Article Text

Abstract
Background The preservation of globe integrity has always been a major concern during the treatment of retinoblastoma for fear of extraocular or metastatic spread. Intravitreal chemotherapy has been attempted as a desperate salvage therapy only for eyes with refractory retinoblastoma. Published data on the safety and efficacy of this route are, however, limited.
Methods A modified technique of intravitreal injection in eyes with retinoblastoma is described. All children with retinoblastoma who received one or more intravitreal injections using this technique were retrospectively reviewed concerning ocular complications of the injection procedure as well as clinical or histopathological evidence of tumour spread.
Results 30 eyes of 30 children with retinoblastoma received a total of 135 intravitreal injections, with a median follw-up duration of 13.5 months. No extraocular spread was seen on clinical follow-up in any patients and there was no tumour contamination of the retrieved entry sites histopathologically analysed among the five enucleated eyes. No significant ocular side effects were observed except transient localised vitreous haemorrhage (3/135).
Conclusion This technique is potentially safe and effective at a low cost and may play a promising role, especially in the treatment of recurrent and/or resistant vitreous disease in retinoblastoma, as an alternative to enucleation and/or external beam radiotherapy. However, this treatment should not replace the primary standard of care of retinoblastoma and should not be considered in group E eyes. Its application should be approved by an ophthalmological-oncological team and it should be performed by an experienced eye surgeon in a tertiary referral centre after careful selection of a tumour-free injection site.
- Anatomy
- angiogenesis
- chemotherapy
- intravitreal injection
- macula
- melphalan
- neoplasia
- pathology
- retina
- retinoblastoma
- surgical technique
- telemedicine
Statistics from Altmetric.com
- Anatomy
- angiogenesis
- chemotherapy
- intravitreal injection
- macula
- melphalan
- neoplasia
- pathology
- retina
- retinoblastoma
- surgical technique
- telemedicine
One of the main principles governing conservative treatment of intra-ocular retinoblastoma has always been the preservation of eye wall integrity throughout the active therapeutic phase. In other words, the idea of any eye-perforating procedures for diagnostic or therapeutic purposes has been strongly rejected due to the risk of spreading highly malignant cells outside the globe.
These views are supported by reports in the literature describing either orbital or metastatic disease following intra-ocular surgeries in unsuspected retinoblastoma, such as pars plana vitrectomy, glaucoma and cataract surgery.1 The risk of spreading tumour cells is linked to the potential reflux of ocular fluids contaminated with viable tumour cells mostly during long lasting open sky interventions at atmospheric pressure, or the use of continuous intra-ocular irrigation systems with positive pressure.
In contrast, fine needle aspiration biopsy (FNAB) in the context of atypical presenting cases of retinoblastoma is a short procedure, characterised by negative pressure, and there is therefore virtually no reflux except possible tumour cell contamination along the needle tract. Occasional tumour seeding in the needle track has been documented ex vivo in postenucleation FNAB.2 ,3 The in-vivo viability of the spilled tumour cells remains questionable, as no recurrence in extraocular tissues has been reported in the literature following the introduction of 25G FNAB,4 with the exception of one unpublished case.5
Despite an obvious risk of reflux, intra-vitreal injections of various chemotherapeutic drugs, including thiotepa,6 ,7 melphalan8 ,9 and methotrexate,10 have been performed as heroic therapies only in eyes with recurrent vitreous disease without any report of exteriorisation. In all these studies virtually no prophylactic treatment measures were taken to treat an anticipated extraocular spread (see supplementary table I, available online only).
The literature owes Kaneko and Suzuki8 the pioneering role in intravitreal chemotherapy (IVC) for publishing the largest series of IVC treatments in eyes with retinoblastoma since the 1990s, with the longest follow-up of over 7 years.9 However, a detailed description of the study population, as well as the treatment modalities of IVC were not published.
Here we describe a modified technique for intravitreal injections with multiple safety precautions to limit the possibility of the extraocular spread of tumour cells along the track of injection, as well as the short-term safety of intravitreal injections in eyes with retinoblastoma regarding the complications of injection and exteriorisation.
Methods
The current work is a retrospective, single centre, non-comparative, interventional clinical review of consecutive patients injected between September 2005 and August 2011 at Jules-Gonin Eye Hospital in Lausanne, Switzerland. This review was approved by the Swiss Federal Department of Health (authorisation no 035.0003-48) and is in accordance with the Declaration of Helsinki.
All eyes with retinoblastoma that received one or more intravitreal injections as a salvage procedure during or after the course of treatment were included. The type of drug and the indication were reviewed. Ocular complications and the occurrence of tumour spread were monitored, based on the monthly follow-up visit under narcosis, clinical oncopaediatric evaluation, and the careful histopathological examination of the needle entry sites when secondary enucleation was required.
Description of the procedure
Eligibility criteria
Indication for IVC must fulfil the following conditions as assessed by ultrasonographic biomicroscopy exploration of the pars plana: (1) the presence of clear media; (2) the absence of invasion of the anterior and posterior chamber; (3) the absence of tumour at the entry site; (4) the absence of vitreous seeds at the entry site; (5) the absence of retinal detachment at the entry site (figure 1A–D).

Examples of ultrasonographic biomicroscopy-based ineligibility criteria. (A) Presence of tumour cells in the posterior chamber. (B) Presence of tumour at the entry site. (C) Presence of vitreous seeds at the entry site. (D) Presence of a retinal detachment at the entry site.
Injection technique
The whole procedure was conducted under microscope viewing through a dilated pupil and general anaesthesia (see supplementary video, available online only).
Creating a transient hypotony
An anterior chamber paracentesis was performed through a clear cornea limbus track created with a 25G MVR blade without perforating Descemet's membrane. A 32G needle mounted on a tuberculin syringe was then introduced through the track tangentially into the anterior chamber peripherally and parallel to the iris. A volume of 0.1–0.15 ml (according to the calculated volume to be injected) of aqueous fluid was aspirated and sent for cytopathological analysis. There should be no leakage at the site of paracentesis when the needle is withdrawn.
Injection
The site for IVC was chosen 2.5–3.5 mm from the limbus at the desired meridian. A 32G needle (figure 2) mounted on a tuberculin syringe was then introduced perpendicularly through the conjunctiva and sclera until the needle tip reached the centre of the vitreous cavity. The calculated volume was injected as a bolus in 5 s under visualisation of the needle tip.

Example of two commercially available needles of 25 and 32G, respectively.
Management of the needle track
Three cycles of freeze and thaw (6 s each) are applied without indenting the eye at the injection site at the time of removal of the needle.
Final measures
Then the eye was held with conjunctival forceps at the anterior insertion of Tenon's capsule 1 mm from the limbus and was shaken in all directions for few seconds without pressure on the globe in order to improve drug distribution within the vitreous cavity. The eye was protected by a transparent plastic shield and put under topical antibiotics (chloramphenicol) and steroids (dexamethasone phosphate) three times a day for 1 week.
Results
The study included 30 eyes of 30 consecutive patients having undergone extensive treatments, including neoadjuvant intravenous chemotherapy (30 patients), intra-arterial chemotherapy (15 patients), periocular chemotherapy (eight patients), brachytherapy (six patients), two external beam irradiation (two patients) and focal therapies (30 patients). This population consisted of 15 boys and 15 girls with unilateral lesions in eight patients and bilateral lesions in 22 patients (13 of them with one residual eye). These patients received a total of 135 intravitreal injections (range 1–10 injections/patient) for vitreous seeding (melphalan n=124; carboplatin n=2) or for ischaemic retinopathy (ranibizumab n=9). The procedure was performed uneventfully in all cases. In particular, there was no visible leakage after removal of the 32G needle. Cytopathological examination of the anterior chamber fluid was negative in all cases. A transient localised vitreous haemorrhage was seen following three injections (3/135). There were no early postoperative complications such as ocular hypertension, uveitis, endophthalmitis or traumatic cataract, nor long-term complications such as retinal detachment. No cases of extraocular recurrence or systemic spread occurred during a median follow-up period of 13.5 months (range 1–66 months).
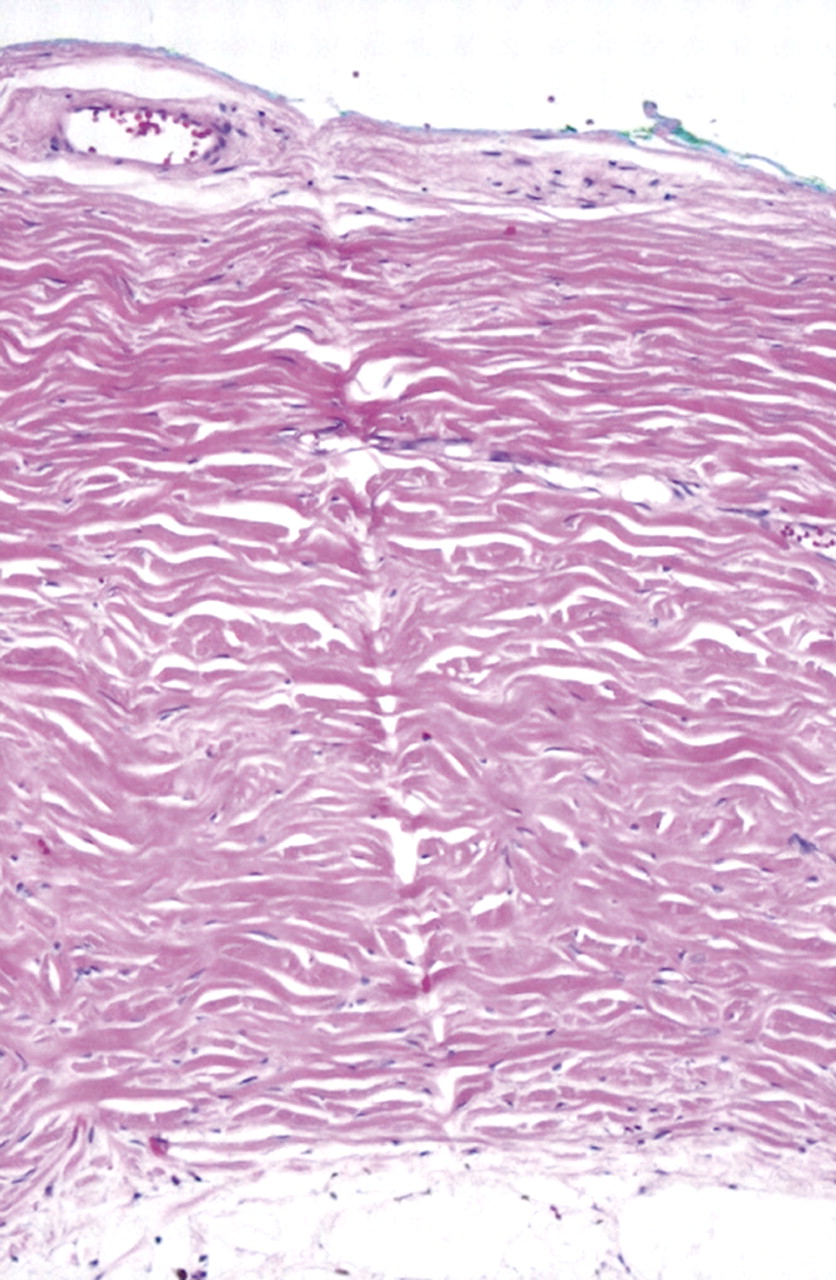
Five eyes were ultimately enucleated after a median retention time of 11 months (range 2–14 months). None of the six entry sites histopathologically studied contained tumour cells (figure 3). The mean diameter of the needle tract scar was 10 microns (range 7–13 microns). Adjuvant chemotherapy following secondary enucleation was required in two of the five enucleated patients, due to the presence of choroidal invasion on histopathology. For the remaining 25 patients (25 eyes), two are currently receiving further treatment, while 23 presented an event-free median follow-up of 9 months (range 1–55 months).

{kind=link}
{kind=link}
{kind=link}
Histopathological assessement of 32G needle tract in an enucleated eye 3 months after injection. A linear scar (10 μm diameter) can be observed throughout the sclera. The entry site is situated on the left. H&E; original magnification, ×63.
Discussion
There are at least five parameters possibly responsible for the risk of extraocular tumour growth following an invasive ocular procedure, namely: (1) the number and size of entries; (2) the presence of a tumour at the needle entry site: (3) a gradient of pressure across the sclera during the procedurel (4) the excessive duration of the exposure; and (5) the potential spilling of tumour cells along the scleral entry site.
By systematically addressing all five parameters, the present technique is expected to offer an unparallelled safety level with regard to tumour spread. In particular, the initial step consisting of producing controlled hypotony by the aspiration of aqueous fluid through a paracentesis efficiently prevents any reflux on intravitreal injection, provided that the aspirated and injected volumes are nearly equivalent. Assuming that the injection is performed at an established tumour-free pars plana site minimises the potential adherence of tumour cells on the needle surface, not forgetting the effect of the antimitotic drug injected moving the nearby vitreous cells and seeds away from the needle. The selection of the injection site is a critical step that must be ultrasonographic biomicroscopy-assisted if there is any doubt about the anterior tumorous extension.11 ,12 The use of a 32G needle creating a minimal scleral aperture of only approximately 10 microns (figure 3) and the short duration of the procedure (10 s for the positioning of the needle and 5 s for the injection per se) reduce the risk of exteriorisation. The absence of external pressure or indenting during the procedure is also helpful in this regard.
Finally, the sterilisation of the needle tract by triple freeze and thaw cryoapplications increases the safety profile of the procedure. This cryoprophylaxis was preferred to a sub-Tenonian deposition of a small amount of chemotherapeutic agent at the injection site, assuming a possible negative effect of the antimitotic drug on scleral healing. Also, the ballooning of the conjunctiva by the injected drug could spread any spilled cells. In addition, the short half-life of antimitotic drug under Tenon's capsule cannot prevent later exteriorisation of tumour cells that might have contaminated the needle track.
Chévez-Barrios et al13 described a technique of intravitreal delivery of a virus vector for gene therapy preceded by paracentesis, which entails a peripheral corneal entry with a 30G needle through the peripheral iris and the lens zonules, sparing the lens and entering the vitreous cavity. Upon retraction of the needle, cryoapplication on the corneal needle track was performed. We think that our technique should be safer as we do not rupture the anterior hyaloid face, thus avoiding the risk of transferring active tumour cells into the anterior segment of the eye.11
In conclusion, our technique is easy and with a steep learning curve that provides a potentially safe alternative to enucleation and/or external beam radiotherapy in the treatment of diffuse vitreous disease. IVC may play a role as salvage treatment in the case of residual vitreous seeding following first line therapy after complete sterilisation of the primary source of seeds. Intravitreal injections of anti-vascular endothelial growth factor could also represent a valuable therapeutic option only in eyes with controlled tumours and neovascularisation from ischaemic retinopathy. As a rule, IVC should not be considered as a therapeutic option unless the following checklist is fulfilled: (1) the indication is discussed within the multidisciplinary retinoblastoma team of the referral centre; (2) the procedure is performed by an experienced eye surgeon; (3) the meridian for the injection is carefully selected as a tumour-free site with good visibility; (4) the contraindications are ruled out (eg, retinoblastoma cells anterior to the anterior hyaloids, group E eyes). More importantly, this treatment must not be used as a primary treatment of retinoblastoma and does not replace the primary standard of care of retinoblastoma.
In summary, IVC is of low cost compared with other available salvage treatments such as ophthalmic artery chemotherapy or external beam radiotherapy, and its safety and efficacy merit further exploration and confirmation by a prospective clinical trial.
Acknowledgments
The authors are grateful to Marc Curchod and Yan Leuba for preparing the iconography, and Suzan Houghton in charge of the data management of retinoblastoma.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online video
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online video
Footnotes
Linked article 300829.
Competing interests None.
Patient consent Obtained.
Ethics approval This review was approved by the Swiss Federal Department of Health (authorisation no 035.0003-48) and is in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.