Article Text

Abstract
Background Choroidal naevomelanocytic lesions are often identified as an incidental finding by community optometrists and referred for expert evaluation in hospital eye units or specialist ocular oncology centres. Optimal management strategy is undecided and most centres err on the side of caution. Our aim was to test a virtual model of service delivery relying on interpretation of imaging test results by non-medically trained graders.
Methods Patients with naevomelanocytic lesions referred to Manchester Royal Eye Hospital and Moorfields Eye Hospital were retrospectively included in this study. All patients underwent imaging tests including optical coherence tomography and ultrasound and management was subsequently decided clinically. Images were anonymised and transferred to the Moorfields Eye Hospital Reading Centre and were reviewed by a trained, masked grader who reached a management decision on the basis of a specific grading protocol. Agreement between decisions made on the basis of clinical examination and imaging (‘gold standard’) by an expert ophthalmologist in the clinic was compared with the decisions made by a masked ophthalmologist and a masked non-medical grader based on imaging tests alone.
Results There were 102 consecutive patients included in this study. Agreement between gold-standard clinical management and decisions made by masked, non-medical grader and masked ophthalmologist on the basis of imaging test results alone was 96.1% (κ=0.97) and 100%, respectively.
Conclusions In this pilot study, a streamlined, dedicated, virtual service for rapid assessment (within 2 weeks of referral) of choroidal naevomelanocytic lesions was shown to be feasible and safe. Such a model of service delivery may prove cost-efficient while optimising patient experience. Further prospective studies are required for formal validation of the proposed service model.
- Diagnostic tests/Investigation
- Imaging
- Neoplasia
Statistics from Altmetric.com
Introduction
Choroidal naevi are very common, usually innocuous lesions, often found on routine optometrist sight tests. It is estimated that approximately 6% of Caucasians have a choroidal naevus with a lower prevalence observed in other racial groups.1–3 On the contrary, choroidal melanoma is a rare potentially vision and life-threatening ocular lesion, manifesting in approximately six in one million white persons.1 There have been several studies that have attempted to pinpoint clinical findings and features on imaging tests credibly differentiating small choroidal melanoma from choroidal naevus.2–5 Established risk factors for growth include ultrasound thickness over 2 mm, subretinal fluid, history of symptoms, orange pigment overlying the surface of the lesion and lesion margin within 3 mm of the optic disc.2–5
The issue of managing choroidal naevi is not a trivial one. Given the tendency to err on the side of caution, there is evidence of excessive referrals challenging service delivery in both tertiary eye units and specialist ocular oncology services.6 Although previous studies have examined the natural history and risk factors for growth of choroidal naevomelanocytic lesions, optimal delivery of management remains uncertain.2–5 Management approaches display diversity with respect to the number and type of baseline investigations, the duration and frequency of monitoring of relevant patients.2–5 ,7–9
Using skills of allied health professionals in appropriate cases would allow streamlining service delivery in a socialised healthcare system, maximise capacity and allow community services to play an enhanced role. However, the evidence for this model of delivery is lacking. The purpose of this pilot study was to test the safety and validity of a one-stop virtual clinic model relying on allied health professionals working to strict criteria and to compare against ‘gold standard’ assessment in tertiary hospital naevus clinics.
Methods
This was a retrospective analysis of the clinical details and imaging of patients attending the naevus clinics at the Manchester Royal Eye Hospital (MREH) and Moorfields Eye Hospital (MEH). As part of their routine care, these patients had a full ophthalmic and medical history and imaging tests carried out by an expert ophthalmologist with experience in the management of choroidal naevomelanocytic lesions. Imaging tests included wide-field colour imaging, autofluorescence imaging (AF), optical coherence tomography (OCT) and B-scan ultrasonography. Imaging tests were undertaken by trained imaging and/or ultrasound technicians. Management decisions were made by the ophthalmologist in clinic and allowed for one of three options:
discharge back to the care of the optometrist,
follow-up in the Naevus clinic at a set interval and
referral to a specialist ocular oncology service.
The decision-making algorithm depended on the level of suspicion ascribed to each lesion and is provided in detail in table 1.
Grading protocol for masked grader and ophthalmologist: the following features were graded by Reading Centre graders and by expert ophthalmologist in a masked fashion
All patients attending the naevus clinics were eligible for this study. Patients who were then diagnosed with alternate pathologies other than choroidal naevomelanocytic lesions (erroneous referrals) were excluded from further analysis. Recognition of alternate pathologies by graders was an additional outcome measure for this project.
Imaging data were extracted from MREH/MEH electronic databases and was securely transferred to the Moorfields Eye Hospital Reading Centre (MEHRC), London, in a pseudo-anonymised and coded form. A tracing number was allocated to each case, corresponding to each individual patient and the relevant patient list was retained within the electronic infrastructure of the respective naevus clinics. This allowed linking data back to patients in case this was required. Imaging data were assessed by experienced non-medical graders in the Reading Centre on the basis of the study grading protocol (see table 1) and a management decision was requested for each case to be made by the grader, as per a detailed decision-making algorithm (table 2). All graders were specialist optometrists trained and accredited for the diabetic retinopathy programme with extensive experience of grading for clinical trials in the context of the Reading Centre. Data available to the grader included all imaging test results (wide-fundus colour image, AF, B-scan ultrasound and OCT). The availability of a wide-field colour fundus image and a B-scan ultrasound were the minimum requirements for proceeding with the grading process. Imaging data were provided to the grader in case-folders containing a colour fundus image, B-scan ultrasound, AF image and OCT scan traversing the highest point of the lesions in each case. In cases of increased autofluorescence, an estimation of its origin was offered by the ophthalmologist or grader. Subtle, faint AF would be attributed to drusen alone as opposed to bright, intense autofluorescence attributable to lipofuscin or subretinal fluid. On OCT, grader was required to document the presence or absence of subretinal fluid and presence or absence of elevation of the choroid. Images would be read and graded in the same order on a study-specific spreadsheet. In terms of patient history, the grader was only made aware of the presence or absence of ‘retinal’ symptoms, such as visual blur, distortion, floaters or flashes, as this is the only parameter relevant to patient history constituting an established risk factor for growth of choroidal naevomelanocytic lesions.2 ,3 Training and certification for the grader were provided by the lead investigator (KB) in accordance with Reading Centre regulations. This involved joint assessment and discussion of 20 sets of imaging tests followed by a certification process consisting of independent grading of 20 cases by the grader previously assessed by the lead investigator. A threshold for successful accreditation was specified at 95% agreement and that was exceeded. The available management decisions to the graders were the same as those for the clinic doctors. The option ‘non-applicable/other’ was also available if the grader identified alternate pathologies other than choroidal naevomelanocytic lesions or a full set of imaging data was missing. As a fail-safe process, all patients were offered a follow-up appointment in the clinic at 6 months, including the ones for whom a decision for discharge to their optician was made. This was meant to verify the appropriateness of original decision making and also in order to fulfil (and test) the requirement by the Royal College of Ophthalmologists guidelines10 for lesion growth to be examined among the criteria for patient referral to specialist ocular oncology services.
Management algorithm
Three pathways for reaching management decisions for patients with choroidal naevomelanocytic lesions were compared: decisions made by Reading Centre graders on the basis of imaging tests alone, decisions made by an expert ophthalmologist (KB) in a masked fashion on the basis of imaging tests alone and decisions made in clinic on the basis of imaging tests and direct clinical assessment (‘gold standard’). The degree of agreement between the gold standard of direct clinical assessment and management decisions reached by the two alternative pathways was calculated. In cases of disagreement in management decisions reached clinically as opposed to the ones reached by the Reading Centre graders, adjudication would take place. An experienced ocular oncologist (MSS) would review imaging data and make a final recommendation for management. Rate of identification of erroneous referrals by grader masked to clinical information and direct patient examination was also examined.
Computation of rates of absolute agreement and κ coefficient with quadratic weights were calculated as a measure of inter-rater agreement. Weights are given to account for ordinal nature of the decisions. Since only management decision for those with choroidal naevomelanocytic lesions were of interest, κ coefficient was calculated considering only those who were diagnosed as such by gold standard.
Results
During the study period (October 2014–March 2015), 102 cases were collected and analysed in the three pathways of gold standard in a naevus clinic, image analysis by a masked ophthalmologist and image analysis by a trained non-medical grader. There were 50 cases from MREH and 52 cases from MEH.
With respect to baseline patient population characteristics, all cases originating from MREH were referred to the hospital eye unit by community optometrists. Of the cases seen in MEH, 42 were referred by community optometrists and 10 were internal referrals from general retinal clinics. There were 90 cases of choroidal naevomelanocytic lesions and 12 cases of erroneous referrals (four cases without any abnormal findings, three non-pigmented lesions, two toxoplasmosis scars and three cases of pigmentary changes secondary to age-related maculopathy). The mean±SD patient age was 43±12 years. Mean best corrected visual acuity at presentation was 0.012±0.14 (LogMar scale).
In terms of grading features associated with risk of growth, there were16 cases with orange pigment identified by clinical examination and there were 18 naevi located within 1 disc diameter (DD) of the optic disc (figure 1). AF imaging was available in 86 (out of 90) cases. In 17 cases increased AF was detected on AF imaging, though in 12 of these cases increased AF was thought to be related to the presence of drusen only (figure 2), as opposed to five cases where it was attributed to lipofuscin or subretinal fluid. OCT images were available in 86 (out of 90) cases. Forty-two scans were performed on the TopCon-2000 device and 44 on the Spectralis device. Subretinal fluid on OCT was detected in eight cases. Twenty-four naevi had thickness ≤1.5 mm on B-scan ultrasound, four between 1.5 and 2.0 mm and only one lesion had thickness of >2.0 mm. The rest of the lesions were undetectable by B-scan. Interestingly, none of the patients had a documented complaint of visual symptoms of retinal origin, such as visual blur or distortion. These results are summarised on table 3.
Features used in the image grading protocol for naevomelanocytic lesions of the choroid

Example of peripapillary choroidal naevus. Annual follow-up in the naevus clinic was recommended by masked grader as per grading protocol. Agreement with gold standard and masked ophthalmologist.

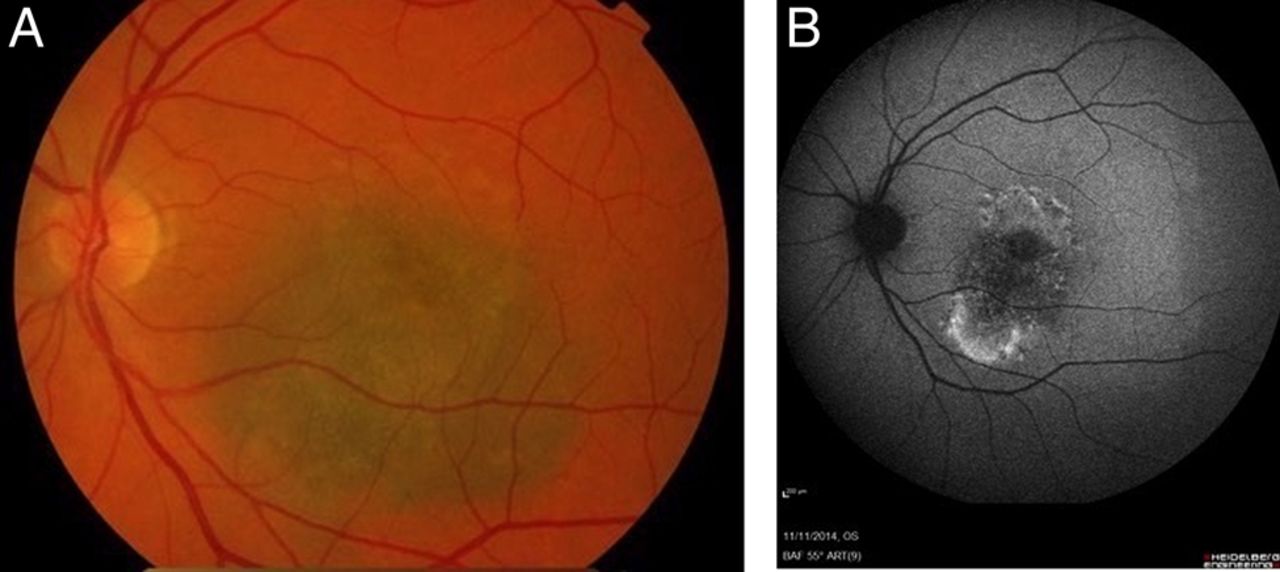
(A) Example of a choroidal naevus with overlying drusen. Masked grader recommended discharge to optician for annual follow-up in accordance with grading protocol. There was agreement with gold standard and masked ophthalmologist assessment. (B) Autofluorescence imaging of the same case. Subtle hyper-autofluorescence accurately identified and attributed solely to drusen by masked grader.
As regards management decisions for relevant patients, 29 of the patients were discharged back to the care of their optician, 53 were followed up in the naevus clinic and eight were referred to ocular oncology service. In the latter group, one was diagnosed with choroidal melanoma and treated with plaque radiotherapy.
Agreement between decision making of gold standard versus masked ophthalmologist and Reading Centre grader
Agreement for management decisions between gold standard and masked grader was excellent at 96.1% (98/102, 95% CI 0.90 to 0.99, κ 0.97), while between gold standard and masked ophthalmologist it was absolute at 100% (102/102, 95% CI 0.95 to 1, κ 1).
Rate of pick up of erroneous referrals by Reading Centre grader
Agreement in the rate of pick of erroneous referrals (ie, non-choroidal naevomelanocytic lesions) between gold standard and masked grader was 98% (100/102), 95% CI (0.92 to 1), κ=0.91, 95% CI (0.79 to 1). A single patient was misdiagnosed as non-choroidal naevomelanocytic lesion by reading centre grading and another one was diagnosed as choroidal naevomelanocytic lesion by reading centre grading but as ‘other’ by masked ophthalmologist and gold standard. These two discrepancies influenced the agreement rates for decision making as well reported above. The former case was a very faint naevus that was not picked up by the grader but was correctly identified by masked ophthalmologist and gold standard. The latter was an elevated minimally pigmented lesion which was diagnosed as a suspicious naevomelanocytic lesion by a Reading Centre grader but was considered as a suspicious non-pigmented lesion by both masked ophthalmologist and gold standard with, however, the same outcome in terms of management with recommendation for referral to ocular oncology.
Agreement between masked ophthalmologist and Reading Centre grader for risk factors of growth
The agreement rate for the presence of orange pigment detected on clinical photographs by a grader in comparison with a masked ophthalmologist was 94%, 95% CI (0.86 to 0.98), κ=0.8, 95% CI (0.64 to 0.97). The agreement location of the lesion within one disc diameter of the optic disc was 97%, 95% CI (0.89 to 0.99), κ=0.89, 95% CI (0.77 to 1).
For the presence of increased AF on AF images, the agreement rate was 93%, 95% CI (0.85 to 0.97), κ=0.88, 95% CI (0.79 to 0.97). Increased AF attributable to drusen only or related to lipofuscin/subretinal fluid had agreement in 95%, 95% CI (0.87 to 0.98), κ=0.87, 95% CI (0.74 to 0.99). Agreement for the presence of subretinal fluid on OCT was 100%, 95% CI (0.95 to 1), κ=1, while agreement for the presence of choroidal elevation on OCT was 98%, 95% CI (0.91 to 0.99), κ=0.96, 95% CI (0.92 to 1).
Discussion
With increasing availability of comprehensive eye checks by community-based optometrists, choroidal naevomelanocytic lesions are a frequent incidental finding. This has been compounded by the widespread use of wide-angle non-mydriatic fundus imaging in the community in settings outside the usual screening for blinding diseases such as diabetic retinopathy. Erring on the side of caution, the seemingly new finding of a pigmented lesion in the fundus prompts referral to ophthalmic hospital services.6 With optometric practice becoming more comprehensive, we believe that such innocent fundus lesions will be found all the more frequently, generating more referrals but also requiring greater resource among ophthalmology services. This report aims to answer the question of whether these low-risk, bland incidental findings might possibly be managed using clinical imaging and algorithms to make appropriate management decisions by non-medically trained health professionals.
Due to the risks of misdiagnosing a choroidal melanoma there is obvious concern to refer many pigmented lesions. There is, however, no universal agreement on the optimal management strategy for these referrals.1–9 Questions such as who should be assessing and monitoring these lesions, how frequent should follow-up be, when is it safe to entrust their care back to community-based optometrists, what are the minimum requirements in terms of baseline investigations so as to confidently ascribe a degree of suspicion for growth to these lesions, even when to refer onwards to a specialist ocular oncology centre, remain largely unanswered. Even referral guidelines to ocular oncology centres issued by the Royal College of Ophthalmologists for relevant pathology contain an element of arbitrariness and are based on the interpretation of the existing literature.10
Choroidal naevomelanocytic lesions have traditionally been diagnosed and managed by medical professionals.1–5 Evidence is lacking on the feasibility of an alternative approach to management of relevant cases relying heavily on allied health professionals, whether these may be specialist imaging technicians or community opticians. This pilot study is the first step towards identifying the optimal management strategy for these cases by generating evidence on the role of non-medically trained health professionals as independent assessors.
In the present work, there was an impressive agreement between masked graders deciding on management on the basis of imaging data alone when compared with the gold standard clinical management. Discrepancy occurred in a single case that was misdiagnosed by the grader as ‘other’, while both the masked ophthalmologist and gold standard assessment identified it as a very faint choroidal naevus. In another case, although both gold standard clinical assessment and masked grader diagnosed a suspicious, elevated lesion warranting referral to ocular oncology, this was considered pigmented by grader but non-pigmented lesion gold standard, and thus fell under the category of ‘erroneous referral’. This discrepancy did not affect management decision for this particular case. Noteworthy is that there was agreement by all three methods for the one case that was diagnosed and treated as a melanoma.
The grading protocol for imaging data from patients with choroidal naevomelanocytic lesions was specifically designed for the purposes of this study and involved identifying known risk factors but also features not commonly associated with increased suspicion for growth of choroidal naevomelanocytic lesions, such as base diameter larger than three disc diameters (figure 3), location in extreme periphery, and presence of more than one lesion. Such grading features were added for the purposes of distinguishing between lesions that are deemed safe to discharge to community opticians as opposed to those requiring follow-up in the hospital-based naevomelanocytic lesions clinic. We tried to anticipate for all possible scenarios of lesion appearance that may render them unsuitable or challenging for follow-up by a community optometrist, such as, for example, extreme peripheral location. Moreover, as the aim of the project was to validate the model of service delivery by trained allied health professionals rather than medical practitioners, robust guidelines for management decision making were devised to eliminate any uncertainty and minimise variability in management.
{kind=link}
{kind=link}
{kind=link}
(A) Large indeterminate naevomelanocytic lesion with orange pigment and subretinal fluid. Referral to ocular oncology was recommended by masked grader as per grading protocol. Accurate identification of orange pigment. (B) Increased autofluorescence accurately identified and attributed to lipofuscin and subretinal fluid by masked grader.
We also included in the grading protocol features originating from various modern imaging modalities with a decisive influence on ascribing suspicion to relevant lesions, such as OCT and AF.11–14 Interestingly, masked graders exhibited excellent agreement with grading by ophthalmologist and even for more ambiguous or difficult imaging features, such as the presence of orange pigment, increased autofluorescence and even estimation of the origin of AF (drusen or lipofuscin/subretinal fluid). In terms of orange pigment, in particular, there was subtle over-reporting by masked grader (19 vs 16 by gold standard) and subtle under-reporting by masked ophthalmologist (13 vs 16 by gold standard). Although this feature was expected to be the most challenging to correctly identify, the rate of agreement reported here is very satisfactory (κ 0.8), though indeed the lowest than for any other imaging feature. For drusen identification, a benign feature, agreement was almost absolute by all assessment pathways.
Though there was high agreement between the different assessment strategies, there must also be a note of caution. In certain cases, there exists a grey area between a suspicious naevus and small melanoma and sometimes even experienced ocular oncologists will classify a lesion as indeterminate, to be followed closely for signs of increasing suspicion. Given that our assessment by any of the strategies involves multimodality imaging, it is plausible that such lesions will be picked out and referred appropriately. Larger prospective studies would help to make this assertion robust.
We recognise the shortcomings in this report. This was a retrospective study, and in view of its pilot nature was not based on formal power calculation. Involvement of a reading centre stemmed from the need to reliably demonstrate the safety of this approach for management of relevant lesions by non-medically trained professionals and on the basis of imaging tests alone. Hence, the graders may be of higher ability than generally available if this system was to be rolled out widely. Allied health professionals, including opticians, imaging technicians or specialist nurses could assume this task following appropriate training. These encouraging preliminary results require a larger scale prospective project to confirm, which must incorporate a health economics analysis to examine financial implications on service delivery while keeping patient safety at the forefront.
Acknowledgments
Retinal Imaging provided by the Manchester Vision Regeneration (MVR) Lab at the Manchester Royal Eye Hospital and NIHR/Wellcome Trust Manchester CRF.
References
Footnotes
Contributors KB had substantial contributions to the conception or design of the work, the acquisition, analysis or interpretation of data, drafting the work, final approval of the version published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. JG had substantial contributions to the acquisition, analysis and interpretation of data, final approval of the version published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. PB had substantial contributions analysis and interpretation of data and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. RA had substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data, revised it critically for important intellectual content, gave final approval of the version published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. DF had substantial contributions to the conception or design of the work or the acquisition, analysis or interpretation of data and final approval of the version published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. TP had substantial contributions to the conception or design of the work or the acquisition, analysis or interpretation of data gave final approval of the version published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MSS had substantial contributions to the conception or design of the work or the acquisition, analysis or interpretation of data, revised the draft critically for important intellectual content, gave final approval of the version published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval Institutional Review Board of Central Manchester University Hospitals NHS Foundation Trust and Moorfields Eye Hospital NHS Foundation Trust.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance