Article Text

Abstract
Aim To compare astigmatic correction between femtosecond-assisted laser in situ keratomileusis (LASIK) and small-incision lenticule extraction (SMILE).
Methods A total of 111 patients were included in this prospective study. Fifty-seven eyes were treated with LASIK and 54 eyes were treated with SMILE for myopia with low to moderate (−0.25 to −4.0 D) astigmatism. Uncorrected distance visual acuity (UDVA), corrected distance visual acuity and manifest refraction were measured preoperatively and at 1 and 3 months postoperatively. Visual and refractive outcomes were reported. Changes in refractive astigmatism were evaluated using vector analysis.
Results Preoperative characteristics were similar between both groups. The UDVA at 1 and 3 months was better in the LASIK group compared with the SMILE group (p<0.009). Postoperative cylinder was higher in the SMILE group (p<0.001). Fewer eyes attained the attempted cylindrical correction in the SMILE group (p<0.029). Vector analysis showed no significant difference in target-induced astigmatism (p=0.091) and angle of error (p>0.596) between the two groups. Surgically induced astigmatism was significantly lower in the SMILE group (p<0.023), while the difference vector (p<0.001) and absolute angle of error (p<0.016) were significantly higher in the SMILE group. No significant difference was found in these parameters between 1 and 3 months in both groups (p>0.122).
Conclusions Our results showed that SMILE offered a less favourable astigmatic correction comparable to femtosecond-assisted LASIK in eyes with low to moderate myopic astigmatism. The alignment of treatment was more variable in SMILE, leading to a lower efficacy compared with LASIK by 3 months postoperatively.
- Treatment Lasers
Statistics from Altmetric.com
Introduction
Laser in situ keratomileusis (LASIK) is the most commonly performed corneal refractive surgery mainly due to a rapid visual recovery and superior safety and efficacy profiles.1 Femtosecond laser corneal flap creation has rapidly gained popularity as it allows the creation of thin and uniform flaps with great precision.2 The American Academy of Ophthalmology Technology assessment report also commented that femtosecond laser was as good as or better than microkeratome for creating LASIK flap.3 The use of femtosecond laser has recently been extended to a new form of corneal refractive procedure, which fashions an intrastromal lenticule with or without flap creation, termed refractive lenticule extraction. Small-incision lenticule extraction (SMILE) represents a more recent advancement in refractive surgery in which the lenticule is removed through a small arcuate incision.4 It has demonstrated promising visual and refractive outcomes and safety profiles.5–8 It was also shown to be comparable to femtosecond-assisted LASIK.9
The aim of the current study was to compare astigmatic correction in low to moderate myopic astigmatism between SMILE and femtosecond-assisted LASIK using vector analysis.10
Materials and methods
This study was part of a prospective audit of consecutive patients who received SMILE and femtosecond-assisted LASIK between 1 January 2014 and 31 December 2014 at the Hong Kong Laser Eye Center, Hong Kong.
All patients underwent a complete ophthalmic examination and had no ocular abnormality except myopia and myopic astigmatism with a best-corrected distance visual acuity of 20/20 or better in both eyes. Patients with myopia of ≥1.0 D and corneal astigmatism of ≥0.25 D were included in the current study. Patients with corneal thickness of <500 μm, suspicion of keratoconus on corneal topography, cataract, ocular inflammation and infection were excluded. Both surgical options were offered to eligible patients who attended the eye clinic. Consecutive cases during the study period were included in the analysis.
Preoperative examinations included slit-lamp biomicroscopy, dilated funduscopy examinations, uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), manifest refraction and corneal topography (Orbscan IIz, Bausch & Lomb, Rochester, New York, USA)
Small-incision lenticule extraction
The same surgeon (GPMC) performed all surgeries under topical anaesthesia. SMILE was performed using the 500 kHz VisuMax femtosecond laser (Carl Zeiss Meditec, Jena, Germany) using an established technique.5 The following parameters were used: cap thickness, 120 μm; cap diameter, 7.5 mm; lenticule diameter, 6.5 mm with a transition zone of 0.1 mm; cut energy, 1.4 μJ; spot and tracking distance, 2.0–3.0 μm. The back of the intrastromal lenticule was created from periphery to centre of the cornea. The anterior lamellar cut was subsequently created from centre to periphery of the cornea, which extended towards the surface to create a 2 mm incision located at 12 o'clock, from which the stromal lenticule was extracted. A thin blunt spatula was used to separate the lenticule, which was then grasped with a pair of forceps and removed. The corneal interface was flushed with balanced salt solution.
Femtosecond-assisted laser in situ keratomileusis
The same experienced surgeon (GPMC) performed all surgeries under topical anaesthesia. LASIK flaps were created using the 150 kHz IntraLase femtosecond laser (Abbort Medical Optics, Chicago, Illinois, USA). All flaps had a superior hinge with an intended flap diameter of 8.5 mm and flap thickness of 95 μm. Other settings included hinge angle, 55°; bed energy, 0.75 μJ; spot separation, 6 μm; line separation, 6 μm; side-cut energy, 1.1 μJ; pocket width, 200 μm; pocket start depth, 210 μm; and both pocket tangent and radian spot separation, 4 μm. Stromal ablation was performed with Allegretto Wave & Eye-Q 400 Hz laser (WaveLight Laser Technologie, Erlangen, Germany) using a 6.5 mm optical zone. Eye tracker was not used intraoperatively. Following laser ablation of the stromal tissue, the flap was replaced and the stromal bed was washed with balanced salt solution.
Postoperatively, all patients received topical tobramycin 0.3% and dexamethasone 0.1% ophthalmic suspension four times a day for 1 week. Preservative-free artificial teardrops were used for 3 months postoperatively.
Follow-up visits were scheduled on day 1, week 1, and 1 and 3 months. Postoperative examinations included slit-lamp biomicroscopy and measurement of UDVA, CDVA and manifest refraction.
Statistical analysis
Only the left eyes were included in the analysis. Astigmatism outcomes were reported according to standardised format.11 Refractive astigmatism at the spectacle plane was converted to the corneal plane using vertex distance of 12 mm. It was then analysed using vector analysis of Alpins, with consideration of the change in the astigmatic axis, measuring three vectors and relationships among them.10 The target-induced astigmatism vector (TIA), defined as the astigmatic change that the surgery was intended to induce; the surgically induced astigmatism vector (SIA), defined as the astigmatic change that the surgery actually induced; and the difference vector (DV), defined as the induced astigmatic change that would enable the initial surgery to achieve its intended target or the postoperative astigmatism. Magnitude of error (ME) is the arithmetic difference between the SIA and TIA. Angle of error (AE) is the angle between the axis of the SIA and TIA.
Statistical analysis was performed using PASW software V.18.0 (SPSS/IBM, Chicago, Illinois, USA). Independent t test was used to compare continuous variables between groups. Paired t test was used to compare continuous variables within a group. Bonferroni correction for multiple comparisons was applied. Categorical variables were evaluated using χ2 test or Fisher's exact test.
Results
Overall, 111 eyes (111 patients) were included in the study. There were 54 eyes in the SMILE group and 57 eyes in the LASIK group. The mean age of the patients was 32.6±9.4 years and 31.3±8.1 years in SMILE and LASIK groups, respectively (p=0.367). No significant differences were observed in manifest spherical equivalent (p=0.182), manifest sphere (p=0.298), manifest cylinder (p=0.077) and CDVA (p=0.595) between the two groups preoperatively (table 1). All surgeries were uneventful without any intraoperative complications.
Preoperative characteristics of patients undergoing small-incision lenticule extraction (SMILE) and femtosecond-assisted laser in situ keratomileusis (LASIK)
Visual acuity and refraction
All eyes had emmetropia as the target refraction. The logarithm of minimum angle of resolution UDVA at 1 and 3 months were better in the LASIK group (p<0.009). No significant differences were observed in manifest spherical equivalent (p>0.597) and manifest sphere (p>0.489) between the two groups postoperatively. Postoperative cylinder was higher after SMILE compared with LASIK (p<0.001). No significant difference was noted in visual acuity and refraction measured between 1 and 3 months after SMILE (p>0.161) and LASIK (p>0.368) (table 2).
Postoperative characteristics of patients undergoing small-incision lenticule extraction (SMILE) and femtosecond-assisted laser in situ keratomileusis (LASIK)
Efficacy and safety
At 1 month, 41 (76%) eyes in the SMILE group and 54 (95%) eyes in the LASIK group achieved a UDVA of 20/25. These proportions remained unchanged at 3 months postoperatively in both groups. No difference was found in the efficacy between 1 and 3 months in both groups (p=0.100 for SMILE; p=0.135 for LASIK). The efficacy index, which was calculated as the ratio of postoperative UDVA over preoperative CDVA, was 0.87±0.20 after SMILE and 0.95±0.10 after LASIK at 1 month (p=0.002). The corresponding values after 3 months were 0.85±0.20 and 0.94±0.12, respectively (p=0.005).
At 1 month, 9 (16.7%) eyes in the SMILE group and 4 (7.0%) eyes in the LASIK group lost ≥1 line in CDVA. At 3 months, the corresponding numbers were 4 (7.4%) and 3 (5.3%) eyes, respectively. In both groups, none of the eyes lost ≥2 lines in CDVA at 3 months. The safety index, which was determined as the ratio of postoperative CDVA over preoperative CDVA, was 0.96±0.11 after SMILE and 0.98±0.06 after LASIK at 1 month (p=0.286). The safety index at 3 months was 0.97±0.06 after SMILE and 0.98±0.06 after LASIK (p=0.458). No difference was found between 1 and 3 months in both groups (p=0.290 for SMILE; p=0.621 for LASIK). The visual outcomes for both groups at 3 months are shown in figure 1.

Visual outcomes for small-incision lenticule extraction (white) and femtosecond-assisted laser in situ keratomileusis (grey) at the end of 3 months postoperatively. (A) Cumulative percentage of eyes attaining specified cumulative levels of postoperative uncorrected distance visual acuity (UDVA). (B) Difference between postoperative UDVA and preoperative corrected distance visual acuity (CDVA). (C) Change in preoperative and postoperative CDVA.
Predictability
At 1 month, 88.9% and 96.5% of eyes were within ±1.0 D of emmetropia after SMILE and LASIK, respectively (p=0.155). At 3 months, the corresponding values were 94.4% and 98.2% (p=0.355).
In the SMILE group, 68.5% of eyes were within ±0.25 D and 85.2% of eyes were within ±0.50 D of the attempted cylindrical correction at 1 month. The corresponding values at 3 months were 70.4% and 87.0%. In the LASIK group, 94.7% of eyes were within ±0.25 D and 98.2% of eyes were within ±0.50 D of the attempted cylindrical correction at 1 month. The corresponding values at 3 months were 96.5% and 98.2%. The differences between the two groups were statistically significant at 1 and 3 months (p<0.029). The refractive outcomes for both groups at 3 months are shown in figure 2. Stability of spherical equivalent for both groups is shown in figure 3. Between 1 and 3 months postoperatively, 7.4% and 3.5% of eyes changed >0.50 D after SMILE and LASIK, respectively.

Refractive outcomes for small-incision lenticule extraction (SMILE) and femtosecond-assisted laser in situ keratomileusis (LASIK) at the end of 3 months postoperatively. (A) Attempted versus achieved manifest spherical equivalent (SEQ) correction in dioptres for SMILE and (B) LASIK. (C) Percentages of eyes within different dioptre ranges of the intended correction in SEQ after SMILE (white) and LASIK (grey). (D) Percentage of eyes attaining specified levels of astigmatism before (white) and after (grey) SMILE and (E) LASIK.
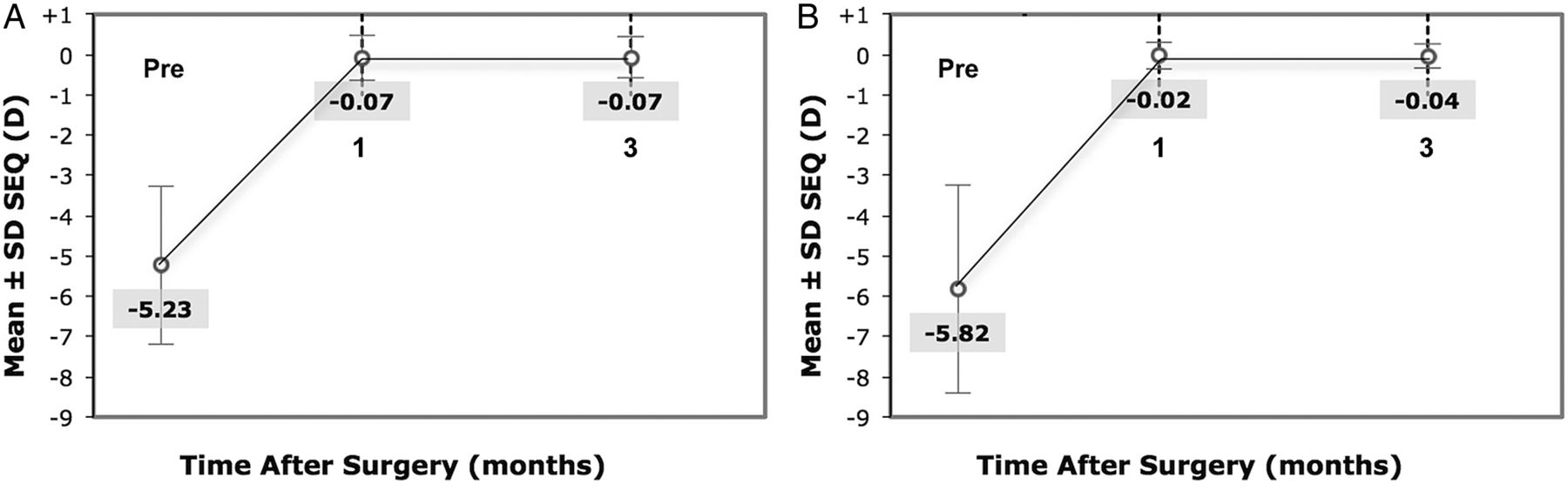
Time course of manifest spherical equivalent (SEQ) after small-incision lenticule extraction and femtosecond-assisted laser in situ keratomileusis.
Vector analysis
The vector analysis results using 1-month and 3-month refractive data are shown in table 3. There was no significant difference in the arithmetic means of TIA (p=0.091) and AE (p>0.596) between the SMILE and LASIK groups. The arithmetic mean of SIA was significantly lower in the SMILE group (p<0.023), while the arithmetic means of DV (p<0.001) and absolute means of AE (p<0.016) were significantly higher in the SMILE group. No significant difference was found in these parameters between 1 and 3 months in both groups (p>0.195 for SMILE; p>0.122 for LASIK). Scatterplots of TIA versus SIA for both procedures at 3 months and the corresponding distribution of AE for both groups are shown in figure 4.
Vector analysis of astigmatic correction at 1 and 3 months after small-incision lenticule extraction (SMILE) and femtosecond-assisted laser in situ keratomileusis (LASIK) using Alpins method

Vector analysis for small-incision lenticule extraction (SMILE) and femtosecond-assisted laser in situ keratomileusis (LASIK) at the end of 3 months postoperatively. (A) Target-induced astigmatism vector versus surgically induced astigmatism vector after SMILE and (B) LASIK. (C) Distribution of angle of error following SMILE (white) and LASIK (grey).
At 3 months, the correction index (CI), defined as the ratio of SIA to TIA, was 0.94±0.44 in the SMILE group and 1.04±0.17 in the LASIK group. Index of success (IS), defined as DV divided by TIA, was 0.14±0.64 in the SMILE group and 0.01±0.19 in the LASIK group. Flattening index, defined as the ratio of the amount of astigmatism reduction achieved by the effective proportion of the SIA at the intended meridian to TIA, was 0.69±0.86 in the SMILE group and 0.71±0.77 in the LASIK group.
The double-angle plots for preoperative TIA and postoperative DV for SMILE and LASIK are shown in figure 5. With-the-rule astigmatism was predominant in both groups preoperatively. After SMILE, the average mark moved closer but did not reach the origin and cross the axes, signifying undercorrection. After LASIK, the average mark moved to the origin, signifying excellent astigmatic correction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Double-angle plots for preoperative target-induced astigmatism (open triangle) and postoperative difference vector at postoperative 1 month (cross) and 3 months (open circle) after small-incision lenticule extraction (left) and femtosecond-assisted laser in situ keratomileusis (right). The filled triangle represents the average preoperative target-induced astigmatism; the filled circle represents the average postoperative difference vector at 3 months.
Subgroup analysis based on the degree of TIA was performed. Eyes were divided into two groups based on the average TIA (1.07 D) of our patients. In eyes with low TIA (0.57 D), only DV was significantly different between SMILE and LASIK (p=0.005). On the other hand, SIA, DV, ME and absolute AE were significantly different between both groups in eyes with moderate TIA (1.75 D) (p<0.010) (table 4).
Subgroup analysis of astigmatic correction based on the degree of target-induced astigmatism at 3 months after small-incision lenticule extraction (SMILE) and femtosecond-assisted laser in situ keratomileusis (LASIK)
Visual and refractive outcomes for both groups at 1 month are shown in online supplementary figures S6 and S7, respectively. Scatterplots of TIA versus SIA for both procedures at 1 month and the corresponding distribution of AE are shown in online supplementary figure S8.
No postoperative corneal complication, such as wound dehiscence, inflammation and infection, was observed in any patient.
Discussion
Previous studies have attempted to evaluate the efficacy, safety and predictability of SMILE.4–6 ,12–15 A recently published review found that 62% of eyes achieved UDVA of 20/20 or better, and 93% of eyes achieved UDVA of 20/40 or better after SMILE.16 The corresponding values were 48% and 93% in our study after 3 months postoperatively. In a prospective analysis of 670 eyes, the efficacy index was 0.90 at 3 months after SMILE12 compared with 0.85 observed in our study.
As for the safety of SMILE, 83–97% of eyes had no loss of CDVA.4–6 ,12–15 The proportion of eyes that lost ≥2 lines of CDVA ranged from 0% to 2.3%.4–6 ,12–15 A recent review reported that 91% of eyes had improved or maintained CDVA and 1% of eyes lost ≥2 lines of CDVA at 6 months after SMILE.16 We observed that 92.6% of eyes had no change in CDVA, and no eye suffered ≥2 lines loss of CDVA at the end of 3 months.
In a prospective study comparing the visual outcomes between SMILE and femtosecond-assisted LASIK for 3 months, the efficacy indices were 1.04 and 1.10 for SMILE and LASIK, respectively.13 Both surgeries had a safety index of 1.01. At 3 months, 98% of post-SMILE eyes and 100% of post-LASIK eyes achieved within ±1.0 D of emmetropia.13 Another comparative study between SMILE and femtosecond-assisted LASIK reported that more eyes achieved a UDVA of 20/20 or better after SMILE compared with LASIK at 3 months postoperatively.9 Furthermore, the safety and predictability, as indicated by a gain in CDVA and postoperative refractive error, were significantly better after SMILE. Our study showed that SMILE had a lower efficacy compared with LASIK by 3 months. This could be partly attributed to the lower predictability in cylindrical correction observed in the SMILE group. As stated by Reinstein et al,7 SMILE for low myopia appears to be as effective and safe as LASIK although the early visual recovery is slightly slower for SMILE.
Accurate astigmatic correction is essential for achieving optimal unaided distance vision after refractive surgery.17 Studies on astigmatic correction using vector analysis reported undercorrection of astigmatism in highly astigmatic eyes but overcorrection in eyes with low preoperative astigmatism after femtosecond-assisted LASIK.18 ,19 In a study analysing astigmatic correction with the earlier flap-based femtosecond refractive lenticule extraction (FLEx), undercorrection was observed in eyes with low astigmatism.20 Similarly, undercorrection in astigmatic error was also noted after SMILE.15 ,21 In a comparative analysis of astigmatic correction after FLEx and microkeratome-assisted LASIK, both techniques yielded good clinical and refractive results.22 Another study on astigmatic correction after SMILE and FLEx showed undercorrection of astigmatism using vector analysis for both techniques at 3 months. The reported success following SMILE was comparable to the findings of our study.23 In the current study, we specifically compared the astigmatic correction between SMILE and LASIK in patients with low to moderate astigmatism. Although the residual spherical equivalent was similar between both groups, residual cylinder was significantly higher after SMILE. This was better illustrated in the vector analysis. The postoperative astigmatism or DV as well as the IS was higher after SMILE, indicating lower ‘success’ in correcting the astigmatism with SMILE compared with LASIK. Moreover, SIA was lower and the derived CI was <1 after SMILE, suggesting undercorrection of astigmatism after SMILE. The coefficient of adjustment (CA), which is the inverse of CI, was 1.07, indicating that an increase of 7% in the magnitude of treatment can potentially improve the outcomes of SMILE in our study. On the other hand, CI and CA were close to 1 in the LASIK group, along with a very low IS, indicating excellent results for astigmatic correction after femtosecond-assisted LASIK. The observed difference between SMILE and LASIK in our study could be explained by the alignment of treatment. In both groups, the mean AE was close to 0, demonstrating absence of systematic misalignment. However, absolute AE was significantly higher in the SMILE group, indicating variable alignment of flattening.
Vector analysis demonstrates that the proportion of loss of flattening effect is 1.5% when treatment is misaligned by 5°, 13.4% when 15° and as high as 50% when 30°.24 The effect is lost totally when the treatment is misaligned by 45°. This emphasises the importance of treatment alignment for successful correction of astigmatism, in addition to the treatment magnitude. The high absolute AE observed in the SMILE group may be attributed to axis rotation or decentration during surgery12 and healing pattern postoperatively.25 In SMILE, two lamellar cuts are performed, and the two stromal surfaces come together after the lenticule is extracted. Additional surgical manipulation is required to separate the lenticule for its removal after the laser cut, which has been suggested to cause topographic irregularities in a small proportion of eyes after SMILE.8 Further subgroup analysis in our study showed that the difference in absolute AE between SMILE and LASIK was significant for eyes with moderate preoperative astigmatism. This could explain the less favourable astigmatic correction observed in SMILE compared with LASIK especially in eyes with a higher degree of cylinder.
Although the same experienced refractive surgeon performed surgery in all the cases in our study, comparing early SMILE cases with femtosecond-assisted LASIK, which has been adopted for years, could limit the conclusions of our study. Another limitation was the short follow-up period and retrospective design. Ivarsen et al15 observed that eyes, which lost ≥2 lines of CDVA at 3 months, recovered to within 1 line of the preoperative CDVA in a late re-examination. A study evaluating interface backscatter observed higher values after SMILE compared with LASIK persisting up to 3 months postoperatively. The values became comparable to LASIK after 6 months, supporting a hypothesis of delayed healing following SMILE.26 The difference in visual recovery may also reflect a differential stromal response to excimer laser and femtosecond laser used in LASIK and SMILE. Kobashi et al23 observed a stable refraction since the first week following SMILE. Only 3.8% of eyes changed more than 0.50 D from postoperative week 1 to month 3. Likewise, our refractive results between 1 and 3 months were not significantly different, suggesting that astigmatic correction might become stable after the first postoperative month. Future long-term prospective studies using corneal astigmatism with keratometric or topographic vector analysis could better reveal any difference between SMILE and femtosecond-assisted LASIK.
Based on the findings of our study, SMILE offered a less favourable astigmatic correction comparable to femtosecond-assisted LASIK in eyes with low to moderate myopic astigmatism. Future work is required to enhance the alignment of treatment in SMILE.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
Footnotes
Correction notice This article has been changed since it was published Online First. The correct Figures 1 and 4 have been used.
Contributors Concept and design: TCYC, ALKN, GPMC and VJ. Analysis and interpretation: TCYC, ZW, CY and VJ. Writing the article: TCYC and ALKN. Critical revision of the article: TCYC, ALKN, GPMC, VCPW, CCYT and VJ. Final approval of the article: TCYC, ALKN, GPMC, ZW, CCYY, VCPW, CCYT and VJ. Data collection: GPMC and ZW. Provision of materials, patients or resources: GPMC and VJ. Statistical expertise: ZW and CY. Literature research: TCYC, ALKN, GPMC, ZW, VCPW and VJ. Administrative, technical or logistic support: GPMC and VJ.
Competing interests None declared.
Ethics approval The Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee approved the study protocol and the study adhered to the tenets of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance