony following surgical decompression is reported to be the precipitating factor responsible for the occurrence of SCH with aphakia, pseudophakia and previous vitrectomy identified as the major risk factors for SCH.16–18 From September 2004, we attempted to avoid hypotony in eyes with these risk factors by using anterior chamber C3F8 gas fill coupled with polyglactin (Vicryl, Ethicon) suture ligation as described by Franks and Hitchings19 for use in non-valved implants. To prevent conjuctival tube erosion we used a scleral patch graft,20 a scleral rotation flap21 or a pericardial patch graft.22 As this gas and ligature (G&L) technique might carry the risk of inducing a postoperative IOP spike or prolonging the ‘hypertensive phase’ commonly seen with AGV implantation,2 11 14 we compared the postoperative pressure profiles of our G&L eyes with those of glaucomatous eyes undergoing standard AGV implantation in our unit during the same time period.
Patients and methods
Patient selection
The indication for AGV implantation was the presence of glaucoma with medically uncontrolled IOP and the presence of factors that would make filtering surgery unlikely to be successful, such as uveitis, previous failed filtering surgery or aphakia. All eyes undergoing AGV implantation from January 2002 to July 2008 were included in this consecutive case series. The majority of the implants were the S-2 single plate model. From January 2008 onwards we implanted only the FP-7 model (single plate silicone body). Surgery was performed by one of the authors (PKW) in all but six eyes, in which surgery was under the supervision of PKW.
Data collection
For each patient we documented the age, gender, race, glaucoma diagnosis, total number of operations before the AGV insertion, presenting IOP, preoperative IOP and visual acuity, gonioscopy and corneal thickness measured by ultrasonic pachymetry (‘Pachmate’; DGH Technologies, Exton, Pennsylvania, USA). Full ophthalmic examination with visual acuity, Goldmann applanation tonometry and fundus examination were performed at all visits. The mean number of medications was calculated by the addition of each medication as one unit, with fixed combinations scored as two and systemic acetazolamide—Diamox SR (Goldshield Pharmaceuticals, Croydon, UK), dose 250 mg twice a day—also scored as two units. Postoperatively the IOP and visual acuity were noted at day 1, day 7, month 1, month 2 and thereafter at 3–6-monthly intervals.
Technique
Following a case of SCH after AGV implantation in an aphakic eye in September 2004, we modified our technique of AGV implantation such that all high-risk eyes undergoing AGV implantation had 14% perfluoropropane (C3F8) gas injection into the anterior chamber by means of a paracentesis and ligation of the tube with a 5 ‘O’ Vicryl suture. Such cases are reported as our G&L group. Eyes having standard implantation without gas or ligature are reported as standard group A (phakic eyes) and standard group B (aphakic/pseudophakic eyes). On implanting an AGV it is necessary first to prime the valve with balance salt solution (Alcon, Fort Worth, Texas, USA), which creates a small drainage hole at the posterior edge of the elastomer membrane. To prevent injected C3F8 gas escaping up the tube and through this hole, temporary occlusion of the tube was provided by a 5 ‘O’ Vicryl ligature. The ligature was tied with three throws of the suture to achieve a compression rather than occlusion of the tube and pulled tight enough to prevent the escape of gas from the anterior chambers up the tube. The high surface tension of a C3 F8 gas bubble should prevent anterior chamber collapse in the event of excess aqueous leak round the tube or the sudden development of choroidal detachments. Tube implantation in all cases was by means of a ‘23’-gauge needle track 2 mm posterior to the limbus through full thickness scleral tissue into the anterior chamber to achieve a water-tight fit. To cover the tube, we used either an autologous scleral rotation flap (figure 1),21 or a donor scleral or pericardial patch.20 We initially used bovine pericardium: Tutopatch (Tutogen GMBh, Neunkirchen am Brand, Germany), but after observing overlying conjunctival melt in some cases we changed to human donor pericardium: Tutoplast (Tutogen GMBh). The conjunctiva was closed with interrupted 8 ‘O’ or 10 ‘O’ Vicryl sutures. No antimetabolites were used in this study. Postoperative topical steroids, Pred Forte (Allergan, Irvine, California, USA) were given four times a day for 1–2 months and atropine drops twice a day for 2 weeks.
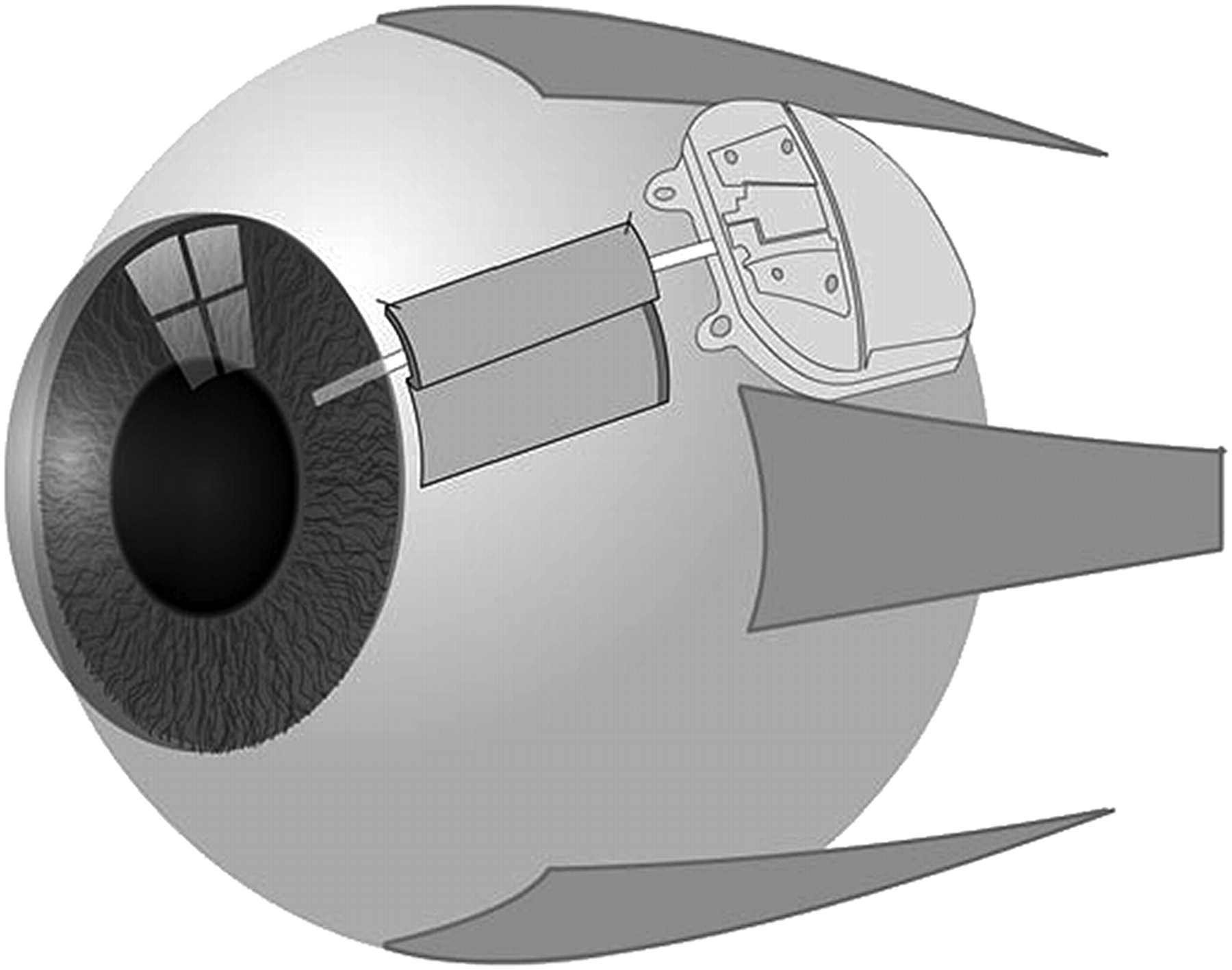
Silicone tube of Ahmed glaucoma valve is covered by a scleral rotation flap.
