Article Text

Abstract
Aims To report the 25-year longitudinal trends in indications and corneal transplantation techniques in New Zealand.
Methods Statistical analysis of prospectively acquired New Zealand National Eye Bank (NZNEB) electronic database from 1991 to 2015 inclusive. Subjects were recipients of corneal transplants in 62 centres supplied by the NZNEB. Main outcome measures were indications, recipient age and transplantation techniques.
Results From January 1991 to December 2015, NZNEB supplied tissue for 5574 corneal transplants, increasing annually from 89 (1991) to 290 (2015). Penetrating keratoplasty remained the most commonly performed technique throughout the 25-year period, although it decreased from 98.9% of all transplants in 1991 to 60.3% in 2015. There was a corresponding increase in deep anterior lamellar and endothelial keratoplasty over the most recent decade from 2.5% to 7.2% and 4.9% to 31.4%, respectively. Keratoconus remained the leading indication for keratoplasty through to 2015 (34.5%). Regrafts (23.1%) and Fuchs endothelial corneal dystrophy (17.0%) have become more common indications, while bullous keratopathy has become less common (10.8%). There was a bimodal distribution in age with peaks at 20–29 and 60–79 years. There was a reduction in recipients under age 40 and corresponding increase in the percentage of recipients aged 40–69.
Conclusion Changing indications and increasing uptake of lamellar keratoplasty have been significant international trends over the last 25 years. However, New Zealand's corneal disease and population characteristics create unique longitudinal trends, with keratoconus remaining the leading indication and penetrating keratoplasty the leading technique from 1991 to 2015.
- Cornea
- Treatment Surgery
- Epidemiology
- Eye (Tissue) Banking
Statistics from Altmetric.com
Introduction
Since the first successful human penetrating keratoplasty (PK) in 1906,1 corneal transplantation has undergone considerable changes in technique and indication. Globally, surgical techniques have evolved greatly in the last 10 years with most surgical centres reporting a significant increase in endothelial keratoplasties (EK) in particular.2–8 However, reported rates of the uptake of different techniques vary considerably between countries, possibly due to differing indications for corneal transplantation as well as variable adoption of newer techniques.2 ,3 ,6
The pattern of corneal transplantation in New Zealand is relatively unique due to the particularly high prevalence of keratoconus as previously reported for the period 1991–1999.9 More recently, Cunningham et al3 reported the indications and distribution of corneal tissue by analysing the New Zealand National Eye Bank (NZNEB) data for 2000–2009, confirming keratoconus as the most common indication and PK as the most common procedure. Since then, there has been significant uptake of deep anterior lamellar keratoplasty (DALK) and Descemet's stripping automated endothelial keratoplasty (DSAEK), which were widely introduced to New Zealand in 2006 and 2007, respectively (although deeper forms of anterior lamellar keratoplasty (ALK) were occasionally performed from 2003 onwards).
The purpose of the current study was to identify longitudinal trends in types of corneal transplantation and the indications for keratoplasty by exploring and analysing the comprehensive NZNEB database prospectively assembled over the last 25 years (1991–2015 inclusive), thereby providing an overview and an update on previous reports and establishing a current New Zealand perspective.
Materials and methods
Review of the prospectively compiled NZNEB electronic database, containing all records of corneal transplantation from January 1991 and December 2015 inclusive.
During these 25 years, the NZNEB supplied corneal tissue to 62 ophthalmology centres nationwide (20 currently active) and has been the primary supplier of donated corneal tissue in New Zealand since 1991. The database records information about the donor and tissue collected from medical and coroners records at time of death, while patient and surgical data are collected from mandatory questionnaires completed by the surgeons on the day of corneal transplantation surgery. Recipient ages, indications and techniques of transplantation were specifically analysed in this study.
Results
From January 1991 to December 2015, 5574 corneal transplants were performed in 62 public and private centres. During this period, there was an average of 223 corneal transplants per year, ranging from 89 (2.5 per 100 000 population) in 1991 to 319 (7 per 100 000) in 2013 (figure 1). On a simplified linear trend, this amounts to six additional transplants per year over the 25-year period.
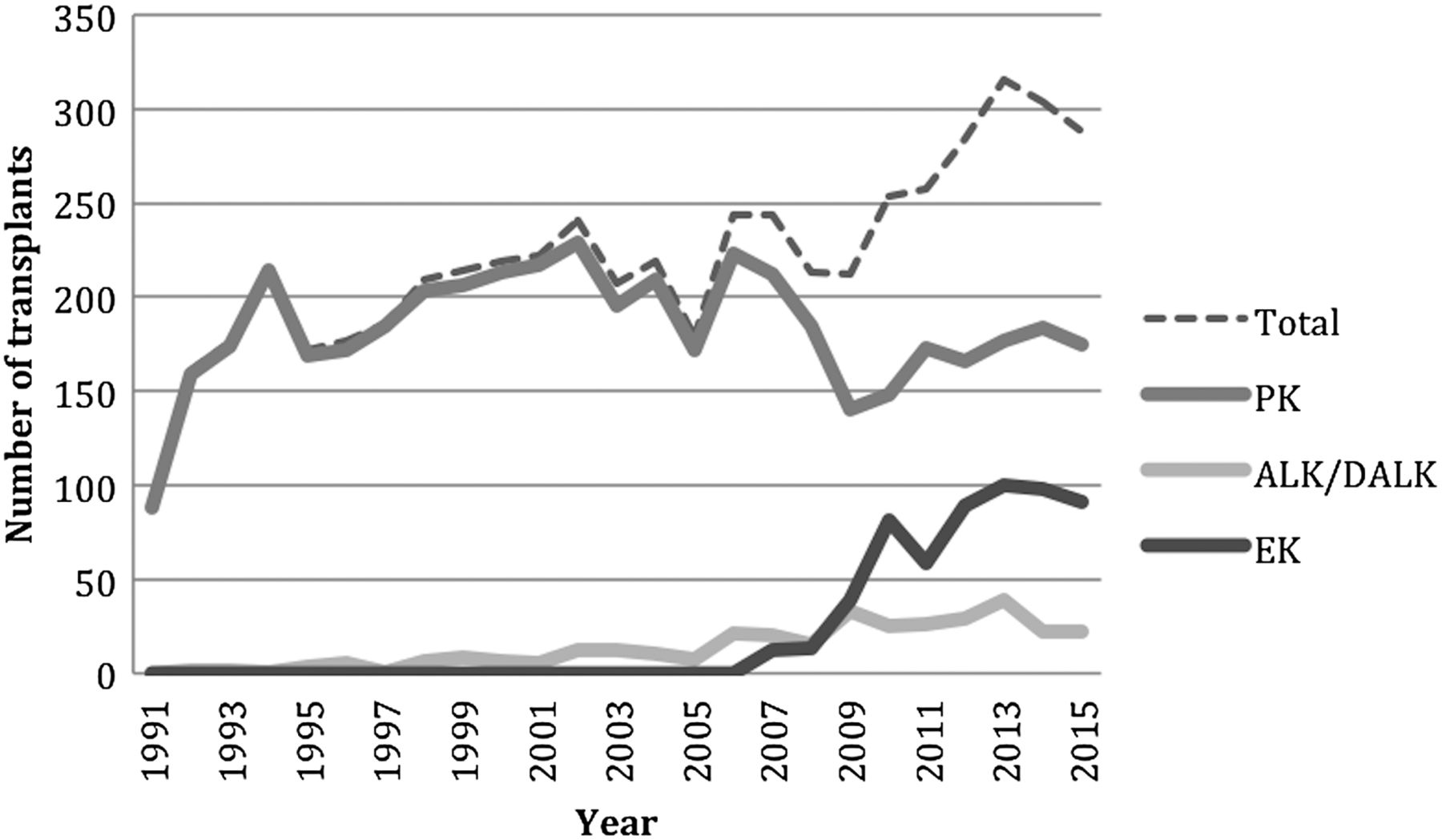
Number of penetrating keratoplasty (PK), deep anterior lamellar keratoplasty/anterior lamellar keratoplasty (DALK/ALK) and endothelial keratoplasty (EK), New Zealand National Eye Bank 1991–2015.
Between 1991 and 2015, 4588 (82.3%) PK, 231 (4.1%) DALK, 101 (1.8%) ALK and 582 (10.4%) EK were performed. The remaining 72 transplants (1.3%) were epikeratoplasties, patch/tectonic grafts or other/non-specified techniques. The annual number of ALK reached a peak of 15 in 2006 but has since been constant at 0–2 cases per year with the introduction of DALK in 2006. The annual number of DALK increased to 33 within 4 years and averaged around 27 per year from 2009 onwards, with a steady ratio around 1 DALK:6 PK. Similarly, there was a rapid uptake of DSAEK since introduction in 2007. The latter accounted for 89 (30.7%) of total annual corneal transplants by 2015. Since the introduction of these newer techniques, there has been a corresponding decrease in the number of PKs from 223 in 2006 (91.4% of total keratoplasties) to 175 in 2015 (60.3% of total keratoplasties).
The age distribution of recipients is displayed in figure 2. Overall, there appears to be a bimodal distribution with one peak at age 20–29 and one peak at 70–79 based on data from 1991 to 2010 (second peak at 60–69 in 2011–2015). Notably, there has been a decrease in the percentage of transplants for recipients aged <40 and an increase for those aged >40, especially in the last five years. The ages of recipients with Fuchs endothelial corneal dystrophy (FECD) were analysed separately and did not show a significant change over the 25 years.
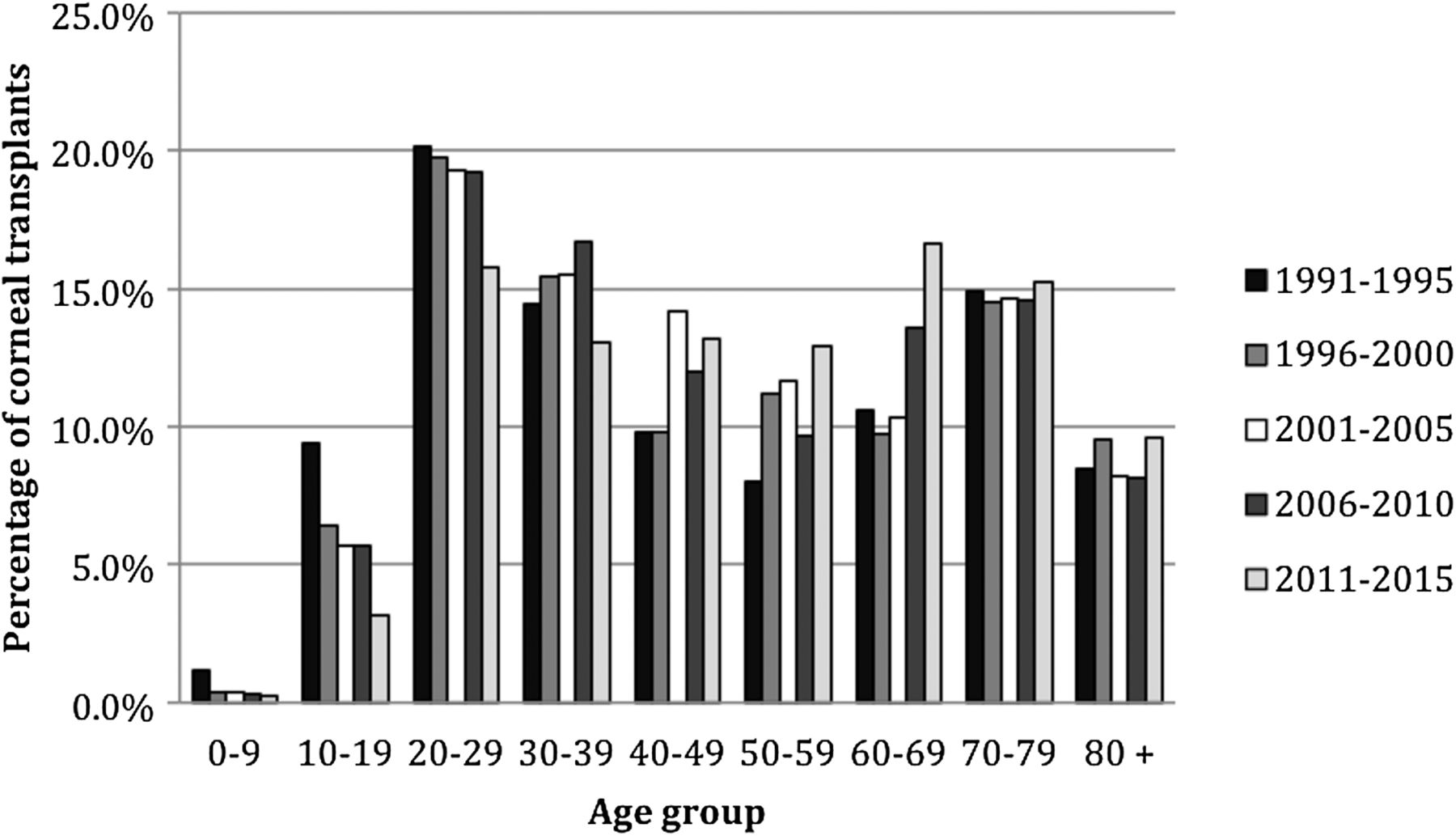
Age distribution of corneal transplant recipients over the study period 1991–2015 subdivided into five consecutive periods.
The indications for corneal transplantation are summarised in table 1. Keratoconus was the leading indication for keratoplasty during the entire period from 1991 to 2015. In 1991–1995, the second most common indication was bullous keratopathy, which became the fourth most common indication by 2011–2015 (9.7% aphakic/pseudophakic and 1.2% unspecified). Regrafts became the second most common indication from the period 2001–2005 onwards. Interestingly, FECD, which was the least common indication in 1991–1995, steadily increased to become the third most common indication by 2011–2015. The proportions of keratoplasties for keratitis, trauma and other corneal dystrophies have fallen significantly over the 25-year period.
Indications for corneal transplantation reported to the New Zealand National Eye Bank, 1991–2015
The trends of the top five indications for corneal transplant over time are shown in figure 3.

Five most common indications for corneal transplantation reported to the New Zealand National Eye Bank 1991–2015 (n=5043 transplants).
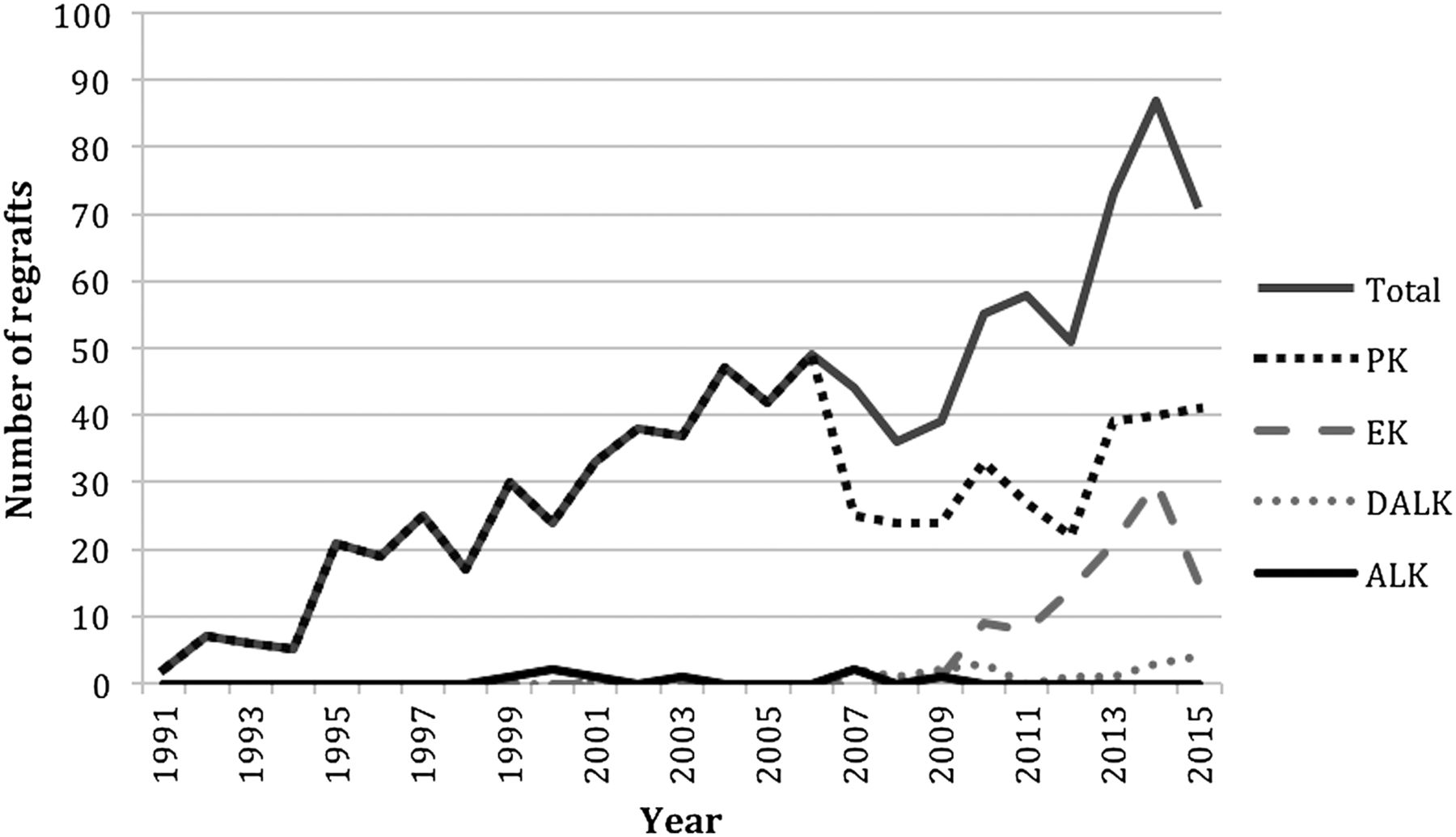
The initial techniques of corneal transplantation in regrafts are shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Initial technique of corneal transplantation in 921 regrafts reported to the New Zealand National Eye Bank, 1991–2015. Total includes 119 cases of regrafts between 2007 and 2015 where the initial technique of transplantation was unknown and two cases of repeat patch grafts. ALK, anterior lamellar keratoplasty; DALK, deep anterior lamellar keratoplasty; EK, endothelial keratoplasty; PK, penetrating keratoplasty.
Discussion
This study examined changes in the indications and techniques for keratoplasty in New Zealand—a small, geographically isolated country with a single national eye bank and a government-funded public health service, pre-dating, but similar to the British National Health Service. During the period studied, the New Zealand population increased from 3.4 million (1991) to >4.6 million people (2015),10 and the number of recorded keratoplasties annually increased from 89 to 290 (2.5 to 6.3 per 100 000 population) in this period. However, in the initial few years, more tissue may have been acquired locally without involving the NZNEB and the current data represent only the tissue supplied by the NZNEB. Similarly, in Canada, there was a recent steady increase in annual number of keratoplasties to 12.6 transplants per 100 000 by 2011.4
Apart from the growing population, possible explanations for the increasing trend may be the growing number of indications or cases amenable to treatment with corneal transplantation, and improved tissue processing, storage and use.11 Also, with the adoption of newer transplantation techniques, such as EK, and an increased number of subspecialty trained corneal surgeons, the clinical threshold for performing keratoplasty may have changed during the study period.
Indications for keratoplasty have changed substantially and correlate temporally with advancements in cataract surgery. In 1991, keratoconus, bullous keratopathy and keratitis were the top three leading indications for keratoplasty in New Zealand. However, the routine use of viscoelastic devices and phacoemulsification in cataract surgery and the use of improved intraocular lens designs have likely contributed to the decrease in bullous keratopathy in more recent years.7 Following analysis of data from the Eye Bank Association of America, Park et al2 also reported a reduction of pseudophakic bullous keratopathy (PBK) as an indication from 20% in 2005 to only 9% in 2014. In Singapore, the most common indication was PBK/ABK, which is noteworthy as the New Zealand population has become more ethnically diverse, especially with a significant increase in the Asian population (5.2% to 12.2% from 1996 to 2013).10 ,12 However, the Singaporean study is based on 1991–2003 results and lately there may have been a similar reduction of bullous keratopathy in Asians too due to the improvements in cataract surgery. Bullous keratopathy is not only less common, but is also an indication that is now more frequently managed with EK than PK, thereby contributing to the shift in transplantation techniques.2
From 2003, the number of regrafts had increased to become the second most common indication. The growing proportion of regrafts is unsurprising in an ageing population given that graft survival is limited. This may be more noticeable in New Zealand where many of the transplantations are performed for young keratoconic patients. However, the data do not reveal how many of the regrafts were performed on initial or repeat grafts, which may be of interest in future research. Also, an increase in the number of subspecialty trained corneal surgeons in New Zealand may have lowered the clinical threshold for performing regrafts and increased patient access to surgery.
The initial keratoplasty technique was identifiable in 800/921 regrafts, and the overall trend of regrafts in respect to initial keratoplasty techniques followed the trend in the overall number of transplants per technique. Having been introduced during the 25-year period studied, failed EK grafts have been a new indication for regrafts, adding to the overall numbers, especially in the introductory phase of the surgical learning curve. Furthermore, the option of EK may also have permitted more patients to undergo repeat transplantation as it is generally less invasive and involves a shorter period of visual recovery.
FECD was the third most common indication in 2011–2015, which may be explained by multiple factors involved in its management. The increased use of technology such as specular and in vivo confocal microscopy, pachymetry and tomography may have enabled the detection of failing corneas at an earlier stage and more accurate diagnoses.13 Furthermore, patients may be undergoing transplantation at lower levels of visual disability due to the availability of DSAEK and its advantage of rapid recovery. Our data suggest that the mean age of recipients has not changed over the years, but the expanding aged population in New Zealand may cause a greater increase in age-related indications like FECD. Cases of non-Fuchs corneal dystrophy were mostly classified as ‘other corneal dystrophy’ rather than ‘unspecified corneal dystrophy’, thus the possibility that some cases of FECD were initially misclassified is minimal.
According to the Eye Bank Association of America data, FECD was the most common indication for any keratoplasty. However, the number of PKs for this indication has dropped significantly (14% to 3%) with the advent of DS(A)EK and Descemet's membrane endothelial keratoplasty (DMEK), which are now the preferred types of transplantation for FECD.2 ,6 FECD has also been the leading indication for keratoplasty in Canada since 2007.4 It is interesting to note that the percentage of keratoplasties for FECD has increased while it has decreased for bullous keratopathy, as in British Columbia.4 In the USA, combined domestic and international numbers of keratoplasty indicate an increase of 58% for FECD from 2008 to 2014 and only 14% for bullous keratopathy. Of course, corneal decompensation may be more readily attributed to FECD, rather than PBK, following cataract surgery. Although our data do not include lens status at the time of keratoplasty, this information would be of great value in analysing the current trends.
In New Zealand, keratoconus remains the leading indication for corneal transplantation unlike most other developed countries.2 ,4 ,6 Keratoconus appears to be unusually common in New Zealand, with a high prevalence in individuals of Maori or Pacific Island descent14 and patients appear to present with more severe disease (eg, acute corneal hydrops) at a younger age.15 Ethnicity data are not routinely acquired by NZNEB; however, census data demonstrate that between 1996 and 2013 the proportions of Maori and Pacific peoples have continually increased (15.4% to 15.6% and 6.1% to 7.8%, respectively).10 This suggests that the need for PK and DALK will probably remain significant in New Zealand.
Corneal cross-linking was widely introduced in New Zealand in 2007 and eventually, by halting disease progression, this is expected to reduce the number of keratoplasties performed for keratoconus. However, as reported in the DUSKS study in the UK, there may be a period of approximately a decade between diagnosis of keratoconus and progression to corneal transplantation.16 Thus, we would expect a lag phase between the introduction of corneal cross-linking and observation of its effect on keratoplasty rates. We believe this interval may be approximately 7–10 years in New Zealand, although we may be starting to observe a decline in keratoplasties for keratoconus, for example, comparing data for 2006–2010 and 2011–2015, there was a 25% increase in keratoplasties per se but only a 7% increase in first-time keratoplasties for keratoconus.17 Ultimately, we anticipate that the development of less invasive methods of keratoconus treatment like cross-linking and contact lenses will allow corneal transplantation to be deferred or entirely avoided in most cases.7 ,17
There was a marked reduction in the absolute and relative number of transplants performed for keratitis, trauma and corneal dystrophies (non-Fuchs') over the study period, with many possible explanations. Advances in contact lens technology and availability may allow visual rehabilitation for scarred and irregular corneas that otherwise would have required transplantation.18 Improved laboratory diagnostics and availability of new-generation antibiotics for treatment and prophylaxis may have reduced the morbidity of infective keratitis.19 Moreover, increasing knowledge of the relatively poor prognosis of keratoplasties performed for infective keratitis may have reduced the number of keratoplasties performed for this indication.20 The use of excimer laser photo-therapeutic keratectomy to treat anterior corneal dystrophies may have reduced the need for keratoplasty for some patients.21 It is also conceivable that increased public awareness of ocular trauma and prevention through protective eyewear and other measures may have reduced the overall incidence of ocular trauma during the study period.
With regard to the types of corneal transplantation in New Zealand, PK remains the most common type of transplantation for keratoconus.17 In Italy, between 2002 and 2008, the leading technique was also PK (82%), which was performed for the majority of keratoconus, regraft and PBK cases.6 In the USA, while PK is also the most common type of keratoplasty performed for keratoconus (89% in 2014), EK has become the most common type of transplantation overall—largely due to a higher proportion of FECD.2
PK is a well-established technique that avoids difficulties associated with the learning curves of DALK and EK, including those faced by the surgeons as well as the eye banks preparing precut tissue.5 ,17 On the other hand, lamellar keratoplasty and EK provide potential advantages over PK, such as faster visual rehabilitation, less astigmatism, reduced risk of rejection and shorter period of corticosteroid use.5 ,17 Reports on visual acuity outcomes are more mixed.5 ,17 ,22–25 After an initial 3-year growth in DALK numbers, the ratio of DALK to PK has been steady around 1:6. This is comparable to the USA where PK is much more popular than DALK. However, the rate of DALK in New Zealand is much lower than other Western countries where DALK has surpassed PK as the preferred technique for keratoconus.26 ,27 This may be due to differences in severity of disease in different countries and the surgeons' preference in techniques.
Despite the learning curves, there has been a rapid uptake of EK for its relative indications.2 In New Zealand, DSAEK has come to account for a third of all keratoplasties over a short period of 8 years. Park et al2 reported the annual number of EK exceeding that of PK from 2011 with the number of DMEK doubling every year in the USA. Yet, the total number of keratoplasties has remained steady, unlike New Zealand and other countries where there has been an overall increase in keratoplasty procedures.2 ,4 ,7 ,8 It may be that these countries have significantly different proportions of indications and that newer techniques such as DMEK are yet to be propagated as extensively as in the USA. In New Zealand, DMEK was introduced recently (2015) and we already foresee a greater uptake.
Limitations of the data in this study include having more than one indication listed for some cases and the dependence on the accuracy of surgeons' documentation. Also, some tissue for transplantation has been sourced from other eye banks overseas, although this number would be expected to represent a small percentage of the total keratoplasties performed in New Zealand. Indeed, a survey of New Zealand ophthalmologists reported that only 44 donor corneas (12.1% of total donor corneas) were directly imported from the USA without involving the NZNEB for the period 2013—likely the highest rate during the 25-year period studied.28
In summary, over the last 25 years, there have been considerable shifts in indications and techniques of corneal transplantation in New Zealand, some of which mirror other developed countries. However, of distinct note in New Zealand, keratoconus remains the leading indication for corneal transplantation and, accordingly, PK is the leading type of corneal transplantation. With the increasing uptake of lamellar keratoplasty and EK, and advances in more conservative methods of ophthalmic treatment such as collagen cross-linking, we anticipate a further substantial change in the next 10 years of corneal transplantation, which may yet reveal unique trends in New Zealand.
Acknowledgments
The authors acknowledge Associate Professor Gillian Clover, PhD, FRACO, founder and first scientific director of the NZNEB; trustees, past and present managers, transplant coordinators, and the scientific staff of the NZNEB who have contributed to and/or supported the clinical and scientific aspects of the NZNEB over the last 25 years. The authors also thank the ophthalmologists of New Zealand for their support and participation in the research and clinical activities of the NZNEB.
References
Footnotes
Contributors BZK, JJM: conception, data analysis/interpretation, drafting and critical revision of manuscript; NHB: data acquisition/analysis/interpretation, critical revision of manuscript; SLM, HCT, DGP, TS: data acquisition, critical revision of manuscript; CNJM: conception, data acquisition/analysis/interpretation, drafting and critical revision of manuscript. All authors have given final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding BZK was funded by an unrestricted fellowship from the University of Auckland.
Disclaimer The funder did not have any role in the study design; in the collection, analysis and interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.