Article Text

Abstract
Aims To determine the level of vascular endothelial growth factor (VEGF) and pigment epithelium-derived factor (PEDF) in the plasma of patients with proliferative diabetic retinopathy before and after an intravitreal injection of bevacizumab.
Methods Eleven patients with type 2 diabetes and control of 30 non-diabetic patients were studied. The 11 eyes of 11 patients received an injection of bevacizumab (1.25 mg). Samples of blood were collected just before the injection, and after 1 day, 7 days and 1 month. The concentrations of VEGF and PEDF in the plasma were measured by ELISA.
Results The VEGF concentration before the injection was 114.0 pg/ml. It was significantly reduced to 9.7 pg/ml after 1 day, to 11.7 pg/ml after 7 days and to 25.9 pg/ml even after 1 month (p<0.001, p<0.001, p<0.001, respectively). The PEDF concentration before the injection was 7.2 μg/ml. It was significantly reduced to 5.8 μg/ml after 1 day, to 5.8 μg/ml after 7 days and to 6.3 μg/ml after 1 month (p<0.001, p<0.001, p>0.05, respectively).
Conclusions The decreased levels of blood VEGF after an intravitreal injection of bevacizumab indicate that bevacizumab enters the general circulation and may also affect the PEDF levels. Thus, we should carefully examine patients for systemic changes and the fellow eye after an intravitreal injection of bevacizumab.
- Bevacizumab (Avastin)
- diabetic retinopathy
- vascular endothelial growth factor (VEGF)
- pigment epithelium-derived factor (PEDF)
- angiogenesis
- neovascularisation
- experimental and laboratory
Statistics from Altmetric.com
- Bevacizumab (Avastin)
- diabetic retinopathy
- vascular endothelial growth factor (VEGF)
- pigment epithelium-derived factor (PEDF)
- angiogenesis
- neovascularisation
- experimental and laboratory
Vascular endothelial growth factor (VEGF) has been implicated in the development of human eye diseases characterised by neovascularisations, and the level of VEGF in the vitreous is highly correlated with the growth of new blood vessels in eyes with diabetic retinopathy.1 2 Pigment epithelium-derived factor (PEDF), on the other hand, is known to be the most potent natural inhibitor of ocular angiogenesis.3 4
A blockage of VEGF has been associated with an inhibition of iris neovascularisation and suppression of the formation of new retinal vessels in primates.5 These findings provided the rationale for anti-VEGF therapy in retinal vascular diseases associated with angiogenesis.
Bevacizumab (Avastin, Genentech, Inc., San Francisco, California, USA) is a recombinant human monoclonal IgG1 antibody that inhibits human VEGF. It has been approved by the US Food and Drug Administration for intravenous use for metastatic colorectal cancer. Several case series have been recently published on the off-label use of intravitreal bevacizumab in VEGF-mediated diseases.6–8
With the expanding application of bevacizumab worldwide, it seems prudent to determine the VEGF levels in different tissues after intravitreal injections of bevacizumab to optimise the dosing regimens. Intravitreal bevacizumab has been shown to be associated with a substantial decrease in the aqueous VEGF levels in patients with diabetic retinopathy.9 10 Chan et al11 also reported on the aqueous VEGF and PEDF levels after intravitreal bevacizumab injection in patients with choroidal neovascularisation. However, to the best of our knowledge, data have not been published on the blood levels of VEGF after an intravitreal bevacizumab injection in a human case series.
Thus, the purpose of this study was to determine the blood levels of VEGF after a single intravitreal injection of bevacizumab and also to determine the levels of PEDF in patients with diabetic retinopathy.
Materials and methods
Subjects
The procedures used in this study conformed to tenets of the Declaration of Helsinki and were performed after receiving approval from the institutional review committee of the Kansai Medical University. An informed consent was obtained from all patients. Patients with proliferative diabetic retinopathy were included if they had neovascular glaucoma, rubeosis of the iris and/or angle structures including the trabecular meshwork, and had aggressive proliferative diabetic retinopathy. Eyes that had undergone vitrectomy were excluded.
Eleven patients with type 2 diabetes mellitus (nine men and two women) and control of 30 non-diabetic patients (15 men and 15 women) were studied. All 11 eyes of the 11 patients received an intravitreal injection of bevacizumab (1.25 mg). The clinical characteristics of the patients are shown in table 1. Eight eyes underwent vitrectomy 1 day after the injection of bevacizumab and three eyes received panretinal photocoagulation after the injection of bevacizumab.
Data of patients with diabetes mellitus
Injection technique
The intravitreal injection of bevacizumab was performed as described.9–11 Briefly, under sterile conditions in the operating room, 1.25 mg (0.05 ml) of bevacizumab (Avastin 100 mg/4 ml) was injected into the vitreous by a sharp 30-gauge needle that was inserted into the eye 4.0 mm posterior from the limbus. The needle was carefully removed, and a sterile cotton applicator was used to prevent reflux. The postoperative medications included topical antibiotics four times per day for at least 7 days, and antiglaucoma medications as needed.
Collecting blood samples
Samples of blood were collected just before the injection, and at 1 day, 7 days and 1 month after the injection of bevacizumab. The blood samples were collected in tubes containing EDTA and were immediately placed on ice. Platelet-poor plasma was prepared by centrifugation (3000 rpm, 20 min) and stored at −80°C before use.
VEGF and PEDF assay
Before the assay, the samples were thawed on ice. The concentration of VEGF in the plasma was measured with an ELISA Kit (Quantkine VEGF ELISA Kit, R&D Systems Inc., Minneapolis, Minnesota, USA) as previously reported9 11–14 according to the manufacturer's instructions. This assay uses a quantitative sandwich enzyme immunoassay technique. The PEDF level in the plasma was measured with an ELISA Kit (Chemikine PEDF Sandwich ELISA Kit, Chemicon International, Temecula, California, USA). The samples were diluted in assay diluent, then immediately applied to the assay plates and measured according to the manufacturer's instructions. The concentrations of VEGF and PEDF were determined by measuring the absorbance at 450 nm with a microplate reader (Titertek, Multiscan, Flow Laboratories Inc., Helsinki, Finland), and the values were compared with those obtained with standard dilutions (VEGF: range 0–2000 pg/ml, PEDF: range 0–1.25 ng/ml). The background absorbance was subtracted from all values.
Statistical analyses
The results are expressed as means (SEM), and the significance of any differences was determined by repeated-measures analysis of variance by ranks with Tukey's multiple comparison test. A p value <0.05 was accepted as significant.
Results
The mean VEGF concentration in the plasma of controls was 92.0 (13.5) (mean (SEM), range 0–172.8) pg/ml. The mean VEGF concentration of diabetic patients in the plasma before the intravitreal injection of bevacizumab was 114.0 (25.3) (range 41.4–351.1) pg/ml. It was significantly decreased after 1 day to 9.7 (3.7) (range 0–42.6) pg/ml (p<0.001) and after 7 days to 11.7 (2.4) (range 0.5–27.5) pg/ml (p<0.001). Even after 1 month, the VEGF level was significantly decreased to 25.9 (7.9) (range 0–91.4) pg/ml (p<0.001) and was still lower than that of the initial levels (figure 1, table 2).
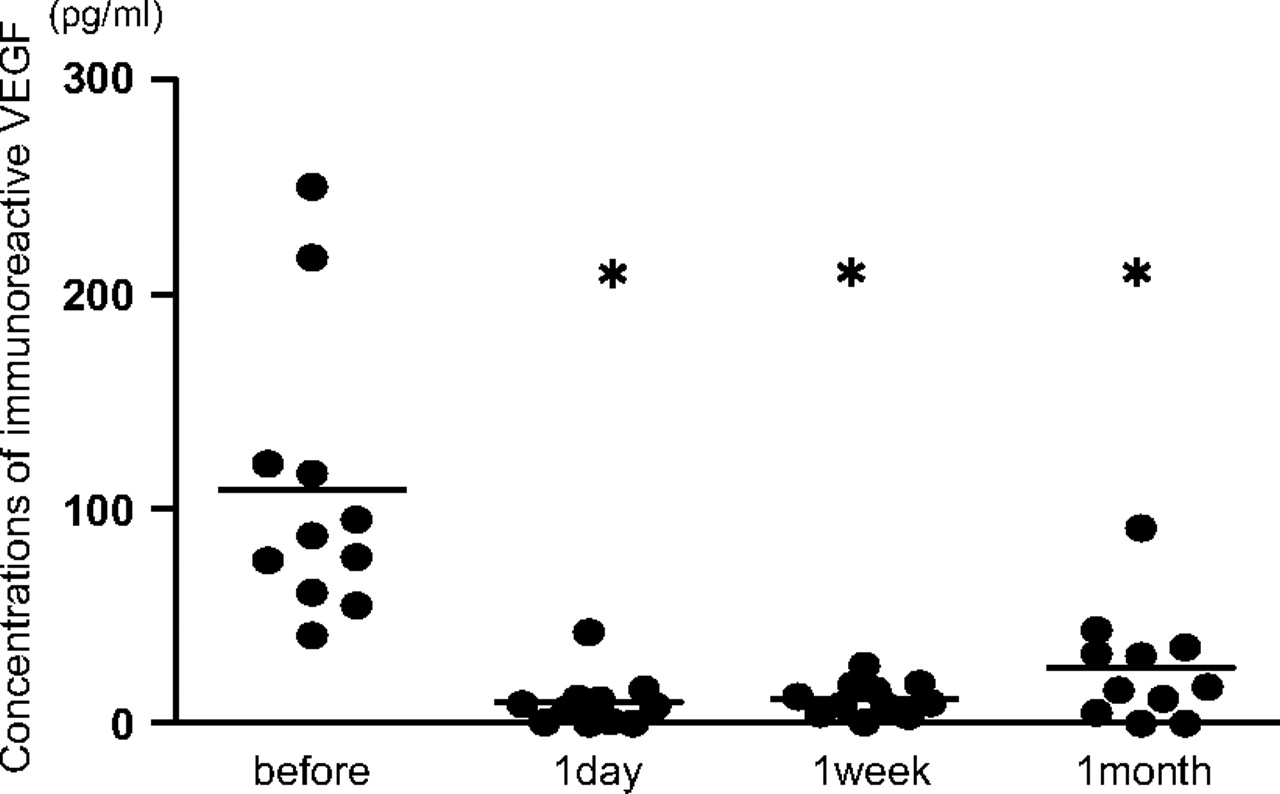
Plasma levels of VEGF before and after an intravitreal injection of bevacizumab. The mean VEGF concentration in the plasma before the intravitreal injection of bevacizumab was 114.0 pg/ml. It was significantly decreased after 1 day to 9.7 pg/ml (p<0.001) and after 7 days to 11.7 pg/ml (p<0.001). Even after 1 month, the VEGF level was significantly decreased to 25.9 pg/ml (p<0.001) and was still lower than that of the initial level. *=p<0.001.
Concentrations of immunoreactive VEGF in plasmas
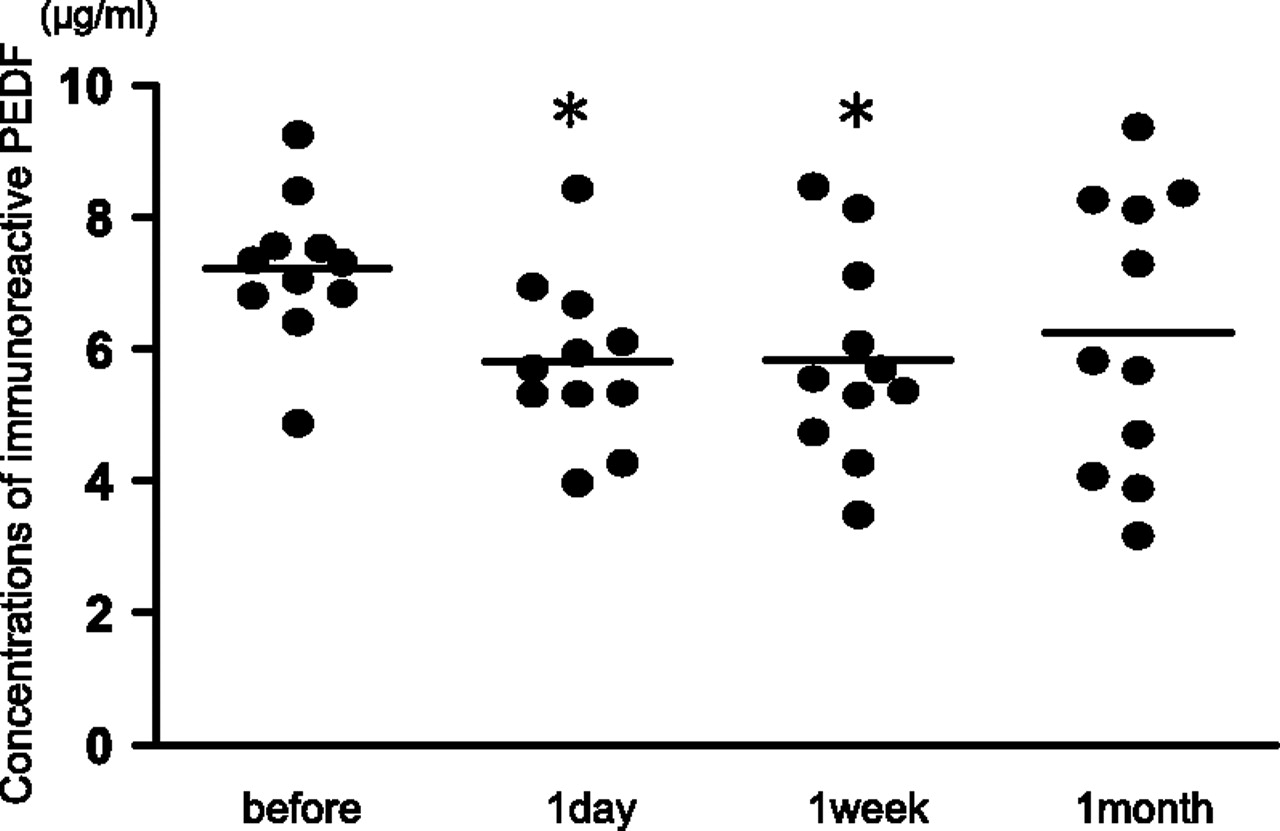
The mean PEDF concentration in the plasma of controls was 3.9 (0.3) (range 0.9–7.6) μg/ml (p<0.001). The mean PEDF concentration in the plasma of diabetic patients before the intravitreal injection of bevacizumab was 7.2 (0.3) (range 4.9–9.3) μg/ml (p<0.001). It was significantly decreased to 5.8 (0.4) (range 4.0–8.4) μg/ml (p<0.001) after 1 day and to 5.8 (0.5) (range 3.5–8.5) μg/ml (p<0.01) after 7 days. After 1 month, the PEDF level was 6.3 (0.6) (range 3.2–9.4) μg/ml (p>0.05). It was still lower than that of initial level, but the difference was not significant (figure 2, table 3).

{kind=link}
{kind=link}
Plasma levels of PEDF before and after intravitreal injection of bevacizumab. The mean PEDF concentration in the plasma before the intravitreal injection of bevacizumab was 7.2 μg/ml. It was significantly decreased after 1 day to 5.8 μg/ml (p<0.001) and after 7 days to 5.8 μg/ml (p<0.001). After 1 month, the PEDF level was 6.3 μg/ml (p>0.05). It was still lower than that of the initial level, but it was not significantly different. *=p<0.001.
Concentrations of immunoreactive PEDF in plasmas
Discussion
Bevacizumab is a human monoclonal antibody that binds to all isoforms of VEGF. Although experimental data on primates suggested that the full-length antibody might not penetrate the internal limiting membrane of the retina,15 recent studies have shown that the full-length antibody did penetrate into the rabbit16 and monkey retina17 within 24 h.
A significant improvement of the visual acuity and a resolution of neovascular vessels have been reported after an intravitreal injection of bevacizumab in eyes with increased intravitreal levels of VEGF—for example, neovascular glaucoma, diabetic retinopathy, age-related macular degeneration, macular oedema in associated with diabetic retinopathy and retinal vein occlusion.6–11
With the increasing use of bevacizumab for VEGF-mediated retinal diseases, it is important to know the VEGF levels in various tissues and its clearance after an intravitreal injection. After an intravitreal injection of bevacizumab, the VEGF levels in the aqueous have been shown to decrease in patients with diabetic retinopathy9 10 and choroidal neovascularisation.11 In humans, intravitreal bevacizumab (1.25 mg) is estimated to have a half-life of 6.7 days in the vitreous, and vitreous levels of free VEGF were negatively correlated with the bevacizumab concentration.18 Krohne et al19 reported that the aqueous half-life of 1.5 mg intravitreally injected bevacizumab was 9.82 days.
Although the VEGF levels and clearance of bevacizumab after an intravitreal injection have been reported for human eyes,9–11 18–20 to the best of our knowledge, published data are not available on the VEGF concentrations in blood before and after intravitreal bevacizumab in a human case series. In this study, we found a significant decrease of VEGF in the plasma after the intravitreal injection of bevacizumab at 1 day, 7 days and even at 1 month in patients with diabetic retinopathy. These results strongly indicate that intravitreally injected bevacizumab passes into the general blood circulation where it acts to decrease the level of VEGF.
Sawada et al13 reported that after an intravitreal injection of bevacizumab in one eye, the VEGF concentrations in the aqueous humour of the contralateral eye were not decreased. Thus, they suggested that the effect would be minimal or none on the contralateral eye. However, there is a report that the elimination of bevacizumab from the aqueous humour and serum were parallel with half-time values of 4.88 and 6.86 days after the intravitreal injection of bevacizumab in rabbits.21 Bakri et al21 reported that very small amounts of bevacizumab were detected in the fellow uninjected eye. In addition, Avery et al8 reported that some patients with bilateral proliferative diabetic retinopathy had regression of neovascularisation in both eyes when bevacizumab was injected intravitreally in only one eye. Their report also support our results that intravitreally injected bevacizumab can pass into the general blood circulation and result in a decrease in the levels of VEGF in the blood.
Heiduschka et al17 and Julien et al22 reported that after an intravitreal injection of bevacizumab in the primate eye, bevacizumab quickly penetrated into the retina, choroid, retinal veins and optic nerve. Immunoreactivity for bevacizumab was most prominent on day 1 after the injection.22 In addition, 125I-labelled bevacizumab was detected in the blood 1 day after the intravitreal injection and remained relatively stable until day 7.17 Bevacizumab penetrated quickly into the iris, anterior chamber angle and ciliary body after an intravitreal injection in the primate eye and accumulates particularly in the blood vessel walls.17 22 Our results showed that the blood level of VEGF was markedly reduced as early as 1 day after the intravitreal injection of bevacizumab.
Taken together, these findings indicate that intravitreally injected bevacizumab does penetrate into the retina, choroid, intraocular blood vessels and aqueous and quickly enters the general blood circulation. Bevacizumab then lowers the level of VEGF in the blood.
In addition to the VEGF levels, we measured the PEDF levels in the plasma after the intravitreal injection of bevacizumab. PEDF in plasma of controls (3.9 μg/ml) was lower than that of diabetic patients before intravitreal injections of bevacizumab (7.2 μg/ml). These data are coincident with previous reports that presented the plasma PEDF level in diabetic patients was significantly higher than that in controls, and the level was especially high in patients with proliferative diabetic retinopathy.23 24 We found that the PEDF levels were significantly reduced at 1 day and 1 week after the injection of bevacizumab. On the other hand, Chan et al11 reported that an intravitreal injection of bevacizumab increased the PEDF levels in the aqueous of patients with choroidal neovascularisation secondary to age-related macular degeneration or pathologic myopia. Our results on the PEDF levels disagree with their findings. The difference may be because of differences in the patients and samples. They measured samples of aqueous humour in patients with choroidal neovascularisation, whereas we measured the samples of blood in patients with diabetic retinopathy.
Administration of PEDF has been shown to effectively inhibit retinal neovascularisation.4 PEDF can counteract the VEGF-induced vascular permeability25 and suppress the VEGF-induced leukostasis.26 These findings indicated that PEDF acts as an inhibitor of VEGF function. Ohno-Matsui et al27 reported that VEGF up-regulates the PEDF expression by VEGFR-1 in human retinal pigment epithelial cells. Zhang et al28 reported that PEDF inhibits the expression of VEGF at the transcriptional level, and in contrast to the findings of Ohno-Matsui et al,27 VEGF significantly downregulated PEDF expression in retinal capillary endothelial cells, suggesting a VEGF receptor-mediated process. The exact mechanism for the interaction between VEGF and PEDF expression is still unknown. The mechanism of the decrease in PEDF concentration in the blood after bevacizumab injection is uncertain, but it would reflect the VEGF levels.
It has recently been reported that bevacizumab is not toxic to retinal ganglion cells after repeated intravitreal injections.29 Therefore, repeated intravitreal injections of bevacizumab might be safe for the retina. We do not know how much of the intravitreally injected bevacizumab passes through the eye to the general circulation. However, only a small amount of bevacizumab—for example, 1.25 mg/0.05 ml of a single injection, was enough to significantly reduce the VEGF levels in the blood and its effects lasted for at least 1 month. Thus, we suppose that with repeated injections of bevacizumab, its effect may last longer and the revascularisation will be delayed after cardiac infarct and arteriosclerosis obliterans as a result. Further studies with larger samples and longer follow-up will be necessary to determine the general effects.
In conclusion, although general complications have been reported to be rare after an intravitreal injection of bevacizumab, we should carefully examine patients for systemic changes especially those with multiple injections of bevacizumab.
Acknowledgments
This study was supported in part by a Grant-in Aid for Scientific Research from the Ministry of Education in Japan.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the institutional review committee of the Kansai Medical University.
Provenance and peer review Not commissioned; externally peer reviewed.