Outcome measures
Success was defined as in the Tube Versus Trabeculectomy Study7 23: IOP 6 mm Hg or greater and 21 mm Hg or less with or without medication and/or IOP reduction of 20% or greater relative to preoperative values. Failure was defined as IOP greater than 21 mm Hg or not reduced by 20% below baseline on two consecutive follow-up visits after 3 months, IOP of 5 mm Hg or less on two consecutive follow-up visits after 3 months, re-operation for glaucoma, or loss of light perception vision. Eyes that had not failed and were not on supplemental medical therapy were considered complete successes. Eyes that had not failed but required supplemental medical therapy were defined as qualified successes.
Statistical analysis
Statistical analysis was performed using the SPSS 16 software for Windows. Descriptive statistics were employed to summarise demographics and outcome characteristics of the groups. Student's t test was used to determine the significance of any differences in the continuous variables within each group. The Wilcoxon signed rank test was used to compare the pre and postoperative antiglaucoma medication scores. The one-way analysis of variance was used to compare means of the three groups and post hoc tests were used for comparisons between groups. A p value of less than 0.05 was taken as statistically significant. The cumulative probability of success was derived using the Kaplan–Meier survival curve and the log-rank test was used to compare survival between groups. The time to failure was defined as the time from AGV implantation to re-operation for glaucoma or the first of the two consecutive visits after 3 months when the patient had hypotony or uncontrolled IOP.
Results
Ninety-four eyes of 83 patients underwent AGV implantation with a mean follow-up of 28.9±20.3 months (range 2–84). These included 51 high-risk eyes that underwent AGV with gas fill and ligature (G&L group; 50 aphakic/pseudophakic and one myopic phakic) and 43 eyes that underwent standard AGV implantation, comprising 28 phakic (standard group A) and 15 pseudophakic/aphakic (standard group B) eyes. Patient demographics and preoperative characteristics are detailed in table 1.
Patient demographics and characteristics of study population
