Article Text

Abstract
Background Tumour control of vitreous seeds remains challenging owing to their resistance to radiation and systemic chemotherapy.
Objective To describe the short-term efficacy of intravitreal melphalan for vitreous disease in retinoblastoma using a new injection technique and dose.
Methods This study is a retrospective non-comparative review of 23 consecutive heavily pretreated patients (23 eyes) with active vitreous seeding and eligible for intravitreous chemotherapy (IViC). They received a total of 122 intravitreal injections of melphalan (20–30 μg) given every 7–10 days. The ocular status was objectively monitored under anaesthesia with fundus photography.
Results All patients are alive without evidence of extraocular spread (95% CI 82.19% to 100%). Concomitant treatments, including other chemotherapeutic modalities, were used until complete sterilisation of the retinal seeding source and subretinal seeds. Globe retention was achieved in 87% (20/23) of cases. All retained eyes were in complete remission after a median follow-up period of 22 months (range 9–31 months). The Kaplan–Meier estimate of ocular survival rates at 2 years was 84.14% (95% CI 62.48% to 95.28%). A localised peripheral salt-and-pepper retinopathy was noted in 10 eyes (43%) at the site of injection.
Conclusions This study reports the first clinically documented case series of patients with retinoblastoma treated with IViC. Despite a possible confounding effect of concomitant chemotherapy prescription using other routes of administration in four of the successfully treated eyes (20%), IViC achieved an unprecedented success rate of tumour control in the presence of vitreous seeding. Of note, none of the treated eyes required external beam irradiation to control the vitreous seeding. Further studies are required to assess IViC retinal toxicity and to better delineate its role in the management of retinoblastoma.
Statistics from Altmetric.com
Introduction
The presence of vitreous and/or subretinal seeds in retinoblastoma at diagnosis significantly reduces the prognosis for tumour control and eye salvage.1 In such eyes, ocular survival barely reaches 50% when external beam radiotherapy (EBR) is used as first-line treatment.2 The outcome of group D eyes remains a challenge despite the introduction of primary systemic chemotherapy, with only 27–47% of the eyes not requiring enucleation and/or EBR.3–6 More recently, the advent of intra-arterial chemotherapy appears to significantly improve the prognosis for eye preservation (70–80%) of group D eyes.7–9 However, these results are still based on relatively short-term median follow-up and are in contrast with a long-term (median 74 months) success rate of only 45% in group D eyes after combined use of intra-arterial and intravitreal melphalan.10 In cases of vitreous relapse the prognosis for eye survival without radiotherapy may be as low as 20%.11
Intravitreal administration of chemotherapy for vitreous disease offers the opportunity of delivering the desired tumouricidal drug concentration within the vitreous cavity, but is associated with the risk of tumour spread. The use of intravitreal melphalan for vitreous seeding was first introduced in the 1990s by Kaneko and Suzuki, who treated 41 eyes with 8 μg melphalan and simultaneous hyperthermia using a Lagendijk applicator.12 At 50 months of follow-up the eye preservation rate was 51.3%. Unfortunately, details of the study population and the treatment modalities have not been published.
The choice of melphalan was based on in vitro studies by Inomata and Kaneko,13 who found this drug to be the most efficient among the 12 tested, achieving complete suppression of colony formation at a concentration of 4 μg/ml. Preclinical studies in albino rabbits14 have established that melphalan at a vitreous concentration of 5.9 μg/ml is functionally and structurally non-toxic to the retina. When extrapolated to the human vitreous volume, the injected rabbit dose corresponds to 20–30 μg to be injected depending on the patient's age.
We recently defined eligibility criteria for intravitreal chemotherapy injection in retinoblastoma, and described a safety-enhanced technique for intravitreal injection (IViC) using an antireflux procedure followed by sterilisation of the needle track.15 Here we describe the efficacy of our preliminary IViC procedure in 23 patients with vitreous seeding.
Patients and methods
This study was approved by the Swiss Federal Department of Health (authorisation # 035.0003-48) and is in accordance with the declaration of Helsinki. Twenty-three consecutive patients presenting vitreous seeding and eligible for IViC were included in this retrospective non-comparative study. This group consisted of five cases followed up in Lausanne since diagnosis and 18 cases referred for second opinion after treatment initiation elsewhere. Eligibility criteria for IViC as assessed by ultrasonic biomicroscopy (OTI Scan 2000 Ophthalmic Technologies, North York, Ontario, Canada) with 35 MHz transducers15 ,16 were as follows: (1) absence of invasion of the anterior and posterior chamber; (2) absence of anterior hyaloid detachment; (3) absence of retinal detachment at the entry site; (4) absence of tumour at the entry site and (5) absence of vitreous seeds at the entry site. All received outpatient IViC as an alternative to enucleation or EBR after informed consent was obtained from the parents.
An anterior chamber paracentesis was performed before melphalan injection. A volume of 0.1–0.15 ml (according to the calculated volume to be injected) of aqueous fluid was aspirated and sent for cytopathological analysis. A 32G needle mounted on a tuberculin syringe was then introduced perpendicularly 2.5–3.5 mm from the limbus at the desired meridian opposite to the seeds through the conjunctiva and sclera under microscope viewing until the needle tip reached the centre of the vitreous cavity. The injected dose was 20 μg in most cases but could be cumulatively increased by 2–4 μg up to 30 μg for each of the following situations: (1) age over 2 years; (2) diffuse nature and/or high density of the seeding; (3) previous intra-arterial exposure to melphalan and (4) relapse after previous IViC. Upon removal of the needle three cycles of freeze and thaw cryoapplications were applied at the injection site. The eye was then carefully shaken in all directions to enable even distribution of the drug. The ocular status at presentation and follow-up was objectively monitored under anaesthesia with fundus photography using RetCam (Clarity, Pleasanton, California, USA) and B-scan ultrasonography (OTI Scan 2000 Ophthalmic Technologies). At each visit the residual vitreous tumour burden was reassessed and IViC carried out every 7–10 days up to eight injections, if a response could be documented, until complete seed fragmentation was observed or complete response was achieved. Complete response was established if the seeds (1) completely disappeared (vitreous seeding regression type 0), or converted into (2) refringent and/or calcified residues (vitreous seeding regression type I), (3) amorphous often non-spherical inactive residues (vitreous seeding regression type II), or (4) a combination of the last two (vitreous seeding regression type III). An injection of consolidation was usually given once a complete response was observed. IViC could be repeated if vitreous recurrence occurred from another source. Simultaneously, focal treatments were applied to eradicate the retinal source of the seeding as well as all epiretinal and subretinal active tumours. The complications were systematically assessed before each injection by RetCam photography and in selected cases by RetCam angiography. The grading was restricted to the presence or absence of a localised peripheral retinopathy.
For injection, melphalan (Alkeran; GlaxoSmithKline, Italy) was supplied as 50 mg sterile, lyophilised powder with 10 ml special diluent containing povidone and propylene glycol for reconstitution. The packages were stored at room temperature (15–25°C), protected from light. The solution was prepared in a biological safety cabinet (level III). After reconstitution to 5 mg/ml the solution was shaken until a clear solution was obtained. Before administration, the solution was further diluted with preservative-free, pyrogen-free 0.9% sodium chloride to a concentration of 0.2 mg/ml of melphalan. One millilitre of this solution was further taken in a 1 ml sterile polypropylene syringe. The final dilution is stable for 3 h between 2°C and 8°C.
Actuarial enucleation-free survival rates were calculated using the Kaplan–Meier method. Statistical analyses were performed with the software JMP version 9.0 (SAS Institute Inc, JMP, SAS Campus Drive). Statistical analysis was conducted using the Wilcoxon test for non-parametric impaired data.
Results
Twenty-three eyes of 23 heavily pretreated patients (13 male and 10 female subjects) with vitreous seeding were included (table 1). Vitreous seeding was found to be localised (confined to one quadrant) in 13 eyes (56.5%) and diffuse (involving more than one quadrant) in the remaining eyes (43.5%). In addition to vitreous seeding, six eyes also had subretinal seeding (table 1). The study population consisted of 18 bilaterally affected patients, 10 of whom had only one eye, and five patients with unilateral retinoblastoma. At presentation 11 eyes had group D, nine eyes group C and three eyes group B disease with a median age at diagnosis of 12 months (range 0.25–41 months). IViC was proposed as an alternative to external beam irradiation or enucleation according to two distinct indications: (1) as salvage treatment for recurrent seeds in 17 eyes (74%), where the relapse of vitreous seeds could be documented despite all prescribed treatments (figure 1), or (2) as second-line treatment for resistant seeds in six eyes (26%) where vitreous seeds persisted with no regression (figure 2) after completion of three courses of intra-arterial chemotherapy (two eyes) or after discontinuation of intra-arterial chemotherapy after the first or the second injection due to side effects, including Purtcher-like retinopathy (one eye), transient spasm of the internal carotid artery (one eye) and transient pigmentary erythema respectively (one eye). Median age at first injection was 29 months (14–71 months).
Eye-level characteristics of the study population

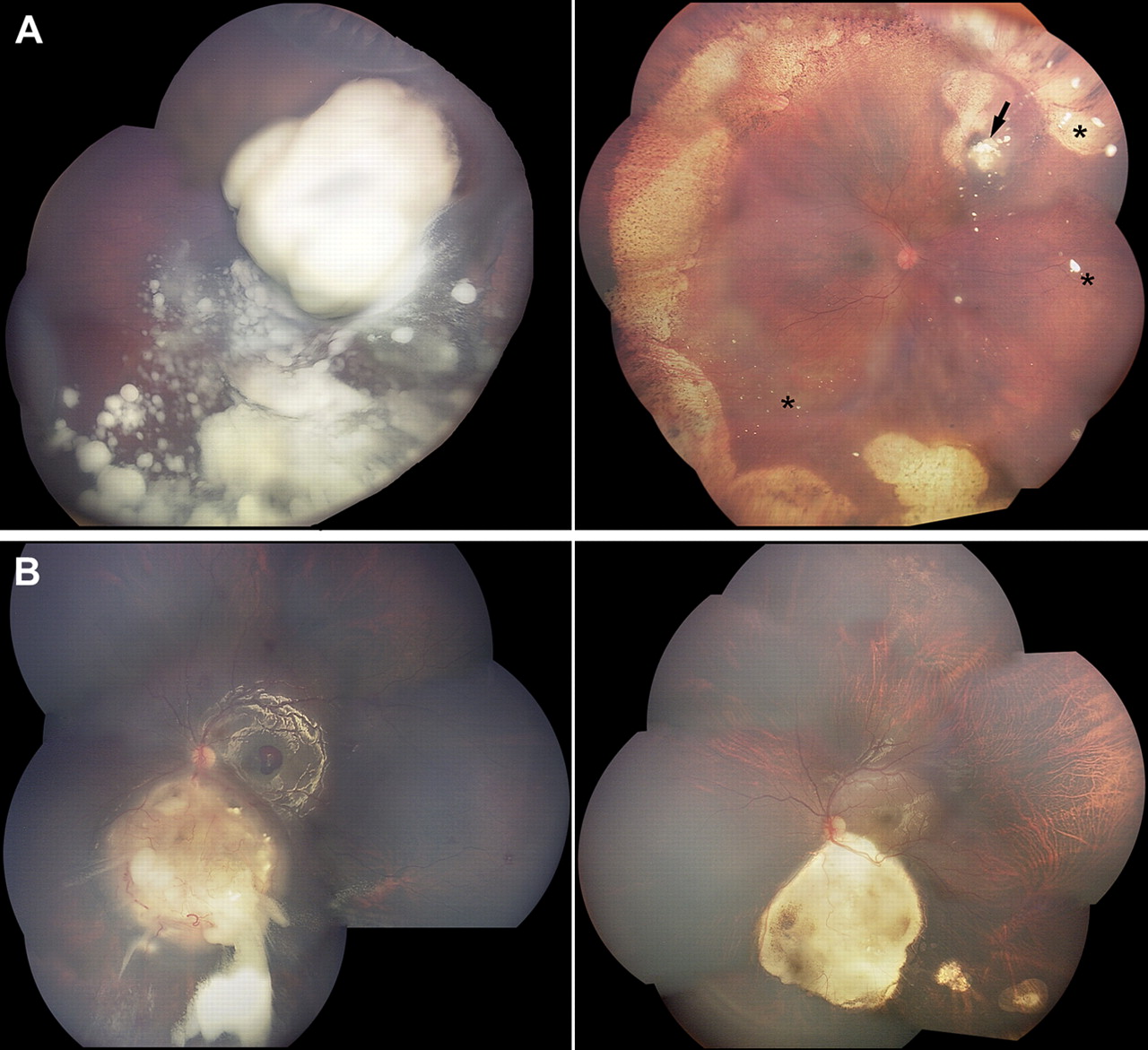
Fundus montage showing diffuse vitreous and subretinal relapse after multiple courses of intravenous and intra-arterial chemotherapy before (left) and after intravitreous chemotherapy (IViC) (right) in patients No 21 (A) and No 23 (B). The black arrow indicates the retinal source of the vitreous seeding. White triangles highlight the largest subretinal seeds. White arrows point to the largest vitreous (and epiretinal) seeds.
{kind=link}
{kind=link}
Fundus montage showing persistent vitreous seeding after one course of intra-arterial chemotherapy before (left) and after (right) intravitreous chemotherapy (IViC) in patients No 2 (A) and No 10 (B). The black arrow indicates the residual primary tumor. Black asterisks show areas with epiretinal calcified debris.
A total of 122 intravitreal injections of melphalan were given without any visible reflux during the procedure carried out under the microscope. Cytopathological examination of the anterior chamber fluid was negative in all cases. Complete fragmentation of vitreous seeds or response could be documented after a median of four injections2–12 in 21 eyes (91.3%), including one eye subsequently enucleated for phthisis bulbi. The remaining 20 eyes still show complete response at the last visit, with a median follow-up from first injection of 22 months (9–31 months).
The phenotypic characteristics of seeding after complete response (table 1) varied from vitreous seeds regression type 0 (complete suppression of seeds) in 14/21 eyes (67%) to various seeds inactivation patterns, including vitreous seeds regression type I in four eyes (19%), and type II or III in three eyes (14%). The diffuse versus localised nature of the seeding at presentation was not a significant predictor of the response with respect to the suppression or inactivation regression patterns. In three eyes, a second occurrence of localised vitreous tumorous dispersion was seen at a distinct location. In one eye (case 1), new vitreous seeds were produced by a distinct retinal source 7 months after a first course of five injections and this was finally controlled by a further four injections associated with a ruthenium plaque. In the other two eyes, the secondary vitreous involvement was iatrogenic in nature and occurred, respectively, 4 and 10 months after eight and four melphalan injections succeeded in controlling the initial localised vitreous disease (cases 9 and 16). In both cases the second vitreous dispersion of tumour cells was noted when the tumour apex ruptured at the time of plaque surgery. These patients received four and two additional melphalan injections, respectively, with complete response (vitreous regression type 0), initiated at plaque removal (ie, before evidence of vitreous growth).
All together, we treated a total of 26 vitreous events; comparison of the number of injections required to obtain control of the vitreous disease for recurrent versus persistent seeds did not show a significant difference. However, when the diffuse versus localised nature of the seeds was compared the difference reached statistical significance (p<0.02), with a median number of injections of 6.5 (3–8) versus 3.5 (2–8), respectively.
Concomitant focal treatments aimed at sterilising the retinal source of the seeding as well as subretinal seeds were necessary in all patients except two (cases 15 and 18), with a median event-free interval (since final treatment) of 16 months (3–24 months). The majority of them received non-chemotherapeutic modalities, such as ruthenium plaques in five eyes and/or focal treatments (cryotherapy, thermotherapy) in 19 eyes. In six eyes, the extent of active retinal tumours (four eyes) and subretinal seeding (two eyes), led to the use of additional routes of chemotherapy delivery, including ophthalmic artery infusion of melphalan in two eyes, chemothermotherapy (intravenous carboplatin) in one eye, periocular topotecan in two eyes and a combination of the last two methods in one eye. Control of the vitreous seeding was not enhanced in this subgroup compared with the eyes treated by IViC alone.
Stereotactic conformal radiotherapy of the posterior pole was required in two eyes with residual active papillary tumour and recurrent macular tumour in an only eye, respectively (and not because of the vitreous seeding). Three eyes (including one of the latter) were enucleated after a median retention time of 11 months (9–15 months) owing to phthisis bulbi in one case, and to disease progression in the other two cases secondary to loss of follow-up. When examined again 4.5 and 6 months later, respectively, the two latter patients already had a blind eye filled with tumour, and were subsequently enucleated. They received four cycles of adjuvant chemotherapy owing to the presence of massive choroidal invasion, associated in one of them with retrolaminar optic nerve invasion but tumour-free surgical section. Both patients are alive, and without relapse at their last visit (28 and 21 months, respectively). The Kaplan–Meier enucleation-free survival rates were 100% (95% CI 82.19% to 100%), 90.15% (95% CI 69.48% to 98.15%) and 84.14% (95% CI 62.48% to 95.28%, SE 0.085), at 6, 12 and 24 months, respectively, with a steady state reached at 15 months.
Successful operations were carried out for three IViC-unrelated treatments—one eye with radiation-induced cataract (after two iodine plaques) and two eyes with rhegmatogenous retinal detachment. Retinal and iridal neovascularisation secondary to ischaemic retinopathy could be controlled in one of two eyes (cases 5 and 13) treated with a single intravitreal anti-vascular endothelial growth factor injection (0.5 mg of ranibizumab).
Retinal toxicity appeared to be limited to the site of injection in the form of a peripheral well demarcated salt-and-pepper retinopathy (figure 1) in 10 eyes (43%). A transient localised vitreous haemorrhage in two eyes (8.5%) was the only ocular complication seen. Specifically IViC was not found to cause corneal endothelium insufficiency, cataract (one case was radiation-induced), uveitis, endophthalmitis, or retinal detachment (the two above-mentioned cases of rhegmatogenous retinal detachment were linked to retinal breaks posterior to a calcified tumour) during the follow-up period.
There was no evidence of exteriorisation and/or tumour spread (95% CI 82.19% to 100%).
Discussion
As far as we know, our report is the first clinically documented case series of patients with retinoblastoma with vitreous seeding treated with IViC. We have shown that this injection technique can be applied under optimised security conditions in a selected subgroup of eligible heavily pretreated patients with retinoblastoma with active vitreous seeding. Specifically, there was neither epibulbar exteriorisation nor metastasis observed within the median follow-up period of 22 months (95% CI for no event). Retinal toxicity, in the form of localised salt-and-pepper retinopathy, appears to be restricted to the peripheral area around the injection site, indicating a higher melphalan concentration at this level and thus further increasing the security against tumour spread. Although our study did not examine potential retinal toxicity away from the injection site, there was no evidence for a detrimental functional effect of IViC at least with the present doses (data not shown).
For the efficacy of IViC, we report a success rate of 83% (19/23), defined as absence of vitreous and/or epiretinal relapse as well as absence of enucleation and/or EBR, despite the fact that two of the failures were due to loss of follow-up. Interestingly, the two irradiated eyes received conformal stereotactic irradiation confined to the posterior pole17 for recurrent macular and papillary tumors, respectively, and not for vitreous seeding, which was completely controlled in both cases. These results are in striking contrast with the literature, which does not exceed 61%18 using intravenous chemotherapy and ciclosporin. Recently, Abramson et al7 reported a success rate of some 66% in eyes with recurrent vitreous seeding treated by intra-arterial chemotherapy with melphalan. Although subretinal seeding seems to be sensitive to IViC, this could be demonstrated for one eye only that had no other treatment during or after IViC (case 15).
Ericson and Rosengren19 were the first to use intravitreal injections of thiotepa as heroic treatment in six only eyes with recurrent vitreous disease. This initial experience was pursued more than 30 years later by Seregard et al20 who treated three eyes using the same approach. More recently, Kivela et al21 reported the use of intravitreal methotrexate in five eyes from four patients with relapse following chemoreduction, only one of the four patients having vitreous seeding. Each eye received 20–27 injections of methothrexate over a period ranging between 10 and 12 months, versus 2–8 injections of melphalan within a 2–12 week period in our study.
Since their initial pioneering report,12 Kaneko and Suzuki have performed 896 IViCs in 237 eyes of 227 patients.22 They reported the occurrence of extraocular subconjunctival extension in one eye (0.4%), which had anterior chamber involvement and dense vitreous seeds. The patient received adjuvant chemotherapy after enucleation and is reported to be in complete remission. Among the 10 patients (4.4%) who developed metastases, IViC was potentially related to 1 (0.4%). However, it should be emphasised that the Japanese experience significantly contrasts with our study both in its IViC eligibility criteria and injection technique. Specifically, the absence of well-defined contraindications, as well as the lack of antireflux measures and needle tract sterilisation, despite injected volumes of 0.1–0.2 ml, might have contributed to the incidence of the reported adverse events.
Although IViC appears to offer a safe and efficient salvage option, its validation awaits the results of a prospective phase II clinical trial. Special attention will be paid to retinal toxicity assessed by electroretinogram, fluorescein angiography and optic coherence tomography. If validated, IViC may prove to be useful as salvage treatment for recurrent or resistant vitreous seeds, and also useful as a prophylactic measure in cases of iatrogenic seeding after photocoagulation and plaque surgery, or second-line treatment for group B eyes with ruptured internal limiting membrane (as assessed by fluorescein angiography)—that is, presumptive submicroscopic infraclinical vitreous disease at presentation. Finally, we want to emphasise that although IViC does not replace standard treatment care for group C and D eyes, we expect that addition of front-line IViC to state of the art treatment in eligible group C and D eyes may significantly reduce the exposure to systemic chemotherapy, as well as the indications for enucleation and/or EBR.
Acknowledgments
We thank Susan Houghton for data management and manuscript editing, Dr Leila Moetteli for statistical analysis and Yann Leuba for the production of composite photographs.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
Footnotes
Linked articles 301016.
Presented in part as “Retinoblastoma Keynote Lecture” at the XVth Biannual Meeting of the International Society of Ocular Oncology, Buenos Aires, Argentina, 14–17 November 2011
Funding This study was supported by a grant from the Foundation Conteurs San Frontières.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by Comité d'Ethique Cantonale.
Provenance and peer review Not commissioned; externally peer reviewed.