Article Text

Abstract
Purpose To report outcomes and complications of fine-needle aspiration biopsy (FNAB) of uveal melanoma performed for diagnostic and prognostic purposes.
Methods Prospective interventional case series of 150 consecutive patients with a clinical diagnosis of uveal melanoma. The FNAB approach (transcorneal (TCO), transscleral (TSC) and transvitreal (TVT) was primarily determined by the location of the tumour. The FNAB was performed using a 25-gauge needle using a previously published technique. Prognostication was done using fluorescent in situ hybridisation detection of monosomy of chromosome 3.
Results FNAB was obtained via TCO (8), TSC (71) and TVT (64) approach and impression smear in seven cases. Diagnostic yield was 92%. False-negative results were observed in 8%. Diagnostic yield was significantly correlated to biopsy approach (TCO 100%, TSC 96%, TSV 86%; p=0.029) and tumour size (basal diameter >5.0 mm; height >2.5 mm). Persistent haemorrhage (subretinal haemorrhage or vitreous) requiring surgical intervention (1%) and rhegmatogenous retinal detachment (1%) were rare. Endophthalmitis, hypotony, tumour recurrence, episcleral seeding were not observed over the average follow-up of 37 months. Prognostication could be performed in 85% of cases. Overall, only 47% of eligible patients enrolled into the adjuvant therapy trial.
Conclusions FNAB for uveal melanoma with 25-gauge needle is a safe procedure that can yield diagnostic and prognostic information in vast majority of cases (92% and 85%, respectively). Even so, only about half of the eligible cases eventually enrolled into the adjuvant therapy trial. Possibility of negative FNAB yield should be considered when counselling patients with small tumours. Alternative means of diagnostic biopsy and methods of prognostication need to be assessed for small tumours.
- Choroid
- Neoplasia
- Pathology
Statistics from Altmetric.com
Introduction
Since original descriptions of diagnostic fine-needle aspiration biopsy (FNAB) for undetermined intraocular mass by Jakobiec in 1979,1 diagnostic FNAB has become well established in various ophthalmic oncology centres.2
With the discovery of cytogenetic markers (chromosome 3 monosomy) for prognostication by Prescher in 1992,3 feasibility of FNAB of uveal melanoma was first reported by Naus et al4 in 2002 who obtained FNAB samples from enucleated globes with uveal melanoma. By 2008, Midena et al5 reported a 3-year follow-up on the excellent safety profile of prognostic FNAB performed in vivo in posterior uveal melanomas undergoing plaque brachytherapy. Since then, safety of prognostic FNAB for uveal melanoma has been reported.6–8
Prognostic FNAB of uveal melanoma is now routinely recommended for individualised prognostication.6 ,7 ,9 The purpose of such prognostication is not limited to patient awareness; it is also to provide customised systemic surveillance for detection of subclinical metastases and potentially to enrol patients with risk of metastases into adjuvant therapy trials.10
Herein we report outcomes of a prospective study conducted to determine diagnostic and prognostic yield, visual outcome and complications of FNAB performed in 150 patients with a clinical diagnosis of uveal melanoma with explicit purpose to enrol at-risk patients into a parallel and companion adjuvant therapy trial (ClinicalTrials.gov Identifier: NCT01100528).11
Methods
Study design and enrolment
We conducted a prospective study to determine diagnostic yield, prognostic yield, visual outcome and ophthalmic complication rates of FNAB for uveal melanoma. In this consecutive, interventional prospective study of 150 patients with a clinical diagnosis of uveal melanoma, patients who accepted to undergo prognostication with explicit purpose to then consider enrolment in a parallel and companion adjuvant therapy trial (ClinicalTrials.gov Identifier: NCT01100528) were included.
All patients were informed about the investigational nature of the study and provided written informed consent. Exclusion criteria were age less than 18 years, prior therapy of the primary tumour and evidence of metastasis assessed at baseline by contrast-enhanced CT scan of chest, abdomen and pelvis. Therapy of the primary tumour included plaque radiotherapy, enucleation or tumour resection based on the standard of care guidelines. IRB approval was obtained (Local IRB #: CASE 5608-CC666).
Ophthalmic examinations and follow-up
In addition to detailed history, ophthalmic examination was performed using slit-lamp examination, 90D lens, gonioscopy and indirect ophthalmoscopy (where indicated). Ancillary studies including indocyanine angiography and ultrasonography with B scan and standardised A scan were performed based on clinical examination. The tumour largest basal diameter and height were measured using ophthalmoscopy and B/A scan ultrasonography. The location of the tumour was classified as iris (including iridociliary), ciliary (including ciliochoroidal) or choroidal. The distance from the fovea and disc was measured based on ophthalmoscopic assessment (where feasible) and approximated to the nearest half millimetre.
Patients were evaluated at their first postoperative visit within 1–4 weeks followed by every 3 months in the first year and every 6 months thereafter. Additional examinations were scheduled as determined by clinical findings or patient symptoms.
Visual outcome at 3 months, persistent visually significant haemorrhage (subretinal or vitreous) requiring surgical intervention (by 4 weeks), rhegmatogenous retinal detachment, endophthalmitis, hypotony, tumour recurrence and evidence of episcleral seeding at the needle entry site were recorded at every visit.
FNAB technique
The FNAB approach (transcorneal (TCO), transscleral (TSC) and transvitreal (TVT)) was primarily determined by the location of the tumour. FNAB was performed using a 25-gauge needle using previously published technique.2 For TCO biopsy, a 1 mm incision was created at the limbus and viscoelastic material was injected over the biopsy site. TSC FNAB was performed for ciliochoroidal and anterior choroidal tumours just prior to placement of radiation implant under a partial thickness (80% scleral thickness) equilateral triangular scleral flap. One or two passes were made and aspirated material from each pass flushed into a single Cytolyt tube. For choroidal tumours located posterior to the equator, tumour localisation and TVT FNAB with a 25-gauge needle was done under indirect ophthalmoscopic control. Without letting the plunger reset to its original position, the needle was withdrawn along the path of insertion. Only a single pass was made through the tumour sample. Localised subretinal and/or vitreous haemorrhage was controlled by applying pressure to the globe by a cotton-tipped applicator at the entry site or by injecting balanced salt solution into the vitreous cavity.2 All enucleated globes were subjected to TSC FNAB after the globe had been enucleated.
FNAB sample processing
All aspirated material was flushed into Cytolyt solution for ThinPrep processing (Hologic, Marlborough, Massachusetts, USA).12 The sample in Cytolyt was then subjected to one or more centrifugation and concentration steps. The pellet was resuspended in a cell preservative solution, PreservCyt, for automated processing. The ThinPrep processor mixes the sample and then, using a gentle vacuum, collects cells on a filter in an evenly dispersed way, approaching a monolayer. This filter was then inverted and its cellular contents transferred to a microscope slide. This method optimises cell yield and preservation and standardises slide preparation for interpretation in this setting of limited material.
Cytological assessment
The diagnosis of uveal melanoma was based on characteristic cellular features as assessed by one of the authors (CVB).13 Uveal melanoma typically have a relatively bland cellular appearance due to the prevalence of spindle cells often associated with an epithelioid component creating a mixed pattern in most cases.13 Cytoplasmic melanin is also a consistent feature.13 The cytological reporting for the slides was divided into four conventional categories: (1) unsatisfactory for interpretation, (2) negative for melanoma, (3) atypical cells (not diagnostic or consistent with melanoma) and (4) positive for melanoma. Where available, FNAB diagnosis of uveal melanoma was corroborated with histopathological diagnosis.
Fluorescent in situ hybridisation
If the sample was diagnostic of melanoma and there were sufficient cellularity, chromosome 3 status was assessed by fluorescent in situ hybridisation (FISH) using both directly labelled SpectrumGreen and SpectrumOrange enumeration probes for the alphacentromeric locus of chromosome 3 (CEP3) and a locus-specific probe, 3p26 (TelVysion 3p, Abbott Molecular Vysis, Des Plaines, Illinois, USA).14 Probes were hybridised to ThinPrep slides. A total of 200 interphase cells were scored using a Zeiss FISH workstation to determine the percentage of signals for each locus. Based on many prior studies, we chose to use a cut-off value of 20% to define monosomy for chromosome 3.15
Statistical analysis
Data were analysed using STATA V.11. Tumour height, basal diameter, distance from fovea and optic disc were coded as categorical variables. Unsuccessful prognosis or diagnosis events were rare in the relatively small data set, and so traditional logistic regression was eschewed in favour of exact logistic regression. Univariate ORs were estimated; multivariate risk factors could not be estimated due to small sample size and high correlation among the variables. Exact p values are reported.
To test associations between categorical variables, Fisher's exact test was used. For hypothesis testing relating to continuous outcomes, equal variance assumptions were made based on examination of boxplots. Associations between continuous variables and two categories, equal variance was not assumed, and so Welch's t test was used. Associations between continuous variables and multiple categories were tested by analysis of variance. In those multiple categories, significant differences in means were assessed using Tukey's correction for multiple comparison of means.
Results
A total of 150 samples from 150 patients were obtained. Iris and iridociliary tumours that were resected (seven cases) did not undergo FNAB as they were diagnosed and prognosticated by impression smear or FISH on paraffin-embedded tissue so as to maintain the integrity of tumour margins for histopathological assessment. These seven cases were excluded from further analysis in this report (table 1). Although the majority of the tumours were choroidal in location (105, 75%), iris and ciliary body melanoma were also included completing the spectrum of uveal melanoma. Most of the tumours were treated by plaque radiation therapy (102, 72%) following standard clinical guidelines. All enucleated globes (41, 27%) were subjected to TSC FNAB after the globe had been enucleated and therefore included in the analysis. The average follow-up in this study was almost 2 years.
FNAB of uveal melanoma: profile of study patients (n=150)
TCO (5%), TSC (50%) and TVT (45%) approaches for FNAB were used depending on the tumour location; however, the needle size (25 gauge) and handling and processing of the aspirated sample were as per a standardised protocol.12
Diagnostic yield
Positive samples were defined as those with sufficient cellularity to ascertain a cytological diagnosis of uveal melanoma. Of the143 samples, 131 positive samples were obtained (92% true positive) (table 2). Of the 131 positive samples, 122 samples (86%) were positive for melanoma and in 9 samples (5%) atypical cells consistent with melanoma were observed. Twelve samples (9%) were reported as being negative for melanoma. Ten samples contained non-diagnostic atypical cells and two lacked even atypical cells; one contained benign squamous cells and columnar cells suggestive of conjunctival contamination while the second contained rare histiocytes. Non-melanoma benign or malignant tumours were not diagnosed (table 2). There was 100% correlation between cytological and histological diagnosis on all 41 enucleated eyes.
Fine-needle aspiration biopsy of uveal melanoma
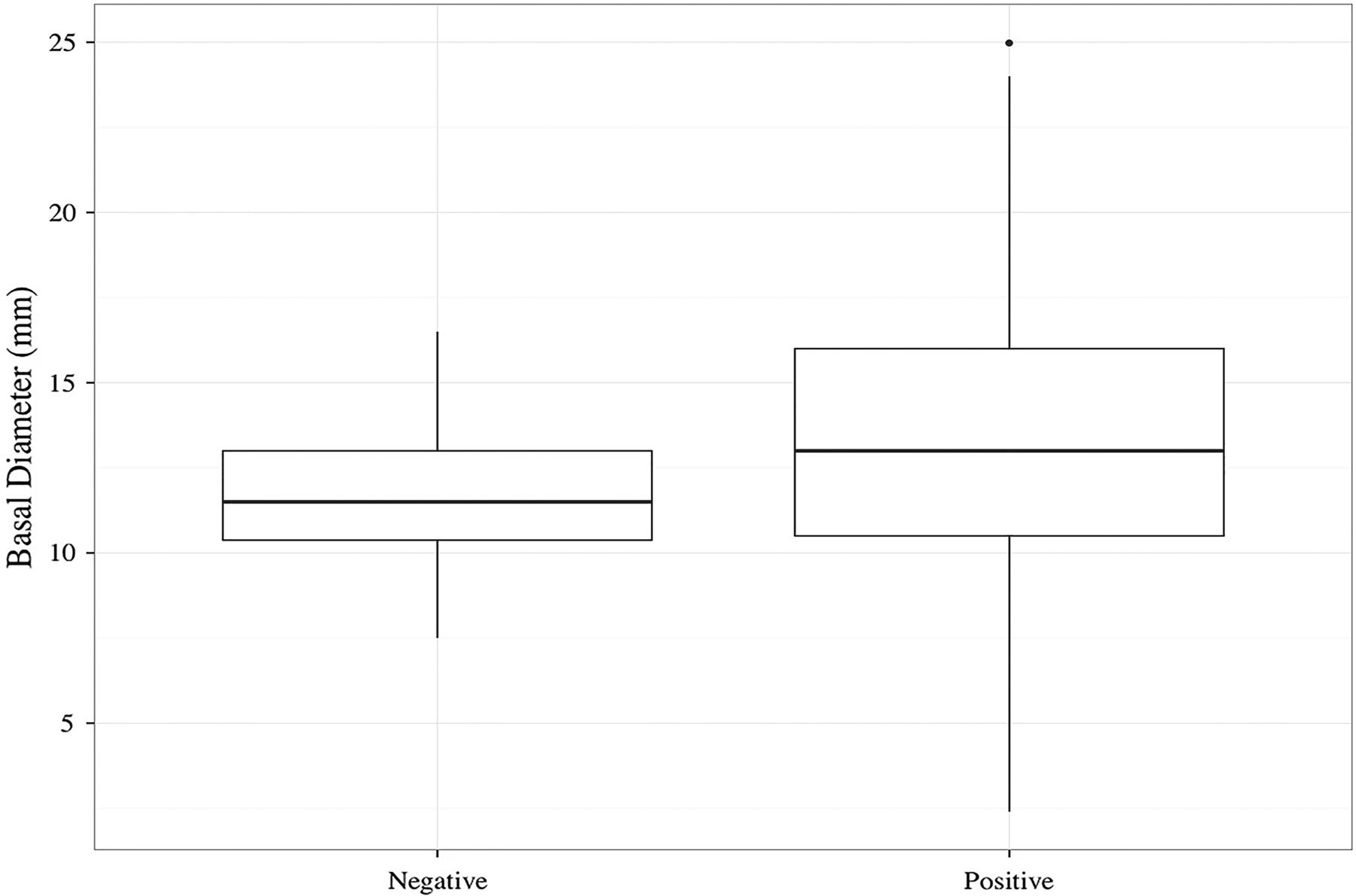
As all the biopsied tumours had typical clinical, ultrasonographic and angiographic features of uveal melanoma (inclusion criteria), based on the sample composition and final reporting, a false-negative rate of 9% was calculated. Sample positivity varied significantly (p=0.029) by FNAB approach (100% TCO, 97% TSC and 84% TVT) (table 3). A statistically significant correlation between tumour height and a positive biopsy was also observed. Average tumour height was 6.2 mm for positive samples and 3.3 mm for negative samples (p=0.0001) (figure 1). The largest basal diameter was also correlated to positive biopsy but less so than tumour height. The average basal dimension was 13.4 mm in the positive group compared to 11.6 mm in the inadequate group (p=0.039) with overlap in the tumour basal diameter between the two groups (figure 2).
Fine-needle aspiration biopsy of uveal melanoma: comparison of positive and negative diagnostic samples (n=143)
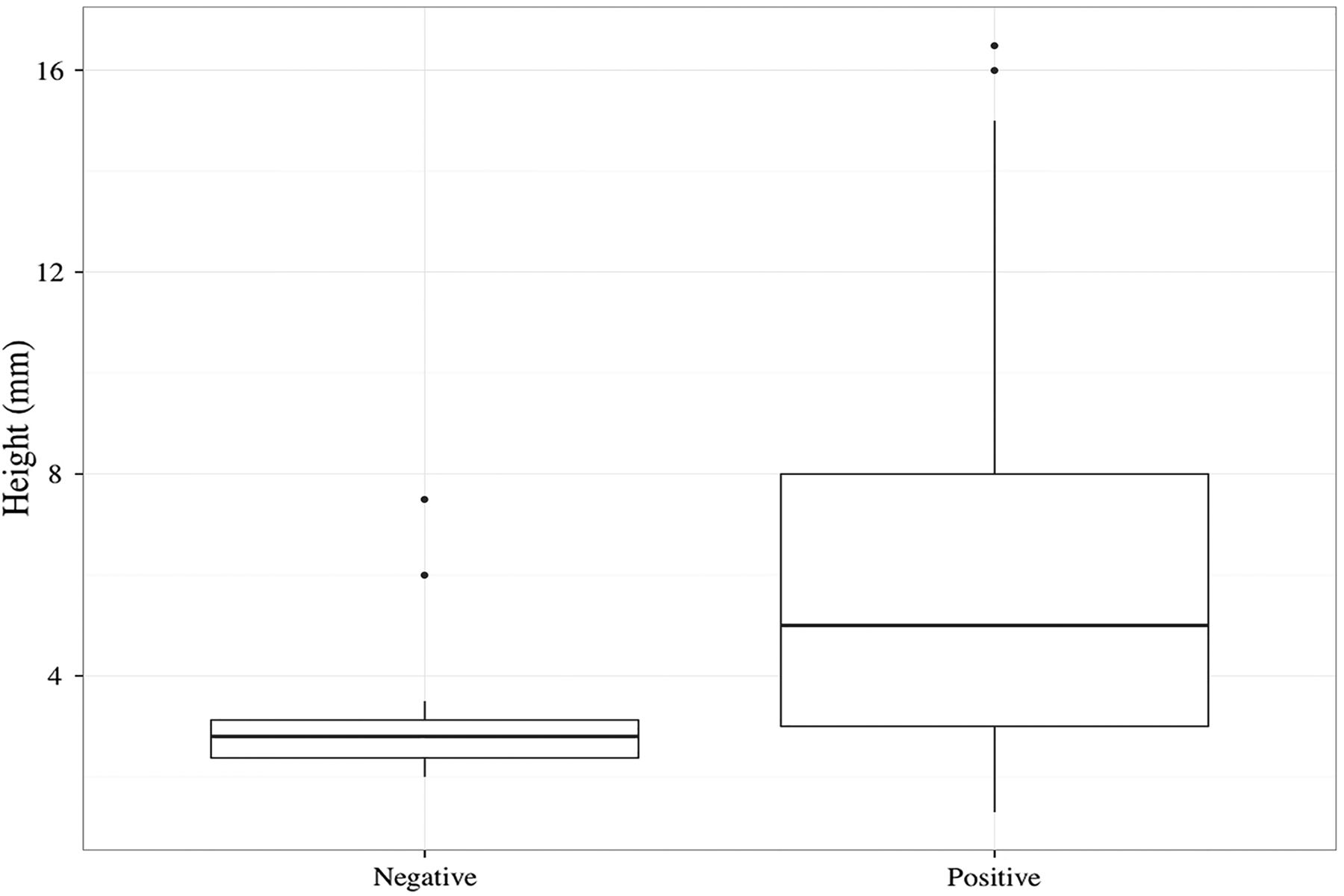
Boxplot (box and whisker plot) of tumour height (mm) grouped by positivity/negativity of sample for diagnostic cytology. The whiskers correspond to the first and fourth quartiles of tumour height, the box corresponds to the second and third quartiles and the bold line corresponds to the median. The difference in mean height between the two groups is statistically significantly (p value≤0.01) by Welch's two sample t test, which does not assume equal variances. There is little overlap in the distributions of tumour height between the two groups, with negative tumour samples generally coming from thinner tumours. Two outliers in the negative group had tumour thickness of 6.0 and 7.5 mm, were biopsied by transscleral (TSC) and transvitreal (TVT) techniques and reported as unsatisfactory and atypical cells not diagnostic, respectively.
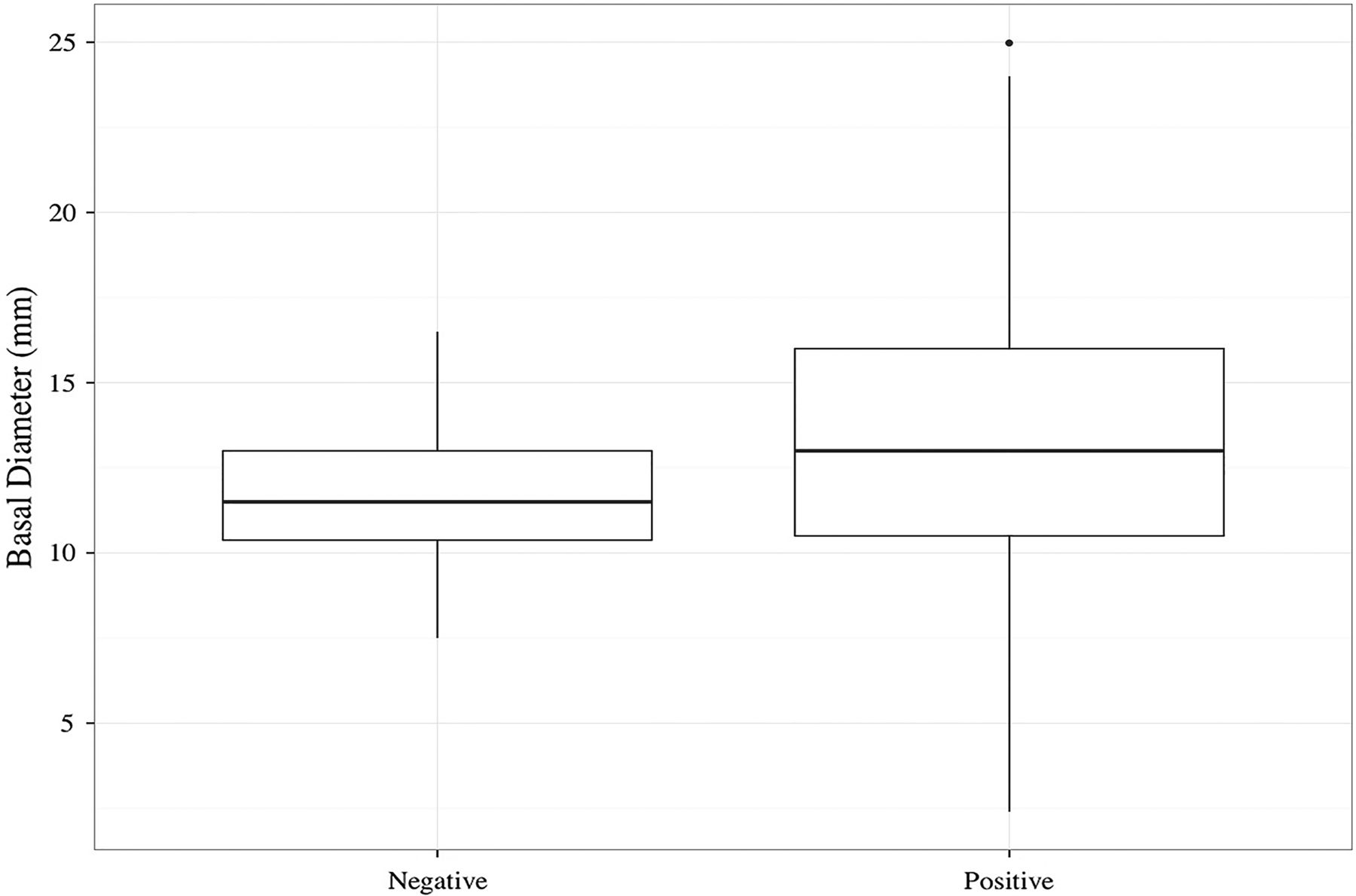
Boxplot of tumour largest basal diameter, grouped by positivity/negativity of sample for diagnostic cytology. The difference in mean height between the two groups is statistically different (p value=0.0391) by Welch's two sample t test, which does not assume equal variance. There is overlap in the tumour basal diameter between the two groups, even though the statistical test found the two means to be marginally statistically different.
Prognostic yield
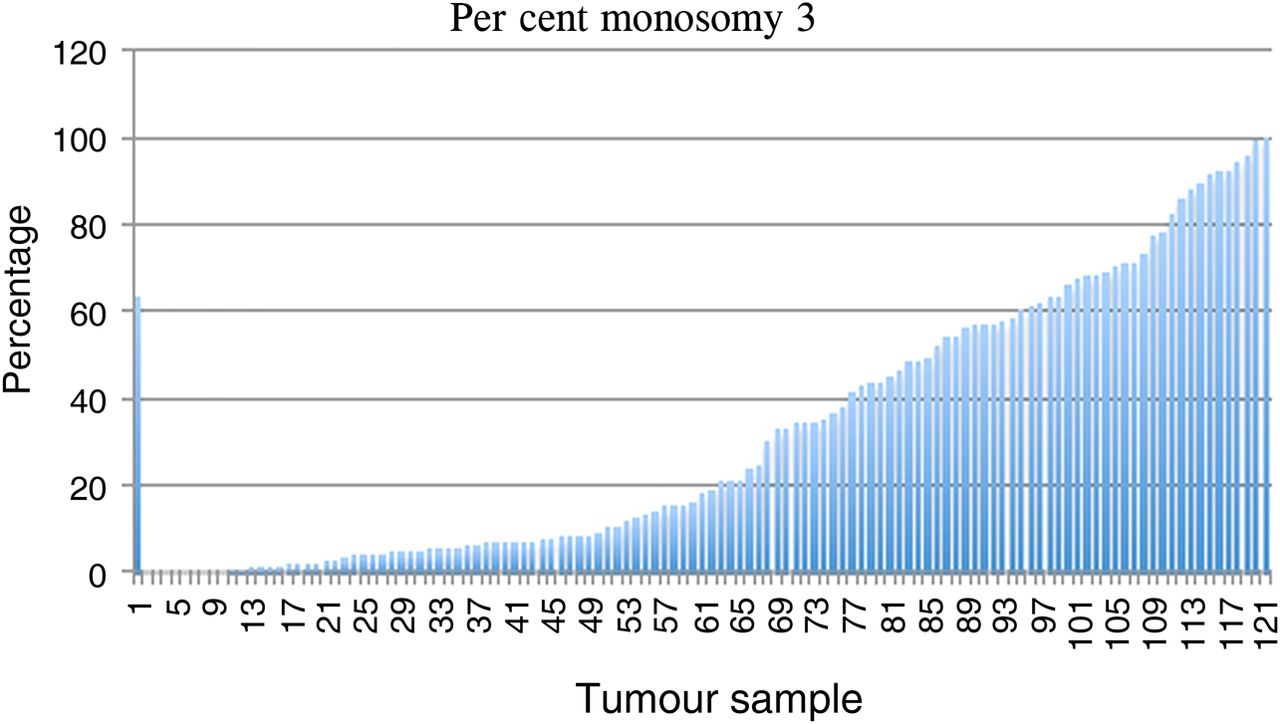
Prognostication using FISH technique (figure 3)15 ,16 could be performed only on 121 samples because of lack of adequate cellularity (less than 200 cells) in the remaining 22 samples, giving overall prognostication yield of 84.6% (table 4). Univariate analysis for factors influencing prognostication yield (n=141) revealed method of treatment (enucleation), tumour size (>5.0 mm in the largest basal diameter; height >2.5 mm) and location (>3.0 m from fovea) to be statistically significant (p<0.05) (table 5). Percentage monosomy 3 within a tumour ranged from 0% to 100% (figure 4).
Fine-needle aspiration biopsy of uveal melanoma: prognostication yield (n=121)
Fine-needle aspiration biopsy of uveal melanoma: univariate analysis for factors influencing prognostication yield (n=143)

Fluorescence in situ hybridisation using directly labelled fluorescent probes to the alphacentromeric region of chromosome 3 (CEP3) (SpectrumOrange) with 4′,6-diamidino-2-phenylindole counterstain illustrating eusomy (disomy) of chromosome 3 (A, two orange signals) and monosomy (B, one orange signal).
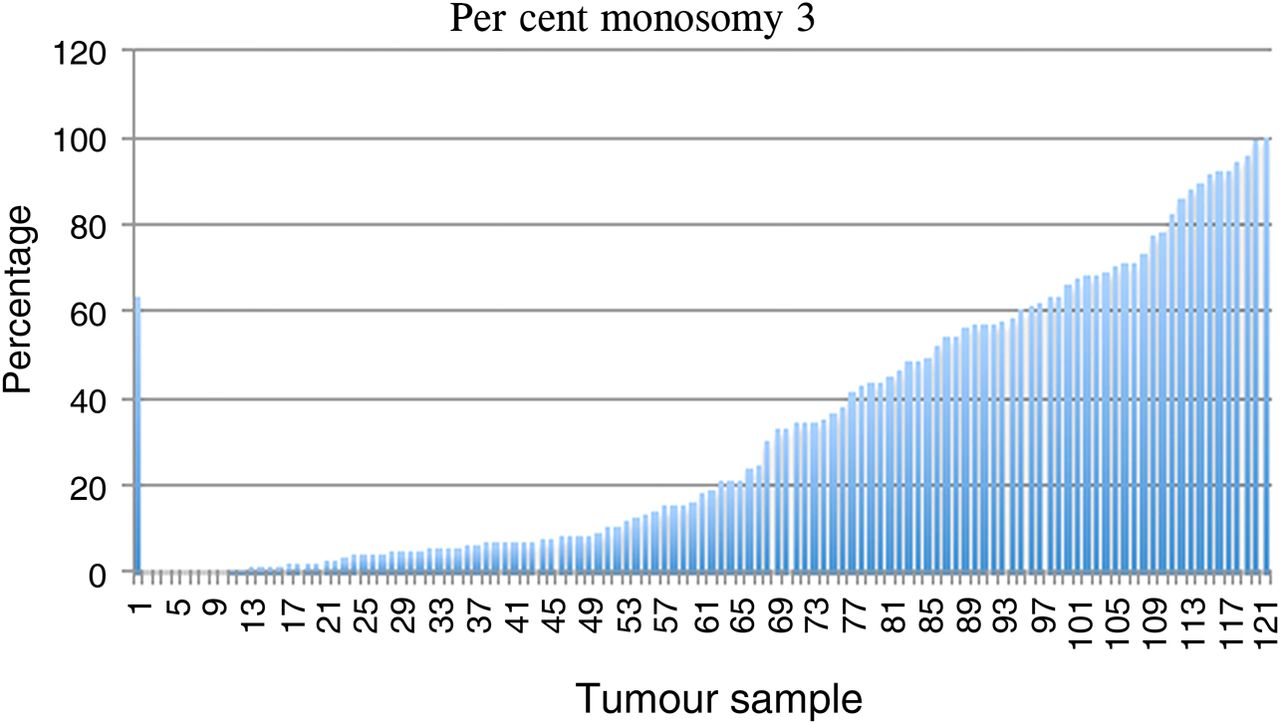
Frequency distribution of the percentage of cells demonstrating monosomy 3. Each vertical bar represents a single case (n=121).
Complications
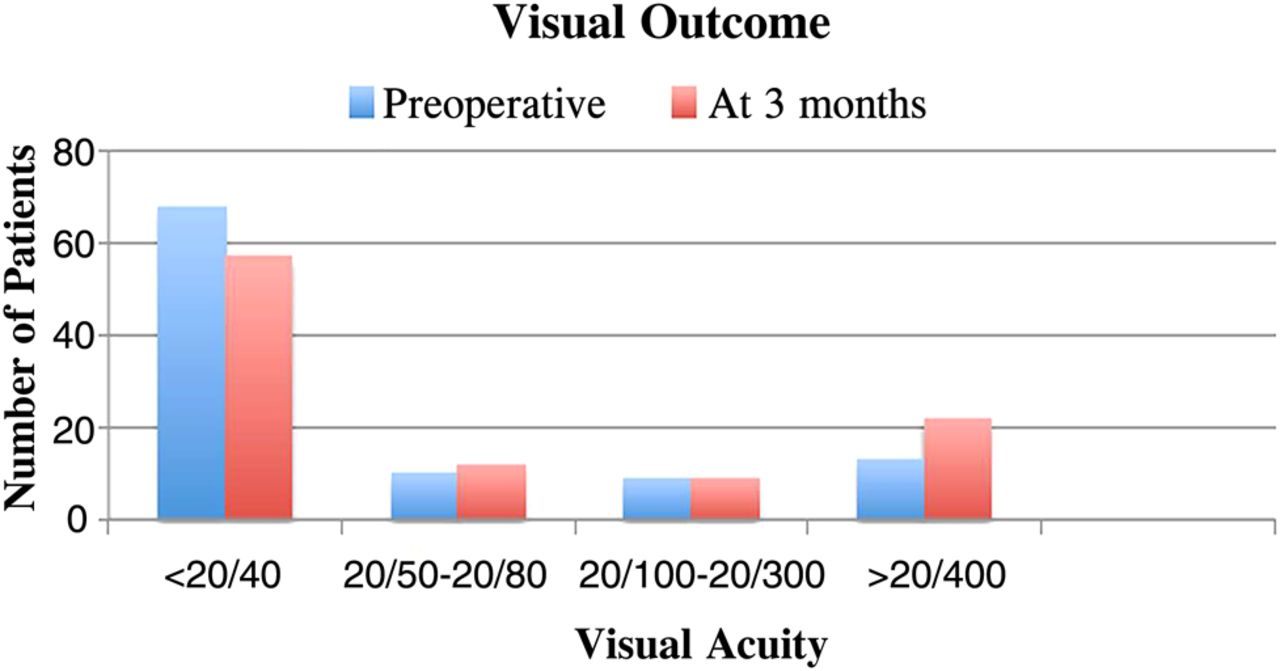
FNAB-related complications were assessed only for 102 eyes that did not undergo enucleation(41). Two patients had follow-up of less than 3 months. In the remaining 100 patients, visual acuity at 3 months of ≤20/40 and ≥20/400 was recorded in 57% and 22% patients, respectively. The proportion of patients with visual acuity ≤20/40 and ≥20/400 when compared between baseline and at 3 months decreased by 11% and increased by 9% at 3 months (figure 5). Minor vitreous or subretinal haemorrhage that resolved spontaneously within 4–6 weeks was universally observed (figure 6). However, visually significant complications such as persistent haemorrhage (subretinal haemorrhage or vitreous) requiring surgical intervention (1%) and rhegmatogenous retinal detachment (1%) were rare.

Visual outcome following fine-needle aspiration biopsy (FNAB). Note worsening of visual acuity at preoperative visit and at 3 months following plaque radiation therapy and FNAB.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Typical localised preretinal haemorrhage at the fine-needle aspiration biopsy (FNAB) site present at the first postoperative visit (1 week) (A). Such haemorrhage is not visually significant and underwent total spontaneous resolution within 6 weeks (B).
A 60-year-old man was referred with a medium-sized choroidal melanoma in the inferior temporal quadrant (9.5×8.5×3.5 mm) of the left eye. Following plaque application the tumour showed minimal regression to the height of 3.2 mm. TVT biopsy had revealed absence of chromosome 3 monosomy and confirmed melanoma on cytological assessment. After 12 months the vision suddenly dropped from 20/40 to Counting Fingers due to vitreous haemorrhage. Two horseshoe retinal tears were noted, one along the posterior margin of the tumour and one superior to it. He underwent scleral buckle, pars plana vitrectomy, endolaser, C3F8 injection and phacoemulsification with insertion of posterior chamber intraocular lens. At 27-month follow-up, visual acuity was 20/50 attributed to mild radiation retinopathy, stable regressed melanoma without detectable metastasis on hepatic ultrasonography.
A 63-year-old woman was referred with a small choroidal melanoma (documented growth) in the supero-temporal quadrant (7.0×7.0×2.5 mm) of the left eye. Immediately following TVT biopsy, she developed diffuse vitreous haemorrhage (without retinal detachment) that did not clear over the next 4 weeks. FNAB had confirmed diagnosis of melanoma with presence of chromosome 3 monosomy. Patient entered adjuvant therapy trial completing it without complications. She underwent pars plana vitrectomy and phacoemulsification with insertion of posterior chamber intraocular lens. At 48-month follow-up, visual acuity was 20/20 with regressed melanoma (1.3 mm) without detectable metastasis on hepatic ultrasonography.
Endophthalmitis, hypotony, tumour recurrence or episcleral seeding at the needle entry site were not observed in any case over mean follow-up of 37 months (range 1–67 months).
Enrolment into adjuvant therapy trial
Of the 121 patients in whom prognostication status could be determined, 61 (50%) were ineligible as their tumour composition was below the threshold for entry into the adjuvant therapy trial (chromosome 3 monosomy <20%). Additionally, 29 (24%) patients, even after detailed counselling, elected not to enrol into the adjuvant therapy trial (table 6).
Prognostication status and enrolment into adjuvant therapy trial
Discussion
To our knowledge, this study is the first prospective study analysing outcomes and complications of FNAB performed for clinically diagnosed uveal melanoma with intent for prognostication with simultaneous cytological confirmation of the clinical diagnosis.
Cytological confirmation was deemed necessary as this study was conducted to identify eligible patients for enrolment into a parallel companion adjuvant therapy trial (ClinicalTrials.gov Identifier: NCT01100528). The study sample included a broad spectrum of uveal melanoma ranging in size from small to large, involving all uveal locations (iris, ciliary body and choroid) and treated with plaque radiation therapy, resection and enucleation following standard clinical guidelines (table 1). Iris and iridociliary tumours that were resected (seven cases) did not undergo FNAB as they were diagnosed and prognosticated by impression smear or FISH on paraffin-embedded tissue so as to maintain the integrity of tumour margins for histopathological assessment.
All FNAB were performed using a 25-gauge needle with handling and processing of the aspirated sample performed using a standardised protocol.12 However, the FNAB approach varied from TCO (5%), TSC (50%) and TVT (45%) depending on the tumour location. All enucleated globes (41, 27%) were subjected to TSC FNAB after the globe had been enucleated. Of the143 FNAB samples, we observed 92% positivity rate, similar to previous reports (table 2).17 ,18 None of the samples were reported as non-melanoma tumours with 100% correlation between cytological and histological diagnosis in all 41 enucleated eyes further corroborating high accuracy of diagnosis in a typical case of uveal melanoma.17 ,19
Negative FNAB samples either contained non-diagnostic atypical cells or lacked even atypical cells. Smaller tumours (height <2.5 mm; 5–16 mm in largest basal diameter) were more likely to be negative than larger tumours (p=0.0001) (figures 1 and 2 and table 5).
The average tumour height in the negative FNAB sample group was 3.3 mm. This is almost half (6.2 mm) of the tumour height in FNAB positive group (table 3). Except for three outliers (height was 3.5, 6 and 7.5 mm) all other negative FNAB samples were in tumours less than 2.6 mm in height (figure 1). Although greatest basal dimension was also statistically significant in differentiating positive versus negative FNAB sample, there was no clear discrimination like that observed with tumour height. Smaller tumours (less than 2.6 mm in height) are likely to yield negative diagnostic and prognostic FNAB samples. Cohen described similar results wherein FNAB adequacy was correlated with tumour height with yields of 40% in tumours <2 mm in height and of 98% in tumours over 4 mm.19 In 170 cases that were biopsied only by the TSC approach, McCannel et al also observed that FNAB adequacy was correlated with tumour height with yields of 53% in tumours <3 mm in height and of 91% in tumours over 5 mm.7 ,20
Sample positivity also varied significantly (p=0.029) by FNAB approach, being lowest for 84% TVT approach most likely due to the fact that postequatorial tumours tend to be smaller (table 3). In a smaller study of 38 patients, biopsied both by TVT and TSC approach, no significant difference was observed between the two approaches to yield sufficient material for cytopathological analysis (71%, 66%, respectively).20
Prognostication using FISH technique (figure 3)15 ,16 is a well-established methodology since the initial description of correlation between chromosome 3 monosomy by Prescher et al in 1992.3 As the technique requires scoring of 200 cells, prognostication could be performed only on 121 samples, giving overall prognostication yield of 84.6% (table 4). With commercial availability of multiplex ligation-dependent probe amplification (MLPA) test21 and gene expression profiling (GEP),22 overall prognostication positivity rate may be higher but such reports lack routine cytological confirmation. In one other study, wherein cytological assessment was correlated with GEP, cytological assessment was inadequate in almost 20% of the cases, whereas GEP was feasible in almost all cases (99.4%).8
Taken together, our data suggest that alternative means of biopsy, for example, vitrectomy-assisted tissue retrieval, might be considered for diagnostic biopsy of small tumours.23 For prognostication of such tumours, MLPA or GEP may be preferred as they both require fewer than 200 cells.21 ,22
FNAB-related complications were assessed only for 100 eyes that did not undergo enucleation (41), resection (7) or had follow-up of at least 3 months (2). Visual acuity at 3 months of ≤20/40 and ≥20/400 was recorded in 57% and 22% patients, respectively. Visual acuity worsened in 13 eyes (13%) (figure 5). Although tumour-related and radiation-related complications can also contribute to vision loss, such events are unlikely within the first 3 months following plaque radiation therapy. Visually significant complications such as persistent haemorrhage (subretinal haemorrhage or vitreous) requiring surgical intervention (1%) and rhegmatogenous retinal detachment (1%) were rare implying overall safety of this procedure in line with other published studies.5–7 ,23 A careful review of a single case each of rhegmatogenous retinal detachment and significant vitreous haemorrhage did not reveal any specific intraoperative or postoperative contributory factors. In our series, endophthalmitis, hypotony and tumour recurrence were not observed in any case. Clinical examination for needle tract seeding is limited to episcleral recurrence at the needle entry site. Exceptional occurrences of such complications has been reported.24 In a recent report of four cases with extraocular extension of uveal melanoma, three had incisional biopsy and/or vitrectomy and the fourth case did not undergo plaque radiation application at the biopsy site, a usual practice after TVT biopsy.25
As the ultimate purpose of this study was to identify patients for enrolment into the adjuvant therapy trial this aspect should be considered as an outcome measure.
Of the 121 patients in whom prognostication status could be determined, 61 (50%) patients were ineligible as their tumour composition was below the threshold for entry into the adjuvant therapy trial (chromosome 3 monosomy <20%).11 Additionally, 29 (24%) patients, even after detailed counselling elected not to enrol into the adjuvant therapy trial (table 6). A total of only 33 patients (31 from FNAB and 2 that underwent FISH on the impression smear) representing 47% of eligible patients or 22% of the total study patients (150) enrolled into the adjuvant therapy trial. With recent interest in adjuvant therapy trials, our study provides some estimates about the numbers needed to screen so as to achieve target enrolment.
In conclusion, FNAB for uveal melanoma with 25-gauge needle is a safe procedure that can yield diagnostic and prognostic information in a vast majority of cases (90% and 85%, respectively). Even so, only about half of the eligible cases may eventually enrol into an adjuvant therapy trial. The possibility of negative FNAB yield should be considered when counselling patients with small tumours. Alternative means of diagnostic biopsy and methods of prognostication need to be assessed for small tumours.
References
Footnotes
Funding Supported by FALK trust, Chicago, Illinois, USA, Ratner Foundation, New York, New York, USA, Supported in part by the Cole Eye Institute, Research to Prevent Blindness Unrestricted Grant.
Competing interests None declared.
Ethics approval IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional manuscripts are under preparation.
Linked Articles
- At a glance