The G&L group and standard group B had a significantly higher mean age (66.5 and 65.6 years vs 50.5 years) and number of previous operations (2.4 and 2.1 vs 0.9) compared with the standard group A (p=0.001 and 0.000, table 2, figure 2). There was no significant difference between the groups in respect of the presenting IOP, preoperative IOP and number of medications (p>0.05).
Results
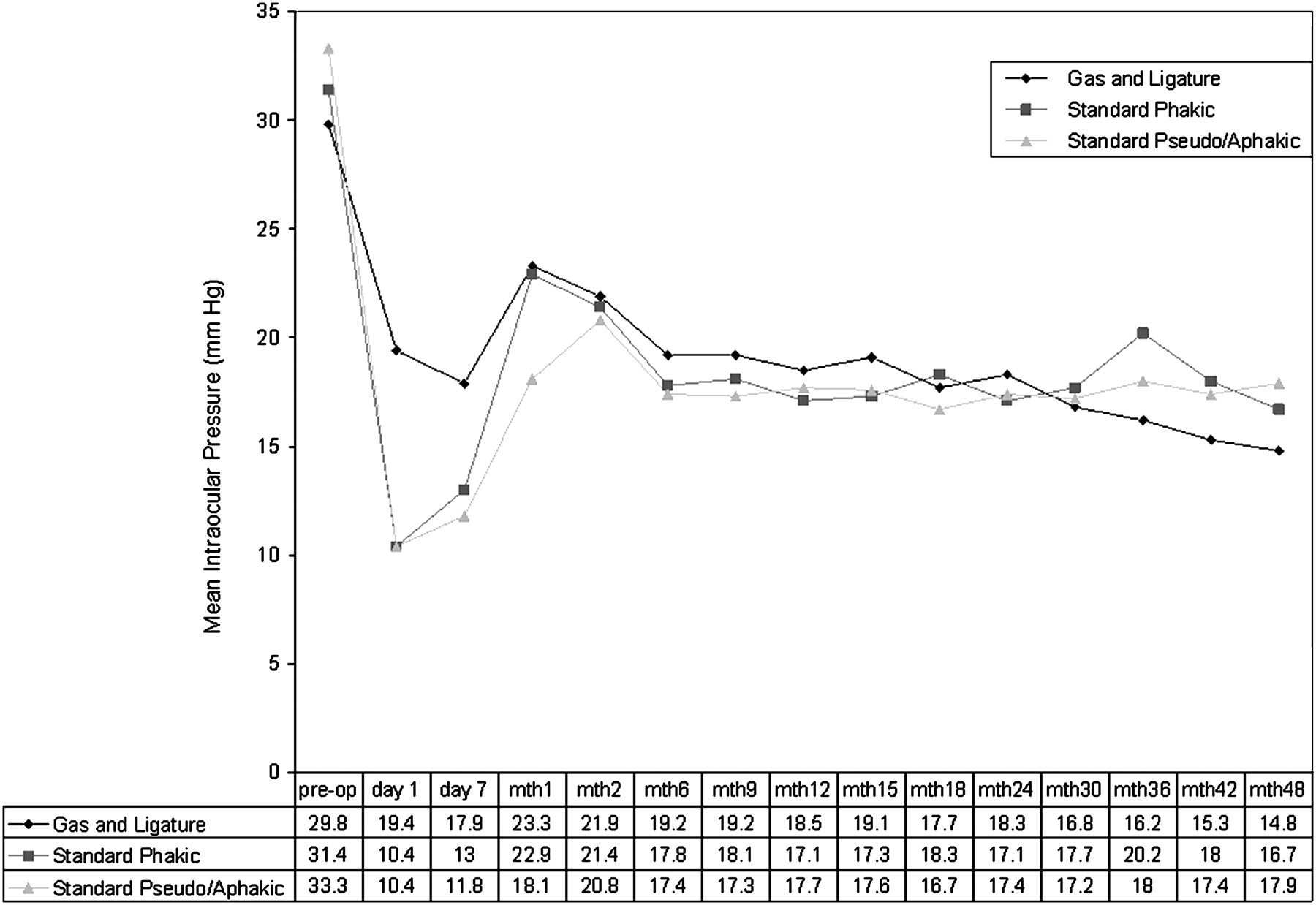
Change in intraocular pressure (IOP) with time. Mean preoperative IOP changed from 29.8±7.6 to 20±7.5 mm Hg (gas and ligature group), 31.4±9.8 to 18.9±6.2 mm Hg (standard phakic group) and 33.3±6.5 to 20.5±10.2 mm Hg (standard pseudophakic/aphakic group) at final visit, a mean change of 30.8, 34.5 and 36.2%. The change in IOP was statistically significant at all times postoperatively (p<0.05).
The mean preoperative and postoperative IOP, antiglaucoma medication, outcome and complications are detailed in table 2. Postoperative IOP control with time is shown in figure 2. The change in IOP was statistically significant at all times postoperatively in all groups. The mean IOP at day 1 and day 7 was significantly higher in the G&L group compared with the standard A and B groups (p=0.000 and 0.006). There was no significant difference in IOP at days 1 and 7 between standard groups A and B. On the first postoperative day, eight eyes in the G&L group had IOP greater than 30 mm Hg (mean 38 mm Hg, range 32–45 mm Hg), which was relieved by tapping the gas bubble by needle pressure on the site of the paracentesis. There was no significant difference in the final IOP between the groups (p=0.56). The mean number of medications reduced significantly in all groups (table 2, p<0.001) and there was no significant difference in the postoperative medication scores of the three groups (p=0.4). At final follow-up success was achieved in 75% eyes in the G&L group, 82.1% in standard group A and 73.4% in standard group B. Complete success was achieved in 30.8% eyes in the G&L group, 39.2% in standard group A and 13.3% in standard group B. Kaplan–Meier survival analysis is detailed in figure 3. The cumulative probability of maintaining an IOP of 6 mmHg or greater and 21 mmHg or less and/or a 20% or greater drop in IOP for the G&L group, standard group A and standard group B was 87.9%, 92.4% and 86.7% at 1 year and 62.9%, 71.5% and 86.7% at 4 years, with a mean survival time of 38.7 months, 66.6 months and 62.7 months. There was no statistically significant difference in the survival between groups (p=0.19).

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival curve for the groups. Kaplan–Meier survival analysis showed a cumulative probability of maintaining an intraocular pressure (IOP) of 6 mm Hg or greater and 21 mm Hg or less and/or an IOP drop of 20% or greater for the gas and ligature group (G&L), standard phakic group and standard aphakic/pseudophakic group to be 87.9%, 92.4% and 86.7% at 1 year and 62.9%, 71.5% and 86.7% at 4 years, with a mean survival time of 38.7 months, 66.6 months 62.7 months, respectively. There was no statistically significant difference in the survival between groups (p=0.19).
Complications are summarised in table 2. CEF directly attributable to AGV implantation occurred in only one eye. This eye was in the G&L group and followed the development of aqueous misdirection with a flat anterior chamber after AGV implantation. CEF worsened after AGV implantation in two eyes with previous intraocular surgery. Late CEF was seen in three other eyes with pre-existing corneal damage—two traumatic aphakic eyes, one iridocorneal endothelial syndrome eye. There was one case of SCH occurring in a 73-year-old aphakic eye with previous vitrectomy that underwent standard AGV implantation. Visual acuity was reduced to perception of light but after drainage of the haemorrhage and vitrectomy with injection of heavy oil, the vision recovered to 6/9. Aqueous misdirection occurred in four pseudophakic eyes after AGV implantation. Zonulo-hyaloido-vitrectomy24 was effective in correcting the aqueous misdirection in all cases. Three of the four cases occurred in eyes with previous acute angle closure glaucoma. Three eyes with advanced visual field loss had a reduction of vision to levels of hand movements by final follow-up.
Discussion
The purpose of this report is to share our experience of the success and hazards attendant on AGV implantation and to describe our attempts to improve the safety of AGV implantation. Sudden postoperative hypotony following tube implantation can lead to serious complications: shallow/flat anterior chambers, the development of choroidal effusions or SCH. SCH is associated with sudden lowering of IOP with aphakic, pseudophakic and vitrectomised glaucomatous eyes especially at risk of this complication following tube implant surgery,16–18 and SCH can follow even relatively minor surgical procedures in glaucomatous eyes.25 26 Shallow or flat anterior chambers in pseuodophakic eyes are a serious complication as this may permit the tube or the intraocular lens implant to touch the corneal endothelium leading to late CEF.
Complications of hypotony do still occur despite tube ligation of non-valved aqueous shunts, with reports of choroidal effusion in 16%, shallow or flat anterior chambers in 11% and SCH in 2%.7 9 23 Following AGV implantation, despite the presence of a valve, a similar rate of these complications still occurs.2 9 14 15 Kee13 described the use of a ligature technique with AGV reducing postoperative hypotony from 25% to 6%, but we could not find any reports of the use of C3F8 with the AGV.
The technique of 14% C3F8 gas fill and ligature in our study was effective in preventing early hypotony and shallow/flat anterior chambers in our G&L group. All our serious complications related to a sudden reduction of IOP postoperatively were seen in the ahakic/pseudophakic eyes with standard implantation in group B. Although eight eyes developed IOP greater than 30 mm Hg on day 1, this IOP was on no glaucoma medication. The mean IOP in the G&L group on the first postoperative day was 19.4 mm Hg, which is similar to that reported for non-valved Glaucoma Drainage Devices (GDD)7 9 23 or following cataract surgery27 or following cyclodiode laser ablation.28 29
Four cases of aqueous misdirection occurred in the G&L group in pseudophakic eyes, three of which had had previous acute angle closure glaucoma. In the fourth eye the aqueous misdirection occurred peroperatively before C3F8 injection as it was noted that there was sudden shallowing of the anterior chamber and the anterior chamber could not be deepened with a C3F8 gas fill, the anterior chamber only retaining a very small amount of gas. Therefore, we do not feel gas contributed to the development of aqueous misdirection, which has been observed in up to 3% of other studies of tube implants.2 7 11 14 15 All cases responded to zonulo-hyaloidectomy with anterior vitrectomy through a peripheral iridectomy as described by Lois et al.24
We had a low incidence of new corneal failure (one eye) developing postoperatively in our series and we suspect this may be related to our low incidence of shallow/flat anterior chambers and hypotony, which reduced the risk of tube/corneal touch. The five other eyes with CEF all had significant preoperative corneal disease.
The AGV ‘hypertensive phase’ is an elevation in IOP occurring within the first 3 months postoperatively, reported to occur in between 48.5% and 82% of eyes undergoing AGV implantation,2 11 14 15 and to resolve in approximately 30% of cases.14 On days 1 and 7 the mean IOP was higher in the G&L group than in the standard groups A and B (figure 2). After day 7 the IOP in the three groups was very similar during follow-up. In all groups the IOP peaked at 1 month postoperatively, presumably indicating the peak of the AGV hypertensive phase. This finding would seem to indicate that the only effect on AGV function of gas and ligature was to elevate the mean IOP temporarily in the first postoperative week. There was no statistically significant difference between the surgical success rates of AGV implantation between our G&L and standard groups A and B.
Other studies of AGV implantation report success rates at 12 months of 70.5% to 83%, achieving mean IOP of 16.4 mm Hg to 18.3 mm Hg on a mean of 1.3 medications, which are similar to our success rates but with a higher rate of postoperative hypotony than ours.9 11 13 14
Preventing conjunctival tube erosion
Without a patch graft or scleral flap to cover the tube, there can be a high rate of tube erosion10 predisposing the eye to the development of infectious endophthalmitis.30 31 A rate of tube exposure of up to 7% following donor scleral patch grafts has been reported,11 15 32 and although donor sclera for a patch graft was successful in preventing erosion in our cases, we used the scleral rotation flap21 method of covering the tube as this avoids the potential transmission of infection from donor tissue.33 However, we noted three erosions out of our 28 scleral rotation flap cases and therefore abandoned this technique latterly and used dried stored pericardium as a patch cover. Tube erosion has previously been reported in up to 2.6% of cases in which human pericardium was used,22 34 35 and so we initially used bovine pericardium (Tutopatch) to prevent erosion as it is twice as thick. However, with Tutopatch, a severe inflammation of the conjunctiva overlying the tube developed in the first postoperative month in 30% of cases. We therefore abandoned Tutopatch and have since used human pericardium (Tutoplast) as the tube cover with no inflammation or erosions to date.
Conclusions
In complex eyes unlikely to respond to conventional filtering procedures, AGV provides a good long-term rate of success with a low rate of complications. We had no cases of endophthalmitis and no cases of persistent hypotony over our 7-year study.
C3F8 gas and temporary Vicryl ligature is a useful technique for the prevention of postoperative hypotony when implanting AGV in high-risk eyes, for example, previous vitrectomy, aphakia or high myopia.
Donor sclera and human pericardium (Tutoplast) appear to be as effective as patch grafts to prevent conjunctival tube erosion.
CEF was an unusual complication of AGV in our study, and we feel that the avoidance of hypotony may be an important factor by preventing shallow or flat anterior chambers and subsequent tube or lens/corneal endothelial touch.
References
Footnotes
Synopsis: Ahmed glaucoma valve implantation is a relatively safe and effective procedure for the management of uncontrolled glaucoma. Steps designed to reduce the incidence of serious postoperative complications (including hypotony and tube erosion) are described.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.