Article Text

Abstract
Purpose To evaluate objectively intraocular scattering in eyes with nuclear, cortical and posterior subcapsular cataracts by means of an objective scatter index (OSI) obtained from double-pass images. To compare the results with those obtained using clinical conventional procedures.
Methods In this prospective, observational, cross-sectional, non-consecutive case series study, 188 eyes with cataracts of 136 patients were analysed (123 eyes had nuclear, 41 eyes had cortical and 24 eyes had posterior subcapsular cataracts). The control group consisted of 117 eyes of 68 healthy patients. Patient examination included subjective refraction, best spectacle-corrected visual acuity (BSCVA), cataract grade using the lens opacities classification system III (LOCS III) and OSI.
Results We found a decrease in the BSCVA and an increase in the OSI with increasing cataract grade. Statistically significant differences were observed when the OSI of eyes without cataracts and those with different LOCS III were compared. The comparison between the OSI and LOCS III reported good percentages of agreement regarding the number of eyes classified in equivalent levels: 72.4% (nuclear cataracts), 86.6% (cortical cataracts) and 84.3% (posterior subcapsular cataracts). A non-linear regression model was applied between OSI and BSCVA, which resulted in the following multiple correlation coefficients: r=0.878 (nuclear), r=0.843 (cortical) and r=0.844 (posterior subcapsular).
Conclusions The results of the study showed that OSI is a useful parameter for evaluating large amounts of intraocular scattering that can be used, in combination with other conventional procedures, as a valuable tool in clinical practice to grade cataracts objectively.
- Cataract
- cornea
- double-pass technique
- epidemiology
- imaging
- intraocular scattering
- ocular surface
- optical quality
- optics and refraction
- physiology
- psychophysics
- treatment surgery
- vision
- visual perception
Statistics from Altmetric.com
- Cataract
- cornea
- double-pass technique
- epidemiology
- imaging
- intraocular scattering
- ocular surface
- optical quality
- optics and refraction
- physiology
- psychophysics
- treatment surgery
- vision
- visual perception
Introduction
The evaluation of the patient's vision before cataract surgery is carried out by running visual acuity and contrast sensitivity tests. However, procedures that measure other aspects of a patient's quality of vision exist. One such procedure consists of a test surrounded by a glare source that detects media disturbances to evaluate disability glare.1 ,2 Another procedure assesses retinal straylight using a device based on a psychophysical direct compensation approach (C-Quant, Oculus GmbH, Wetzlar-Dutenhofen, Germany).3 A new test has been proposed for measuring the visual discrimination capacity in a dim environment and is used in patients with different ocular pathologies4 and after refractive surgery.5 The results suggest that it can be useful to account for scattered light. These procedures, which capture the impact of forward scattering in vision, require the active participation of the patient, so the results may present a subjective component.
Other procedures involve the observation of the lens through a slit lamp from which a gradation of the state of every cataract is assessed. The most standardised system is the lens opacities classification system III (LOCS III).6 They provide information related to the back-scattered light and not forward scattering, which is responsible for the degradation of vision.
The results obtained using LOCS III may show variability among physicians.7 To overcome this, attempts have been made to classify cataracts objectively using Scheimpflug imaging,8 optical coherence tomography9 among other methods. The results suggest that this instrumentation can help in characterising grades of cataracts from a density or anatomical point of view although not from a functional point of view.
As an alternative approach, the double-pass technique is a useful tool for evaluating cataracts. It is a procedure used in clinics to assess ocular optical quality,10 and is able to capture the complete optical information of the eye, including the effect of higher-order aberrations and intraocular scattering within a small visual angle.11 ,12 It has been used successfully in patients with keratitis and uveitis,13 ,14 and those undergoing refractive surgery.15–17
Some attempts have been made to use the double-pass as a means of estimating scattering. Westheimer and Liang18 proposed a combined analysis of double-pass images and subjective measurements. However, they did not evaluate the contribution of aberrations and the procedure was not applied in eyes in which scatter was the main cause of degraded vision. Artal et al19 have recently proposed a new objective scatter index (OSI) calculated from double-pass images for estimating scattering with the intention to grade cataracts. The advantage is that it mainly accounts for the forward-scattered light and its validity has been analysed in several studies.20 ,21 Artal and co-workers19 established a classification based on the OSI for eyes with different degree of scattering taking into account the results obtained for 38 eyes with diagnosed nuclear cataracts. In this study we present a similar analysis in a larger number of eyes presenting different types of cataracts: nuclear, cortical and posterior subcapsular. We establish a quantitative comparison between the OSI and the results obtained using conventional procedures such as visual acuity and LOCS III.
Patients and methods
Patients
This prospective, observational, cross-sectional, non-consecutive case series study included the analysis of 188 eyes of 136 patients with different types and grades of cataracts (123 nuclear, 41 cortical and 24 posterior subcapsular cataracts). One hundred and seventeen eyes of 68 healthy patients were included in the study as a control group. Examinations were performed by three physicians (MJR, AS, JLG) at the Hospital Universitari Mútua de Terrassa, the University Vision Centre (Terrassa) and the Instituto de Microcirugía Ocular (Barcelona) from September 2008 to May 2010. All patients provided written informed consent before any examination and ethical committee approval was obtained. The Declaration of Helsinki tenets of 1975 (as revised in Tokyo in 2004) were followed throughout the study.
Cataract classification and clinical examination
Patients included in the study did not report any ocular alteration other than the cataract itself. Eyes with corneal opacities, anterior segment diseases, abnormal posterior pole evaluation, intraocular pressure values over 21 mm Hg, abnormal tear film and previous ocular surgery were excluded. Only eyes with a low to moderate grade of cataract on the LOCS III were included: from NO1 to NO3 (nuclear opacities), from C1 to C3 (cortical cataracts), and from P1 to P3 (posterior subcapsular cataracts). Patients with higher gradations were excluded from the analysis because a posterior pole evaluation could not be properly carried out due to the lack of transparency of the lens. The inclusion criterion for the control group was restricted to eyes with a best spectacle-corrected visual acuity (BSCVA) equal to or higher than 20/20.
Patient evaluations included determining the subjective refraction and measuring the BSCVA with a standard logMAR visual acuity test at 4 m. Cataracts were graded at the slit lamp after dilating the pupil by instilling 0.2 ml tropicamide (1%) using the LOCS III.
Intraocular scattering measurements
The protocol included an assessment of scattering using the OSI, which is a dimensionless parameter estimated from double-pass images acquired with the optical quality analysis system (OQAS 2; Visiometrics S.L., Terrassa, Spain). This is a clinical instrument based on an asymmetric configuration.22 The OSI is not significantly affected by refractive errors if these are corrected better than 1.0 D of spherical equivalent.
Artal et al19 established the following classification: OSI below 1 correspond to normal eyes with low amounts of scatter, between 1 and 3 to older eyes with associated scatter of an early cataract, between 3 and 7 to developed cataracts that should undergo surgery, and higher than 7 to eyes with severe cataracts.
In this study, measurements were carried out without dilation and using a pupil diameter of 4 mm. As the optical quality may be dependent on the tear film quality, measurements were taken just after a blink.23 The spherical refractive error was automatically corrected by the double-pass system while the astigmatism was corrected with an external cylindrical lens to achieve the best possible retinal image. The external lens was not placed exactly in the perpendicular direction to the optical axis of the OQAS but it was slightly tilted to avoid possible reflections on the lens influencing the measurements.
Statistical analysis
The data were analysed using the SPSS software for Windows (V.17.0). Comparisons were considered to be statistically significant for p values of less than 0.05.
An analysis of variance test was used with a Bonferroni post-hoc statistical analysis to compare the mean values of the main outcome measures for eyes of the control group and with nuclear, cortical and posterior subcapsular cataracts of different grades (LOCS III). The pair of eyes was included as a factor to control for the inter-eye correlation. A post-hoc power analysis was also performed (α=0.05) to show the statistical significance of the results obtained.
Agreement between the BSCVA and the OSI was analysed using a non-linear regression model, from which the multiple correlation coefficient was computed (r).
Results
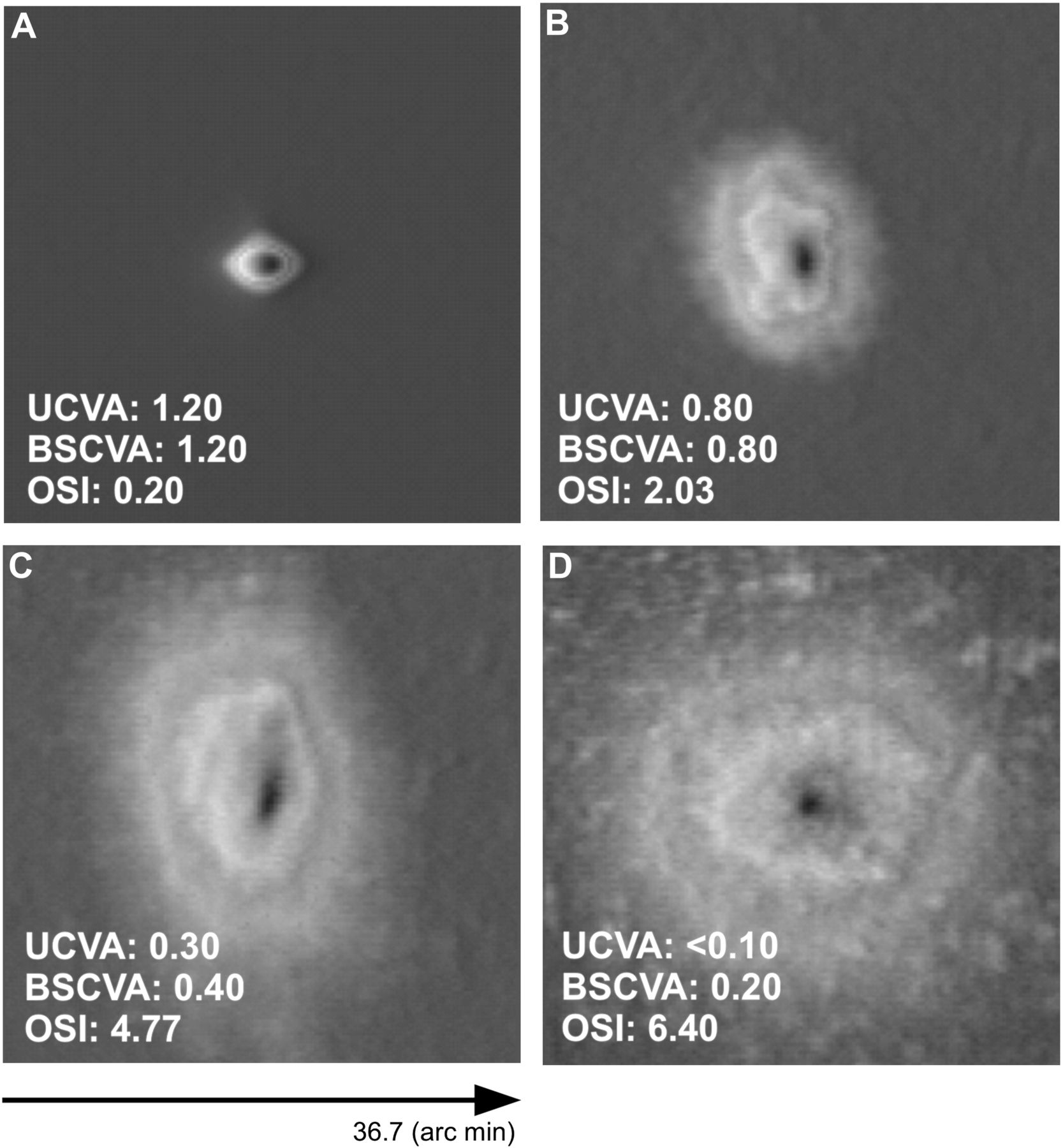
Figure 1 shows double-pass images associated with representative cases of patients belonging to the control group and with nuclear opacities. Table 1 presents the patient demographics and the number of eyes. No statistically significant intra-patient correlations could be established and for this reason the two eyes were considered when the patient had cataracts in both eyes.
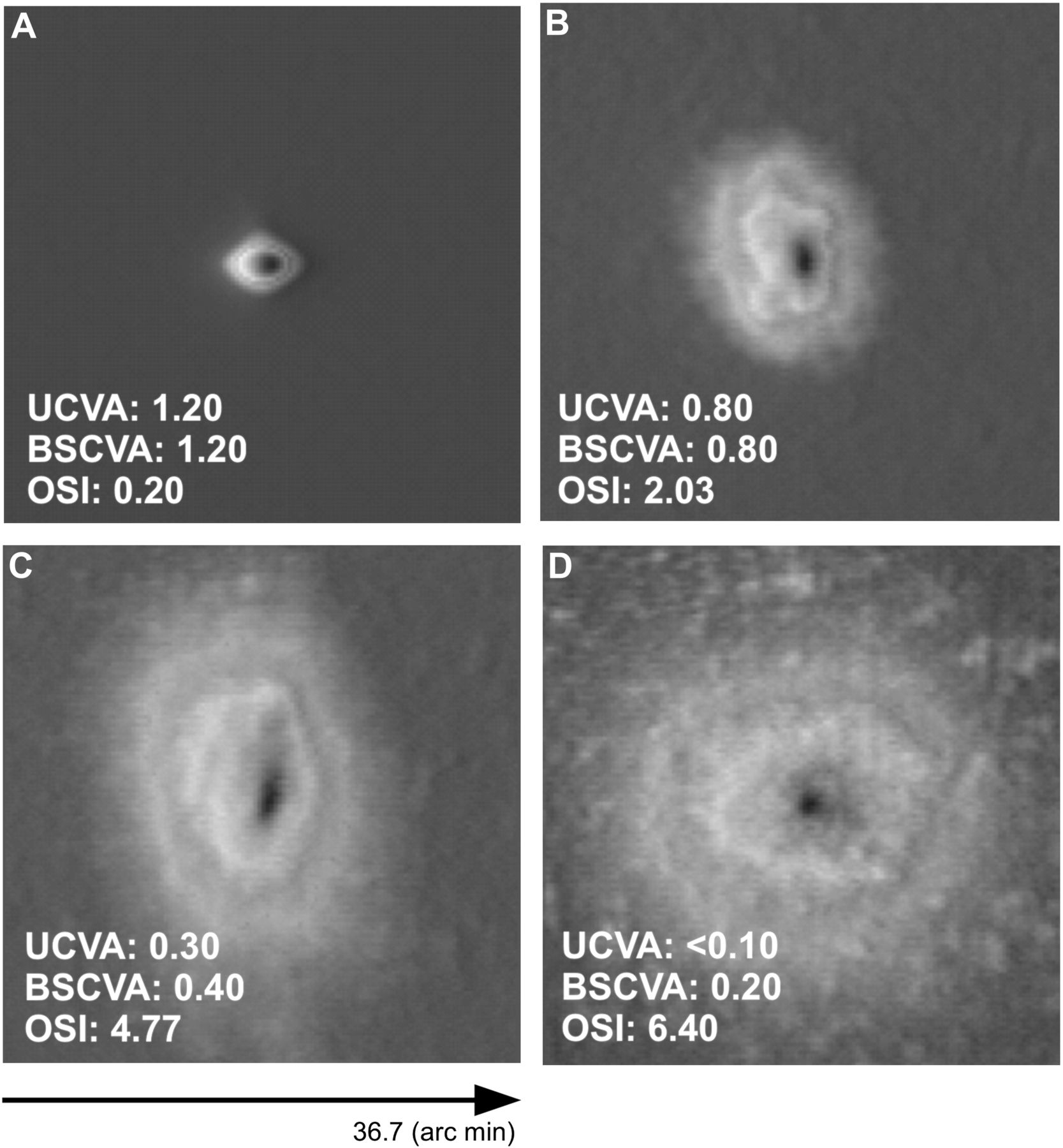
Double-pass images corresponding to representative eyes without cataract (control group) (A), with a nuclear cataract classified as NO1 (B), as NO2 (C) and as NO3 (D). The decimal best spectacle-corrected visual acuity (BSCVA) and objective scatter index (OSI) are also shown. UCVA, uncorrected visual acuity.
Patient demographics for the eyes of the control and cataract groups classified using the LOCS III
Table 2 shows the refraction of eyes considered. No statistically significant differences were found between eyes in the control group and with nuclear, cortical and posterior subcapsular cataracts in terms of sphere, cylinder and spherical equivalent (p>0.05).
Subjective refraction (sphere, cylinder and SE) of the control and cataract groups
Considering each type of cataract independently, no significant differences were observed in the refractive error between eyes belonging to different gradations (p>0.05). No statistically significant differences were found between the refraction and the OSI (p>0.05).
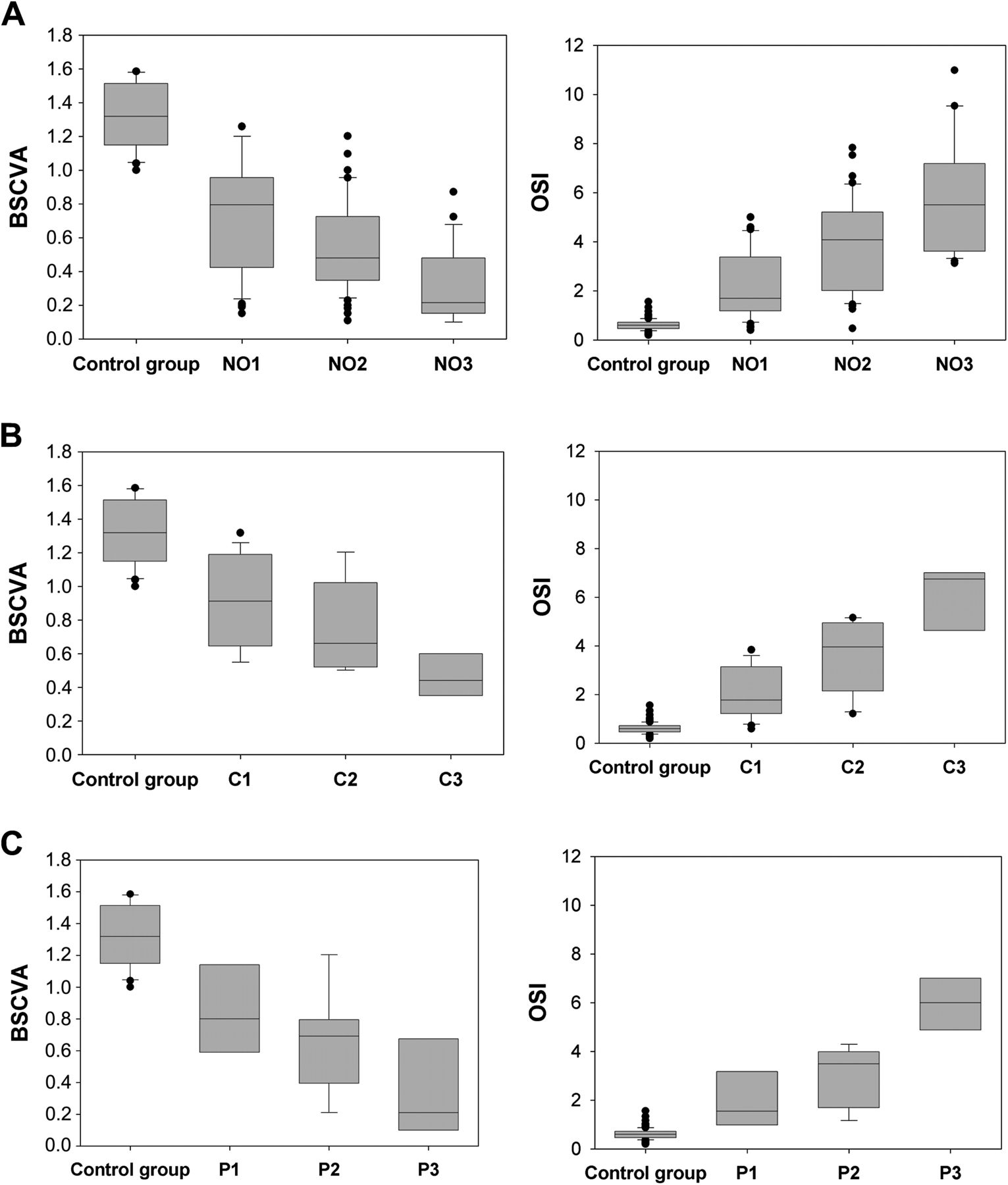
In table 3 the mean BSCVA and OSI of eyes in the control and cataract groups are shown. Figure 2 uses box plots to compare the BSCVA and OSI among groups. For all types of cataracts, the BSCVA values worsened as the cataract grade increased. An increase in the OSI was observed with cataract gradation. However, there was a significant dispersion in both parameters, especially in groups with cortical and posterior subcapsular cataracts.
BSCVA and OSI of the control and cataract groups

Box plots showing the decimal best spectacle-corrected visual acuity (BSCVA) and objective scatter index (OSI) values for the control group and eyes with nuclear cataracts graded as NO1, NO2 and NO3 (A), cortical cataracts graded as C1, C2 and C3 (B), and posterior subcapsular cataracts graded as P1, P2 and P3 (C). Five statistical descriptors are shown in these plots: maximum, third quartile, median, first quartile and minimum as well as the outliers.
The comparison of the mean OSI reported no statistically significant differences between eyes with different cataract types (p>0.05). Statistically significant differences were found in the BSCVA when eyes with cortical and nuclear cataracts (p<0.001) and those with cortical and posterior subcapsular cataracts (p=0.048) were compared. This was not the case in eyes with nuclear and posterior subcapsular cataracts (p=0.603).
The mean BSCVA and OSI of the three groups with different gradation were compared for each type of cataract independently. Statistically significant differences (p<0.05) were found in terms of the BSCVA and OSI between groups with different LOCS III and with the control group, regardless of the type of cataract. The only exceptions were found when the BSCVA of cortical cataracts graded as C1 and C2 (p=0.084) and C2 and C3 (p=0.131) was considered, and when groups P1 and P2 were compared in terms of BSCVA (p=0.793) and OSI (p=0.070).
A post-hoc power analysis on our outcomes revealed that the power for all significant results was above 0.98 so that the sample size used could be considered adequate.
Figure 3 shows the values of OSI in all eyes. While eyes of the control group always had small OSI, eyes with cataracts were linked to higher values. There was a high variability in the results, and some individual eyes with cataracts classified in different groups using the LOCS III showed similar OSI.
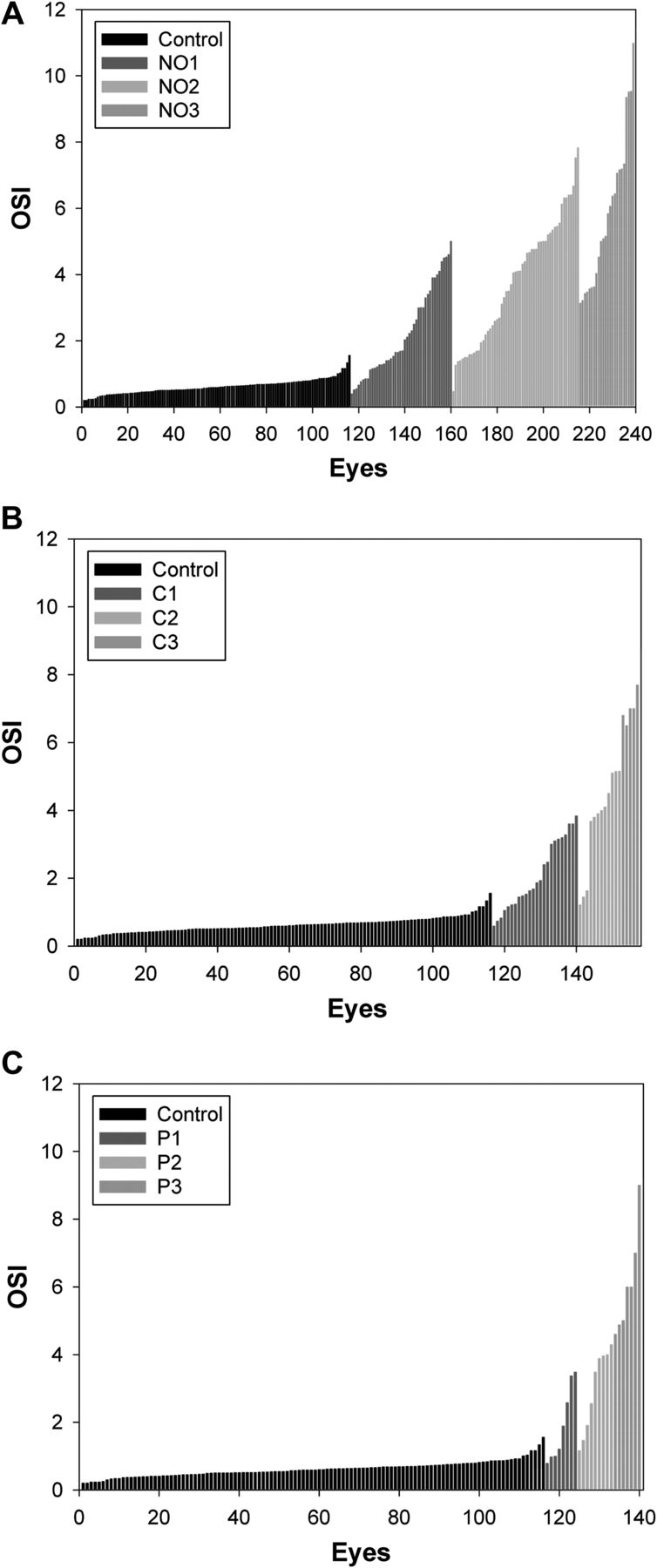
Individual objective scatter index (OSI) values for eyes belonging to the control group and eyes with nuclear cataracts (A), cortical cataracts (B) and posterior subcapsular cataracts (C).
The analysis of the data also established a non-linear correlation between the OSI and BSCVA (figure 4). An exponential decay model with two parameters (y=a·e−bx) was found to provide the best agreement. The correlation coefficients (r) obtained for the regressions were 0.878 (nuclear), 0.843 (cortical) and 0.844 (posterior subcapsular) cataracts, thus showing that approximately 70% of the variation in OSI could be explained by the model applied.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scattergrams showing the relationship between the objective scatter index (OSI) and decimal best spectacle-corrected visual acuity (BSCVA) for eyes of the control group and with nuclear cataracts (A), cortical cataracts (B) and posterior subcapsular cataracts (C). The multiple correlation coefficient (r) and parameters (a) and (b) of the exponential decay regression model performed are also given. Solid line corresponds to the regression while dashed lines correspond to the 95% CI.
Discussion
The presence of a cataract degrades the optical quality and thus the double-pass images (figure 1). The deterioration of the retinal image is more pronounced as the cataract grade increases. The cataract has a great impact on outer parts of the image, mainly related to scattering. Examples show a decrease in the BSCVA with increasing cataract grade, while eyes with higher grades are linked to higher OSI.
Results have shown that in general nuclear, cortical and posterior subcapsular cataracts lead to a visual deterioration in terms of BSCVA and an increase in OSI. However, as seen in figure 2, this is not the case for all subjects. The BSCVA and OSI worsened as the cataract grade increased, although there was a significant dispersion in both parameters, especially in groups with cortical and posterior subcapsular cataracts. This could be explained by the fact that some patients with these cataracts still have a clear centre of the lens and that the double-pass system measured the optical quality using a pupil diameter of 4 mm. Patients with nuclear cataracts always have opacities in the centre and, therefore, a smaller dispersion is expected. In addition, visual acuity can be maintained even when some scatter effect is already measurable through OSI.
We did not find significant differences in terms of BSCVA and OSI when groups of eyes with different cataracts were compared (p>0.05). The only exception was for eyes with cortical cataracts, for which slightly better BSCVA was obtained. Probably this could again be attributed to some eyes still with a clear centre.
Statistical analysis (analysis of variance test with a Bonferroni post-hoc analysis) proved that eyes with any type of cataract could generally be differentiated from eyes without cataracts in terms of BSCVA and OSI (p<0.05).
When each type of cataract was analysed independently, significant differences were in general observed when the BSCVA and OSI values of eyes with different LOCS III were compared.
The OSI for eyes of the control group was on average lower than 1, whereas this parameter was higher when the cataract gradation increased. Artal and collaborators19 established a classification of eyes with different degrees of scattering based on the OSI. Using this scale and the LOCS III, every eye can be classified and a percentage of agreement regarding the number of eyes classified in equivalent levels by the two scales can be established. We found 72.4% of agreement in eyes with nuclear cataracts, 86.6% with cortical and 84.3% with posterior subcapsular. If only the first two levels in both scales were considered, which is especially useful in daily clinical practice to detect early cataracts, 83.1% of eyes with nuclear cataracts were classified as equivalent with both methods. The percentages were 89.3% for cortical and 91.1% for posterior subcapsular cataracts. Only six eyes in the control group (5.13%) had OSI values higher than 1 and, consequently, were classified erroneously as having an early cataract. These results are very similar to those found by Artal et al19 and suggest the suitability of using the OSI as a tool for detecting incipient cataracts. Furthermore, it must be remarked that three physicians participated in this study. Authors have analysed the reliability of the LOCS III test when different observers were involved and found that results may show variability.7 Percentages of agreement could be even more favourable if only one physician had participated.
A deeper analysis of the data also established a significant non-linear correlation between OSI and BSCVA (figure 4). The plots show that in some cases a dense cataract can drastically increase the OSI and therefore the intraocular scattering, whereas its impact on visual acuity is not as strong. This effect is more pronounced in eyes with cortical cataracts, whose OSI values are comparable to those obtained for nuclear and posterior subcapsular cataracts, although their BSCVA remains higher.
Ortiz et al24 also found a significant decrease in the modulation transfer function measured with a double-pass system with increasing cataract grade. However, measurements performed with a wavefront sensor did not report noteworthy differences in higher-order aberrations, which confirms that double-pass retinal images can be used to measure the joint effect of higher-order aberrations and scattering. The results obtained in this study suggest that OSI correctly isolates the information related to intraocular scattering from the double-pass images and thus from the corresponding modulation transfer function.
Another study has analysed the visual and optical performance in patients with different intraocular lenses after cataract surgery.25 Meanwhile visual acuity and contrast sensitivity seemed not to be enough to describe the visual outcomes, optical quality measured with a double-pass system revealed significant differences among groups. This, together with our results, highlights the relevance of pre and postoperative optical quality evaluation in cataract patients.
In conclusion, the OSI is a new parameter that can be used as a valuable tool for evaluating intraocular scattering and grading cataracts. The main advantage of using double-pass measurements is that it is an objective procedure that does not require the active participation of the patient or the physician. The OSI measurement provides a useful tool for detecting incipient cataracts and might be useful for evaluating the convenience of scheduling the surgery.
References
Footnotes
Funding This study was supported by the Spanish Ministry of Education and Science under grant DPI2008-06455-C02-01, and the Spanish Agency for International Cooperation under grant D/030286/10.
Competing interests MA is an investor for Visiometrics SL. JLG, PA and JP are investors and consultants for Visiometrics SL. MV, MJR, SOL, JCO and AS have no interests to declare.
Patient consent Obtained.
Ethics approval Ethics approval was provided by Comité Ético del IMO, Comité Ètic de l'Hospital Universitari Mútua de Terrassa.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance
- At a glance