Article Text

Abstract
Purpose To determine prevalence of refractive (RA), corneal (CA) and internal astigmatism (IA), including variation with gender and spherical equivalent refraction (SE), in a population of 12-year-old Chinese children.
Methods A total of 1783 students with a mean age of 12.7 years (range 10.0–15.6 years) completed comprehensive eye examinations in the Anyang Childhood Eye Study. Data of cycloplegic refraction and corneal curvature were analysed.
Results Prevalences of RA, CA and IA ≥1.0 D were 17.4% (95%CI 15.6% to 19.2%), 52.8% (50.5% to 55.1%)%) and 20.9% (19.0% to 22.8%), respectively. With different limits of astigmatism axes classification, including ±15°, ±20° and ±30°, RA and CA axes were mainly ‘with-the-rule’ (WTR) (ie, correcting axis of negative cylinders at or near 180°), while those for IA axes were mainly ‘against-the-rule’ (ATR) (ie, correcting axis of negative cylinders at or near 90°). RA was not different between the genders, but girls had higher prevalence and greater means of CA and IA. RA and CA increased in students with higher ametropia (more myopia and more hyperopia) and were the highest in a high myopic group (SE≤−6 D), while IA was stable across refraction groups. Children with RA higher than 0.50 D were more likely to have lens corrections (51%, 57%, 61% and 69% for magnitudes of ≥0.50 D, ≥0.75 D, ≥1.0 D and ≥1.5 D, respectively).
Conclusions Prevalence of RA in the Chinese 12-year-old children was relatively high compared with other studies. RA and CA had mainly ‘WTR’ astigmatism, while IA was mainly ATR and partially compensated for CA. Girls had greater means and prevalences of CA and IA than did boys. Both RA and CA, but not IA, increased with refractive errors away from emmetropia.
- astigmatism
- epidemiology
- Chinese children
- prevalence
Statistics from Altmetric.com
Introduction
Astigmatism is a common eye condition in children as well as in adults.1 Total, or refractive astigmatism (RA) is a combination of a corneal component (CA) and an internal astigmatism component arising from the lens (IA). In practice, the first two are determined independently and IA is taken as the difference between them. Knowledge of the distribution of the astigmatism components may be important for understanding the development and progression of the eye’s refraction.2 3
There are several epidemiological reports on astigmatism in school-age children across the world, with prevalence varying greatly according to population characteristics.4–8 Astigmatism of Chinese students has been reported in several surveys.9–11 The RESC (Refractive Error Study in Children) surveys in children aged 5–15 years reported 26% and 10% astigmatism (≥0.75 D) with cycloplegic autorefraction in rural areas in Beijing and urban areas in Guangzhou, respectively, and corresponding values for cycloplegic retinoscopy of 21% and 14%. However, there is no detailed information on astigmatism of Chinese children, especially for the corneal and internal components.
Axes of astigmatism distributions have also been reported, with ‘with-the-rule’ (WTR) (ie, correcting axis of negative cylinders at or near 180°) usually being predominant for RA10 12 13 although an Australian study of 12 year students found most children had ‘against-the-rule’ (ATR) astigmatism (correcting axis of negative cylinders at or near 90°).4 14 Additionally, some studies found RA was higher in females than in males,15 16 while others reported no gender variation of RA.9 17 18 Some studies have also demonstrated significant relations between astigmatism severity and the spherical error.19 20 In Chinese students with a very high prevalence of refractive error, especially myopia,21 it is necessary to investigate the association between astigmatism and spherical error in order to understand the functional significance of astigmatism.
The Anyang Childhood Eye Study (ACES) is a school-based study of eye conditions in Anyang city, a small prefectural-level city in central China with a relatively stable demographic structure.22 In the present study, we aimed to report the prevalence and distribution of astigmatism and its components in a population of 12-year-old Chinese children, including the distribution of astigmatism axes and associations of astigmatism with gender and spherical equivalent refraction (SE).
Methods
Study population
The ACES has studied the prevalence, incidence and progression of myopia among Chinese children in urban areas of Anyang, Henan Province, Central China. Methodology details have been given elsewhere.22 Briefly, stratified cluster sampling was used to recruit children from schools across Anyang city. All the 21 primary and 11 junior high schools in Anyang were stratified into three levels based on the quality evaluation of local government. Finally, 3112 grade 1 students of 11 primary schools and 2363 grade 7 students of 4 junior high schools were randomly sampled. These children, consisting of 6-year-olds and 12-year-olds, are being followed up annually for 5 and 3 years, respectively. The survey used a comprehensive eye examination to collect data and was approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University. All procedures adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from at least one parent of each child as well as verbal assent from all children. The response rate was 95.9% and 2267 grade 7 students were examined at baseline.
Eye examinations
The IOLMaster 500 (Carl Zeiss, Meditec AG Jena, Germany) was used to measure anterior corneal curvature. Corneal power was calculated by multiplying the curvature by 0.3375. Three consistent measurements were obtained and the averages were used for analysis.22
One drop of topical anaesthetic agent (Alcaine, Alcon) was instilled to alleviate discomfort, followed by 2 drops of 1% cyclopentolate (Alcon) and 1 drop of Mydrin P (Santen, Japan), administered 5 min apart, to induce cycloplegia. Thirty minutes after the last drop, a third drop of cyclopentolate was instilled if the pupillary light reflex was still present or the pupil size was less than 6.0 mm. Three measurements were taken with a HRK-7000A autorefractor (Huvitz, Korea) and the mean was used for analysis.22
Definitions
Refraction was analysed as spherical equivalent (SE), calculated as sphere +cylinder/2. Myopia and hyperopia were defined as SE of ≤ −0.50 D and ≥+0.5 D, respectively. Refraction was stratified into six groups as follows: high myopia (SE≤−6 D), moderate myopia (−6.0 D<SE≤−3.0 D), low myopia (−3 D<SE≤−0.5 D), emmetropia (−0.5 D<SE<+0.5 D), low hyperopia (+0.5 D≤SE<+2 D) and moderate and high hyperopia (SE≥+2 D).
Astigmatism was expressed in negative cylinder notation. The total astigmatism RA of the eye was given by cycloplegic autorefraction. The CA was the difference between the corneal powers of the principal meridians, with the cylindrical axis corresponding to the meridian of minimum power. RA and CA were converted to power vector notation using:
J 0(RA) = −(RA/2)×cos(2αRA), J 45(RA) = −(RA/2)/2×sin(2αRA)
J 0(CA) = −(CA/2)×cos(2αCA), J 45(CA) = −(CA/2)/2×sin(2αCA) where J 0 and J 45 are the horizontal/vertical and oblique components of astigmatism, respectively, and α is the cylinder axis. The components of IA were determined as
J 0(IA) = J 0(RA) – J 0(CA), J 45(IA) = J 45(RA) – J 45(CA)
The IA components were recombined to give IA and its axis αIA as:
IA = –2√[J 0(IA) 2+ J 45(IA) 2]
αIA = atan(J 45(IA)/J 0(IA))
with appropriate corrections to keep αIA in the range 0°−180°.23
While astigmatism was determined in negative cylinder format, sign is ignored in what follows. Prevalences of astigmatism≥0.5 D, ≥0.75 D, ≥1.0 D and ≥1.5 D were determined. Astigmatism type was classified using different angular classification limits of WTR and ATR astigmatism of ±15°, ±20° and ±30°.
Statistical analysis
There were high correlations between right and left eyes for RA and CA (r=0.70 and 0.71, respectively, for absolute values) and moderate correlation between right and left eyes for IA (r=0.4 for absolute values). Given these correlations and because distributions were similar for right and left eyes, especially for IA (online supplementary tables 1-3), data from right eyes only were presented. Statistical analysis was performed using SPSS V.17.0. For continuous variables and categorical variables, group differences were compared by Student’s t-test and the χ2 test, respectively. Prevalence estimates and their 95% CIs were presented. Associations of astigmatism with refraction were assessed by Pearson correlation. The threshold for statistical significance was set at p<0.05.
Supplemental material
Results
Characteristics of the study population
A total of 1783 students were included for analysis with available data of all items. Of them, 49.5% were boys. The mean age was 12.7 years (range 10.0 to 15.6 years) and 71% students were 12 years old (between 12.0 and 13.0 years, SD for boys and girls were 0.51 and 0.49). Mean cycloplegic spherical equivalent was −1.57 D (range −9.88 D to +13.38 D). Prevalences of myopia, emmetropia and hyperopia were 67%, 17% and 16%, respectively. Four hundred and eighty-four students were excluded due to missing data of cycloplegic refraction or IOLMaster. There was no significant difference in characteristics between those included and excluded students.
Prevalence of astigmatism
Mean RA, CA and IA were 0.57 D, 1.11 D and 0.72 D, respectively. Distributions of RA, CA, IA are given in figure 1. The highest prevalence for RA was between 0 and 0.5 D (45%), while those for CA and IA were between 0.5 D and 1.0 D (34% and 49%, respectively).

Distributions of RA, CA and IA. CA, corneal astigmatism; IA, internal astigmatism; RA, refractive astigmatism.
Table 1 shows the prevalences for RA, CA and IA at different magnitudes, and the prevalences of lens correction for children with astigmatism. Prevalences of RA and IA were lower than for CA. For example, prevalences for ≥1.0 D astigmatism with RA, CA and IA were 17.4% (95% CI 15.6% to 19.2%), 52.8% (50.5% to 55.1%)%) and 20.9% (19.0% to 22.8%), respectively, and corresponding prevalences for ≥1.5 D were 6%, 20% and 3%. Children with RA higher than 0.50 D were more likely to have lens correction (57%, 61% and 69% for astigmatism magnitudes of ≥0.75 D, ≥1.0 D and ≥1.5 D, respectively). Single spectacles were mostly often used for correction of astigmatism, followed by bifocal lenses and progressive spectacles. Contact lenses was not used for any children.
Prevalences of RA, CA and IA at different magnitudes as well as the condition of children with or without lens correction
Table 1 shows also gender-specific prevalences. There was no statistical difference for prevalence of RA between males and females at any criteria (>0.2). For CA and IA, except for astigmatism≥1.5 D, prevalences in girls were higher than in boys by 4%–7%.
Table 2 shows means of RA, CA and IA stratified by gender and SE group. Consistent with table 1, girls had significantly higher values of CA and IA than boys (mean difference 0.06 D for both CA and IA). The prevalence of RA≥1 D was 19% for myopes, 12% for emmetropes and 15% for hyperopes.
Mean RA, CA and IA by gender and refraction group
Relationship between astigmatism and spherical equivalent refraction
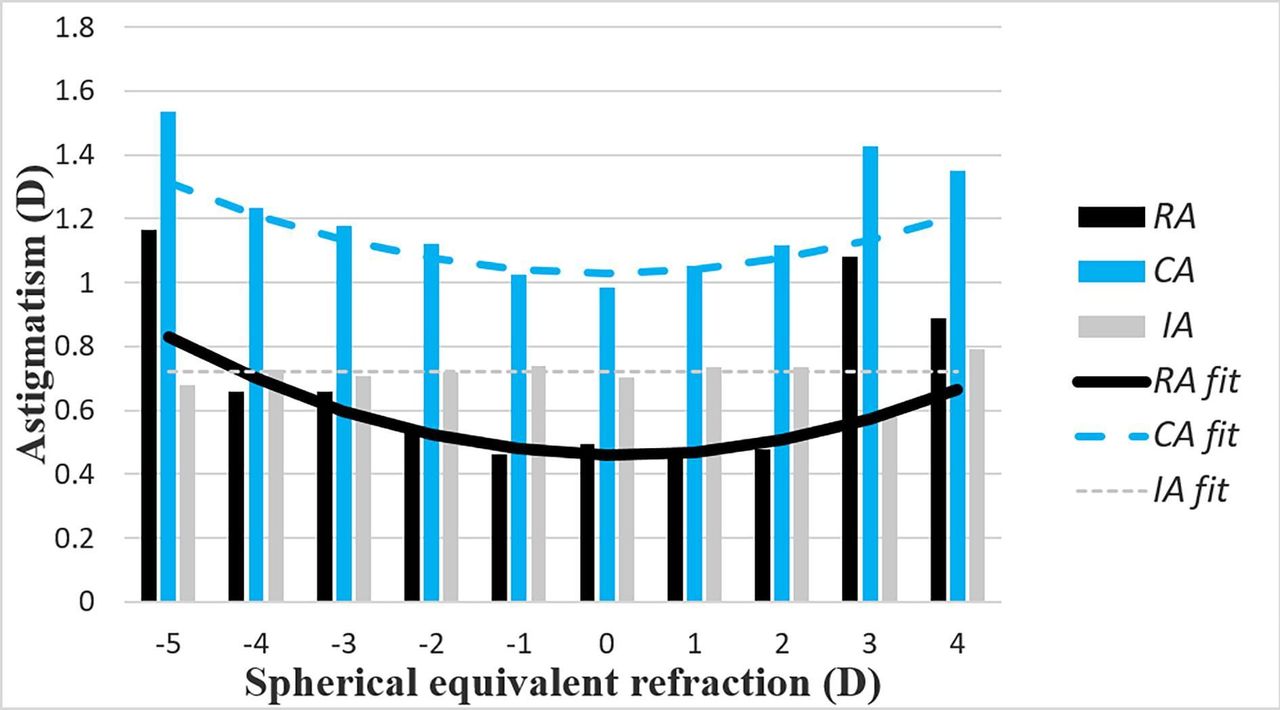
As shown in figure 2 and table 2, the distributions of RA, CA and IA varied with SE. RA and CA increased away from emmetropia in both myopic and hyperopic directions, while IA was little affected by refractive group. The differences in both RA and CA between the emmetropic group and other groups, except for low myopes and low hyperopes, were significant. For RA, the differences were 0.83 D (high myopia), 0.24 D (moderate myopia) and 0.52 D (moderate/high hyperopia). Corresponding differences for CA were 0.52 D, 0.19 D and 0.34 D.

{kind=link}
{kind=link}
Mean RA, CA and IA as a function of SE. Fits to the data are: RA =+0.0139(SE – 0.155)2 + 0.46, R2=0.10; CA =+0.0113SE2+1.03, R2=0.05; IA =+0.72. CA, corneal astigmatism; IA, internal astigmatism; RA, refractive astigmatism; SE, spherical equivalent refraction.
RA and CA were correlated significantly with SE according to quadratic relationships (p<0.001), but IA was not correlated significantly with SE (figure 2). Additionally, RA and CA, but not IA, were also correlated significantly with the spherical refraction (r=0.106, p=0.00; r=0.061, p=0.01; r=−0.017, p=0.47), respectively.
Distribution of astigmatism axis
Table 3 shows distributions of astigmatism axes with different definitions of angular limits for WTR and ATR types. With a classification limit of astigmatism axes of ±15°, 53%, 7%, 31% and 9% of students had WTR, ATR, oblique astigmatism and no measurable astigmatism (ie, <0.12 D), respectively. In students with measurable astigmatism (1633), the per cent were 58% WTR, 8.0% ATR and 34% oblique astigmatism. CA was predominantly WTR. IA was predominantly ATR followed by oblique astigmatism. With the classification of ±20° and ±30°, obviously there are higher WTR and ATR percentages and lower oblique percentages for all three astigmatism components.
Prevalences of RA, CA and IA by gender and different classification with axes
There were no gender differences in prevalences of WTR, ATR and oblique astigmatism for any of RA, CA and IA.
Discussion
Being an important refractive anomaly, astigmatism has been described in different groups of children (table 4). We have reported the prevalences of total, or refractive, astigmatism and its corneal and internal components in 12-year-old, grade 7 school children in Central China. Prevalences of RA, CA and IA were 17%, 53% and 21% at a 1.0 D criterion and means of RA, CA and IA were 0.57 D, 1.11 D and 0.72 D, respectively. Nearly half of the children had astigmatism less than 0.5 D, while CA and IA had peak prevalence between 0.5 D and 1.0 D.
Reports of prevalence of astigmatism in different countries
The prevalence of RA≥0.75 D (32%) was higher than those reported in rural Southern China (25.3%),24 China Shunyi (9.5%),25 Chile (19%),26 India (5%),15 16 Iran5 and Australia,4 but was lower than found in urban Southern China (43%).9 The prevalence of RA≥1.0 D (17%) was higher than that reported in Australia (7%),4 similar to those reported in Singapore (19%)17 and Northern Ireland (20%)6 and lower than that in Taiwan (27.9%).12 In the Australian Sydney Myopia Study,4 racial background sampling showed that the East Asian background population had the highest prevalence of RA, followed by South Asians and then Caucasians. The reason may be that the Asian people have tight eyelids and narrow palpebral apertures.24 The prevalence of RA≥1.5 D (5.9%%) was similar to that of Sweden,25 but lower than that reported in Mexico (9.5%).26
RA and CA increased in both myopic and hyperopic directions and there were significant associations between mean RA and CA with SE. Other studies have also found relationships between SE and astigmatism,4 5 8 19 27 particularly for high myopia.28 In the Australia children,4 the highest RA and CA values were also found in a high myopic group. This suggests a connection between myopia and astigmatism, but it is not clear whether children developed higher astigmatism before or after developing high refractive error: this requires longitudinal follow-up.
We observed gender difference in the means and prevalences of CA and IA, with girls having higher astigmatism than boys, but not in RA (table 1). This is consistent with the Huynh et al study,4 while some other studies reported higher prevalence of RA in girls than in boys.9 15 16 28 29 However, the differences (4%–7% for prevalence and 0.06 D for mean value) were small and are probably not clinically relevant.
Since the axes ranges of the astigmatism types affect the percentages, we made analysis based on three angular limit classifications of ±15°, ±20° and ±30° for WTR and ATR. The axes of astigmatism were not evenly distributed between the astigmatism types. For the ±15° classification, WTR was dominant for RA, confirming previous studies in Xiamen,10 Singapore,13 Taiwan12 and Hong Kong.30 In the Australia study,4 RA was predominantly WTR and ATR (40% and 44%, respectively). For the ±30° classification, the WTR (76%) and ATR (13%) were higher and lower, respectively, than an Iran study in 7–15 years students with respective percentages of 46% and 48%.5
The partial compensation of the CA by IA is clearly shown in our data and has been reported previously.4 6 27 We also found IA values, different from RA and CA, were relatively stable across all refraction groups, which was consistent with that of Australia children31 and suggests that IA appears to be unaffected by refraction. However, one recent study on the IA in myopes and non-myopes using vector analysis found that IA may reduce CA’s contribution to RA in eyes with low amounts of CA, but IA is not a constant, and the compensation of IA needs to be further confirmed.32
There was a limitation in the present study in that it was a cross-sectional study, and longitudinal analysis is necessary to clarify the relation between astigmatism and myopia development in children.
In summary, in a large cohort study of myopia in Chinese children, we found high prevalence of ocular astigmatism, with RA and CA mainly WTR and IA mainly ATR. Girls had greater CA and IA than boys. RA and CA, but not IA, increased away from emmetropia in both myopic and hyperopic directions.
Acknowledgments
The authors thank the support from the Anyang city government for helping to organise the survey.
References
Footnotes
HL and S-ML contributed equally.
Contributors NW had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: S-ML, NW, L-RL, PM, S-YZ. Acquisition, analysis or interpretation of data: HL, SML, DAA, M-TK, J-HG, RY, Y-WB. Drafting of the manuscript: HL, S-ML, DAA. Critical revision of the manuscript for important intellectual content: All authors. Administrative, technical or material support: NW, L-RL. Study supervision: NW.
Funding The ACES was supported by the capital health research and development of special (2016-4-2056), the Ministry of Science and Technology, the Major State Basic Research Development Program of China (‘973’ Program, 2011CB504601) of the Ministry of Science and Technology, the Major International (Regional) Joint Research Project of the National Natural Science Foundation of China (81120108007), the National Natural Science Foundation of China (81300797) and Beijing Nova Program (Z121107002512055).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee of Beijing Tongren Hospital, Capital Medical University.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance