Article Text

Abstract
Background/aims Closure is more difficult to achieve in macular holes that remain open following a previous unsuccessful pars plana vitrectomy (PPV). We present our results with the internal limiting membrane (ILM) translocation technique that is used to optimise outcomes in refractory macular holes.
Methods A prospective, interventional, case series was conducted. 12 eyes of 12 consecutive patients with incomplete sealing of the macular hole (open and type 2 closure) after a previous PPV with ILM peeling were included. Measured baseline parameters included best-corrected visual acuity (BCVA) and macular hole smallest diameter, base diameter and height. Surgeries were performed by harvesting a fragment of the ILM near the vascular arcades and subsequently placing it inside the hole. Postoperative measured outcomes included macular hole status, foveal contour, outer retina integrity, BCVA and surgery-related complications.
Results Anatomic closure occurred in 11 of 12 eyes (91%). This technique elicited a statistically significant improvement in BCVA (p=0.008). Mean BCVA was 20/400 at study baseline and 20/160 at final follow-up. However, less than 16.7% of cases had a final BCVA of ≥20/63.
Conclusion The ILM translocation technique seems to facilitate persistent idiopathic macular hole closure, where primary surgery with PPV and ILM peeling failed.
- Treatment Surgery
- Vitreous
- Retina
- Macula
Statistics from Altmetric.com
Introduction
Idiopathic full-thickness macular holes (MHs) are a frequently recognised cause of central vision deterioration. Its pathogenesis involves a combination of anteroposterior and/or tangential tractions exerted at the vitreoretinal interface.1 ,2 The rationale for the surgical management of this condition is to relieve these tractions by the thorough removal of the vitreous and of proliferations at the retinal surface. The simultaneous peeling of the internal limiting membrane (ILM) restores retinal compliance and reduces the risk of postoperative epiretinal membrane formation.
Kelly and Wendel3 were the first to report successful results of vitreous surgery for MH repair in 1991, and pars plana vitrectomy (PPV) with ILM peeling is currently the standard procedure. In recent publications, closure rates after primary surgery exceed 90%.4 Despite these high success rates, surgical failure is still reported. Anatomic and functional success is more difficult to achieve in these refractory MHs and closure rates of reoperation rarely exceed 70%, usually remaining well below this value.5–7
In 2010, Michalewska et al described a technique for the primary repair of large MHs, where a remnant of an incompletely peeled ILM is used to cover the base of the hole.8 This technique seems to improve both functional and anatomic outcomes of PPV for larger MHs (those with a smallest diameter of ≥400 µm). They hypothesised that the inverted ILM flap provides stimulus and serves as a scaffold to the proliferation of glial cells, thus enhancing hole closure.
The current study reports our initial results with a technique of ILM translocation that has shown promise by enhancing anatomic success in persistent MHs following a previous PPV with ILM peeling.9 The procedure is based on the same presumption as the inverted flap technique, in which the placing of a graft of peripheral ILM inside of the MH promotes its closure.
Materials and methods
Type of study
A prospective, multi-centre, interventional, consecutive case series was conducted.
Patients selection
Patients with a documented incomplete sealing of the MH, with bare retinal pigment epithelium (RPE) after a previous PPV with ILM peeling and gas endotamponade (open and type 2 closure) were included. All MHs were idiopathic in origin, with exclusion of cases associated with trauma and high myopia (defined as an eye with a refractive error of more than −6 D or an axial length in excess of 26 mm). The MHs remained open for at least 1 month after surgery and until complete disappearance of the intraocular tamponade. Spectral domain optical coherence tomography (SD-OCT) scans showed stability of minimum diameter after primary vitrectomy in all cases. Due to the large dimensions of the MHs and the natural history of this pathology, further closure was considered highly unlikely and surgery was undertaken. Patients with concomitant ocular disease capable of causing significant visual acuity loss, such as diabetic retinopathy, age-related macular disease, choroidal neovascularisation or advanced glaucoma, were excluded.
Preoperative evaluation
All patients underwent a comprehensive preoperative examination, with recording of slit-lamp and dilated funduscopic findings. The parameters analysed included baseline best-corrected visual acuity (BCVA), lens status and MH size and index. MH configuration was determined using the Cirrus SD-OCT (Carl Zeiss Meditec, Dublin, California, USA). The parameters measured were smallest diameter; base diameter, measured at the level of the RPE; and height, measured as the distance from the RPE to the innermost aspect of the MH (figure 1). The macular hole index (MHI), described by Kusuhara et al,10 was calculated as the ratio of the hole height divided by the base diameter.
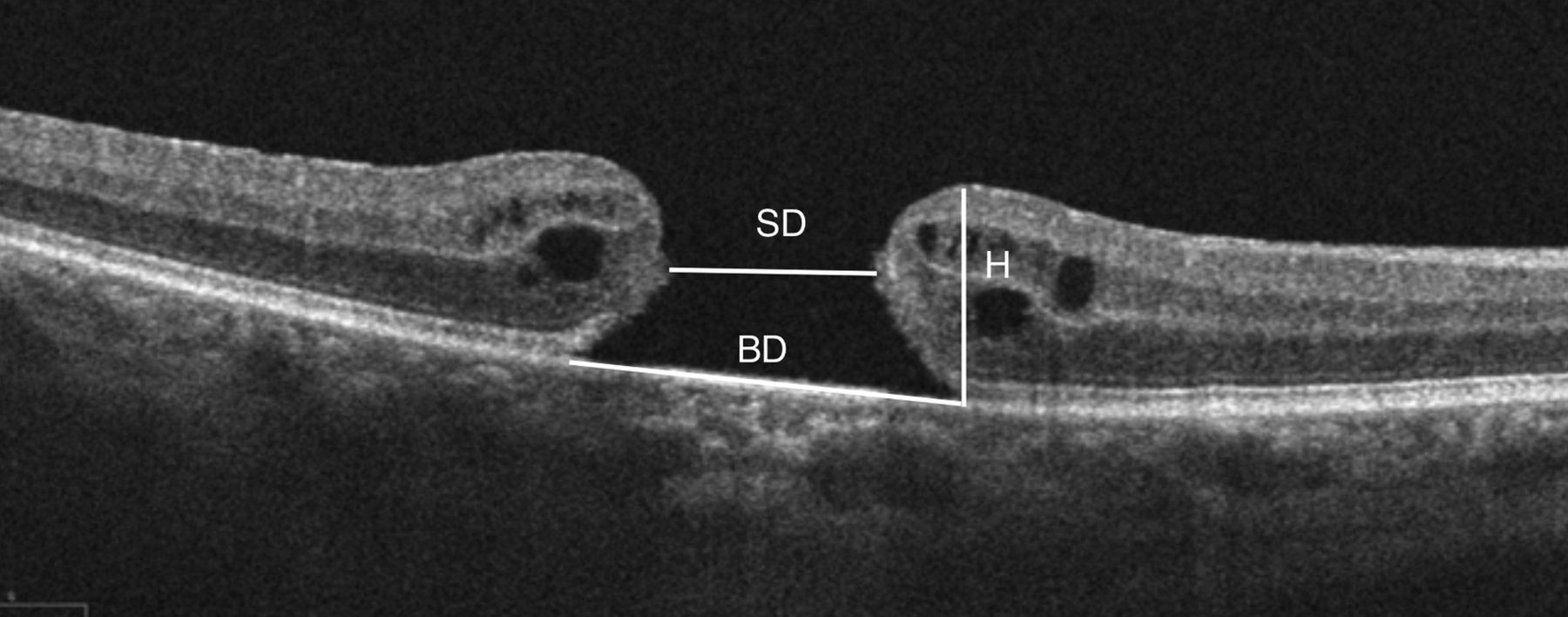
Spectral domain optical coherence tomography image showing refractory macular hole with superimposed scheme of dimension measurements. BD, base diameter; SD, smallest diameter; H, height.
Surgical technique
Patients were retreated by two experienced vitreoretinal surgeons (JN and NLG), at two different centres, in Barcelona (Spain) and Braga (Portugal). All cases had been previously operated on by these two surgeons.
At the time of the first surgery, a complete ILM peel was routinely performed, aided by the use of Brilliant Blue G (Brilliant Peel, Fluorine; Geuder AG, Heidelberg, Germany, 0.25 mg/mL solution). The ILM was peeled in an area centred on the fovea, extending to the optic nerve, close to the superior and inferior temporal arcades and approximately two disc diameters from the fovea nasally. The inverted ILM flap technique was not performed at the time of the primary surgery and no direct trauma to the retina was observed during surgical manoeuvers.
The second procedure consisted of a standard 23-G three-port PPV, assisted by staining of the posterior pole with Brilliant Blue G to confirm the extent and visualise the edges of the previous ILM removal. After dye injection the ILM was noted to be completely removed from the macular area in all eyes and the area of ILM peeling was not enlarged, as it was considered adequate. A fragment of ILM of at least one disc diameter in size was harvested with the use of an end-gripping forceps (Alcon/GRIESHABER 23-G disposable Revolution ILM forceps) close to the vascular arcades, where the edge of the previous peeling was located. This graft was subsequently placed inside the MH and fluid–air exchange was performed. The ILM graft was prevented from dislocating by reducing the infusion pressure of air to 20 mm Hg and carefully aspirating on the nasal side of the optic disc, until a complete fluid–air exchange was achieved. Gas endotamponade with 12% perfluoropropane (C3F8) was used in all cases and patients were instructed to avoid supine position, without any other specific demands for forced positioning (see online video available as supplementary digital content).
Supplemental material
Postoperative evaluation
Follow-up time points included 1 day, 1 week and 1, 3, 6 and 12 months postsurgical evaluations. SD-OCT, BCVA measurement and slit-lamp and fundus examination were recorded at each visit. Hole closure was defined as complete sealing of the MH without bare RPE (type 1 or V-shaped and U-shaped hole closure),11 ,12 and was confirmed by SD-OCT. Foveal contour and integrity of the ellipsoid zone (EZ) were also assessed. Main postoperative parameters analysed included BCVA, anatomic closure after retreatment and intraoperative and postoperative complications associated with the procedure.
Ethical considerations
Our study was carried out with approval from the appropriate institutional review board and adhered to the ethical standards laid down in the 1964 Declaration of Helsinki. The possible risks and benefits of the procedure were explained before surgery and informed consent was obtained from all patients.
Data analysis
Statistical analysis was carried out using the Statistical Package for the Social Sciences (V.22.0) software for MAC (SPSS, Chicago, Illinois, USA). Visual acuity scores were transformed to logarithm of the minimal angle of resolution (logMAR) and finger counting and hand motion acuities were transformed to 2.0 and 3.0 logMAR, respectively. The preoperative and postoperative BCVAs were analysed using the Wilcoxon signed-rank test. Multiple regression analysis was used to evaluate the correlation between the postoperative visual acuity and preoperative variables. A p value of <0.05 was considered significant.
Results
A total of 12 eyes of 12 patients, who underwent PPV with ILM translocation for a persistent MH after PPV with ILM peeling were enrolled. The patients’ age ranged from 68 to 82 years (mean 75 years). Two of the patients were men and 10 were women. All patients were pseudophakic at the beginning of the study. The mean MH smallest diameter was 654.92±196.51 µm (range from 392 to 1073 µm), the mean MH base diameter was 1662.67±688.47 µm (range from 964 to 2847 µm) and the mean MH height was 464.00±106.88 µm (range from 315 to 662 µm). The MHI was inferior to 0.5 in all patients (average of 0.32±0.12).
Cystoid oedema at the edges of the hole was noted in all cases but one (case number 7) and MH margins showed no sign of atrophy in any of the preoperative SD-OCT scans.
Anatomic outcomes
Retreatment of persisting idiopathic MHs with PPV and ILM translocation resulted in anatomic closure in 11 of our 12 cases (91%), as confirmed by SD-OCT imaging. Preoperative and postoperative SD-OCT images of all enrolled patients are shown in figure 2.

Spectral domain optical coherence tomography images showing patients 1 to 12, before (left column) and 3 months after reintervention by pars plana vitrectomy with internal limiting membrane translocation (right column).
Functional outcomes
All patients completed the 12 months follow-up and final BCVAs were obtained at this time. Table 1 summarises BCVAs before and after the ILM translocation procedure and also showcases preoperative dimensions and postoperative outcomes of all the MHs. PPV with the ILM translocation technique elicited a statistically significant improvement in BCVA (p=0.008). Mean preoperative BCVA at the study baseline was 20/400 and mean postoperative BCVA 12 months after reintervention was 20/160. The BCVA improved in nine patients and remained stable in the other three patients, with no cases of vision deterioration after reoperation.
Patient data and main functional and anatomic outcomes
Despite the significant improvement in visual acuity, less than 16.7% of eyes had a final BCVA of ≥20/63.
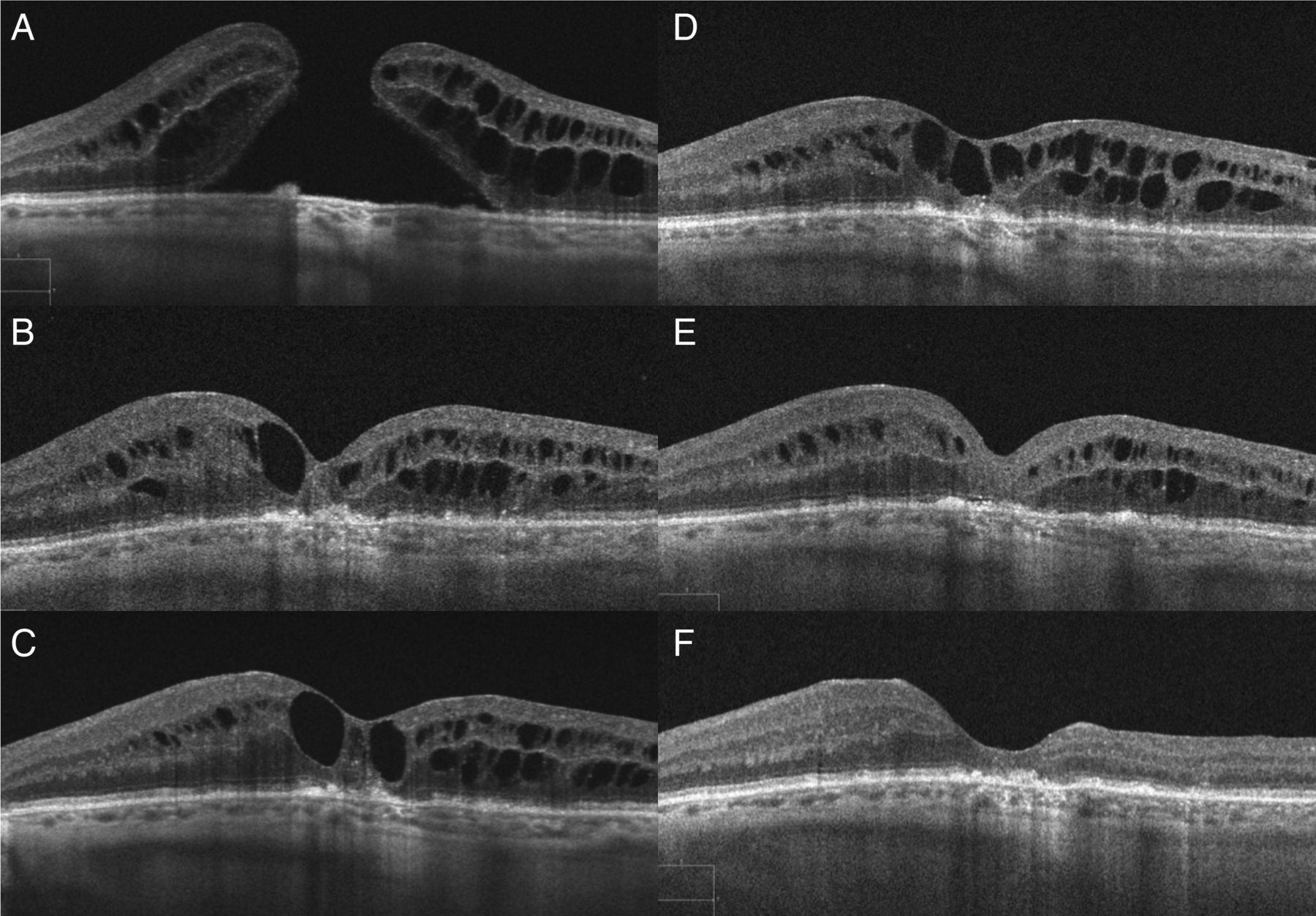
There was one case (case number 12) of persistent MH after reoperation, with the patient declining any further surgery. No late reopening of any MH was observed after successful hole closure during the 12 months follow-up. Case number 10 developed a persistent intra-retinal macular oedema, which resolved after a single injection of a 700 μg dexamethasone implant (Ozurdex, Allergan). In figure 3, we can see the tomographic evolution of this case, with complete resolution of the oedema at final follow-up.

Spectral domain optical coherence tomography images showing patient number 10 (A–F). Before reintervention with pars plana vitrectomy and internal limiting membrane translocation we can see a full-thickness macular hole with raised edges and intra-retinal fluid (A). After the procedure, the macular hole was successfully closed but with persistence of intra-retinal fluid at 1 week (B), 1 month (C) and 3 months (D). At this time, an injection of 700 μg dexamethasone implant (Ozurdex, Allergan) was performed. Partial resolution was documented 2 weeks after implant injection (E), with no residual fluid 12 months after surgery (F).
With regard to the postoperative features of the outer retina architecture, recovery of the EZ was observed in 33.33% of the cases (cases 4, 7, 9 and 11), as evident in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postoperative spectral domain optical coherence tomography images showing four surgically closed macular holes (A–D), after pars plana vitrectomy with internal limiting membrane translocation. Despite macular hole repair, we can see, in all these cases, a hypo-reflective disruption of the normally hyper-reflective ellipsoid zone, with associated unstructured external limiting membrane (between the asterisks).
A multiple regression analysis was run to predict the postoperative BCVA from preoperative variables. No significant correlation was found between independent preoperative variables (namely BCVA, MH smallest diameter, MH base diameter, MH height and MHI) and postoperative BCVA.
There were no significant complications related to the technique or to the surgical procedure.
Discussion
There has been a refinement in surgical technique for MH repair leading to an improvement in functional and anatomic outcomes. Despite the high success rates achieved, MH persistence after primary PPV remains one of its major complications. A recently published meta-analysis has shown that ILM peeling increases the chance of MH closure and it is routinely performed by most surgeons at the time of primary surgery.4 The rationale for this is that perifoveal vitreous contraction and cellular components on the surface of the ILM play a role in the pathogenesis of the MH. ILM dissection ensures the thorough removal of remnants of cortical vitreous and/or epiretinal membranes, relieving all tractions. ILM peeling also activates Müller cells and increases cytokine release and secretion of collagen, basement membrane components and inflammatory factors, stimulating the glial cell-mediated closure of MHs.13 However, there is still a small percentage of patients where surgery fails, even when the ILM is peeled. Anatomic and functional success is more difficult to achieve in these refractory MHs. This might be partly due to the fact that there is little else to do when the posterior hyaloid has been detached and the ILM removed. Several different techniques have been described as adjunctive procedures to attempt closure when reoperating these patients, such as pneumatic retinopexy and repeat fluid–gas exchange,14 PPV with enlargement of previous ILM peel,15 endotamponade with silicone oil16 ,17 or long-lasting gas,7 radial relaxing retinotomies on the margin of the hole18 and laser photocoagulation,19 among others.
The repair of large MHs using a flap of inverted ILM was developed based on the presumption that the presence of the ILM in the bare area of the MH brings adhered cellular remnants of glia and Müller cells. These act as a substrate for proliferation and migration of cells to the centre of the fovea, enhancing MH closure,8 and the surgical trauma induced by the ILM peeling also promotes the formation of a glial scar. Although the inverted ILM peeling technique has been shown to be effective, it can only be performed when the ILM has not been previously peeled, rendering it unsuitable when primary surgery with ILM peeling failed. The presented ILM translocation procedure overcomes this problem. It can also be used in cases in which the ILM flap becomes torn off from the retina surface when attempting a classic inverted flap technique.
The closure rate of secondary procedures for refractory MHs stands well below the results reported after primary surgery. Our MH closure rate compares favourably with those found in other publications.5 However, despite anatomic success being found in 91% of patients and despite the significant improvement in BCVA, the functional results were limited, with only 16.7% of patients attaining a BCVA of ≥20/63. It is well known that anatomic success does not always guarantee a favourable visual prognosis, which seems to hold true for refractory MHs. In our study, complete restoration of the integrity of the EZ was found in only 3 of 12 eyes and it can explain the somewhat disappointing functional results after a seemingly successful surgery.20 ,21
Another variable which has been studied as a predictor of functional improvement after PPV for MH is the MHI and a MHI value ≥0.05 was associated with a greater postoperative visual acuity.10 In our series all cases had a MHI value ≤0.05 and holes with such configuration (with a greater basal diameter) may be more frequently closed by excessive glial proliferation, presenting less viable adjacent photoreceptor layers than eyes with a greater MHI, which may not need as much glial proliferation to close.
It also needs consideration that functional recovery after surgery is gradual and has been reported to continue for up to 2 years.22 Perhaps our cases would have shown better functional results with a longer follow-up period, as EZ defects are likely to decrease for several months after surgery.23 Further, BCVA does not assess other beneficial effects of surgery, such as the reduction of distortion and the elimination of central scotomas, which are known to be important in patients with MHs.24
This study has some limitations that should be acknowledged. These include a small number of patients, a limited follow-up time, the absence of a control group (as this was a non-comparative study) and the fact that the duration of the MHs and the time between the primary surgery and reoperation were not taken into consideration. Further studies with longer observation periods and larger sample sizes are needed. However, large studies of repeat MH surgery are unlikely to be forthcoming because of the high success rate of primary surgery.
In conclusion, this technique seems to facilitate the closure of persistent full-thickness idiopathic MHs, where primary surgery with PPV and ILM peeling failed. Anatomic success rates exceed most of the published results for refractory MHs, but visual acuity improvement was somewhat disappointing. Glial proliferation may be an inevitable process for the sealing of larger MHs, but it may also prevent normal photoreceptor alignment and function from being restored.25 Also, whether it is worth reoperating on MHs with initially unsuccessful surgery and which is the best treatment are two questions that remain unanswered.6 The efficacy of this procedure must be evaluated in a larger population and directly compared with other techniques.
References
Footnotes
Contributors JP, NLG and JN meet authorship criteria and certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript.
Competing interests None declared.
Ethics approval Comissão de Ética do Hospital de Braga.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance