Article Text

Abstract
Background/aims During the last decade, improved neonatal care has resulted in increased survival of the most immature infants and improved health of more mature infants. We hypothesise that this has affected incidence and treatment of retinopathy of prematurity (ROP), enabling guidelines for screening to be modified.
Methods In Sweden, all infants with gestational age (GA) at birth ≤30 weeks are screened for ROP. Results are registered in a web-based register, Swedish National ROP Register, with a coverage rate of 97%. Incidence of ROP and frequency of treatment, aspects on natural course of ROP and number of examinations, are calculated in relation to GA at birth in infants born during 2008–2017.
Results Of 7249 infants, 31.9% (2310) had ROP and 6.1% (440) were treated. No infant with GA 30 weeks was treated. Incidence of ROP remained similar, but frequency of treatment increased (p=0.023). Over time, GA and birth weight were reduced in infants with ROP and with treated ROP. In the most immature infants, postmenstrual age was lower and postnatal age was higher when any ROP and stage 3 ROP were first detected (p<0.001). At treatment, postmenstrual but not postnatal age of the infant was associated with GA (p<0.001). During the 10-year period, 46 038 examinations were performed.
Conclusion Modification of Swedish guidelines is proposed, including only infants with a GA of <30 weeks and postponing the first examination with 1 week in infants with GA 26–29 weeks. This would spare many infants from stressful examinations and reduce eye examinations with at least 20%.
- retina
- child health (paediatrics)
- epidemiology
Statistics from Altmetric.com
Introduction
Retinopathy of prematurity (ROP) is a blinding disease globally.1 With the help of ophthalmological screening of infants at risk, infants with treatment-requiring ROP can be identified and timely and properly treated. Such screening, however, is costly for the society and stressful for the infants. Screening routines, therefore, ought to be continuously evaluated and if possible also modified, to reduce the number of examinations in infants with low risk of treatment-requiring ROP and to reduce the expenses of ophthalmological care. There is an ongoing discussion regarding optimising the ROP screening. In the UK, tightening the guidelines is calculated to reduce the number of screened infants with around 11%–15%.2 Various predictive models have been constructed to optimise the ROP screening programme.3–6
Guidelines for ROP screening vary between countries. In Sweden, national guidelines are based on population studies, the first one resulting in a recommendation to include infants with a gestational age (GA) at birth of less than 33 weeks,7 the second one less than 32-week GA8 and the third one less than 31-week GA.9 With the help of 10-year data from a Swedish National ROP Register (SWEDROP), the present study aims to evaluate if further modifications of the national guidelines for ROP screening can be undertaken. The early course of ROP and its different stages will be analysed and trends over time regarding ROP and treatment will be explored in relation to GA at birth.
Methods
Present guidelines for ROP screening in Sweden include infants with a GA less than 31 weeks. In addition, for safety reasons, neonatologists are recommended to refer also more mature and severely diseased infants. The results of all infants who are born and screened in our country are registered in the Swedish register, SWEDROP. Eye examinations start at 5-week postnatal age (PNA) or at a postmenstrual age (PMA) of 31 weeks, whichever comes latest. ROP is classified according to international recommendations10 and treatment for ROP follows the Early Treatment for Retinopathy of Prematurity criteria.11
Previous studies have presented results of SWEDROP data from the years 2008–2015.9 12–14 The present study is a 10-year report including the years 2008–2017. During this period, guidelines for screening were changed in July 2012 from GA <32 weeks to GA <31 weeks. For comparison of incidences of ROP and frequencies of treatment over time, the present study includes only infants with a GA of less than 31 weeks in the analyses.
The coverage rate of SWEDROP is calculated by comparison with the Swedish Neonatal Quality Register (SNQ). During the years 2008–2017, the coverage rate of the infants fullfilling the national screening criteria (GA <32 weeks during the years 2010–2012, and <31 weeks during the years 2013–2017) was 97.6% (range 96.2%–99.3%). Information on GA and birth weight (BW) was collected from the SNQ register.
Statistical methods
Data are primarily analysed using descriptive statistics, where continuous variables are described as median and range and categorical as number and percentage. In order to explore trends, both in terms of calendar year and GA, linear regression models have been used for continuous variables and logistic regression models for dichotomous variables. The results from the regression models are expressed as the slope (for linear regression) and OR (for logistic regression) related to a one-unit increase of the dependant variable, with 95% CIs.
All statistical analyses were performed using R V.3.5.0.
Results
During the period 2008–2017, 8473 infants had been screened for ROP and registered in SWEDROP. Of these infants, 7249 had a GA of <31 weeks, constituting the present study group. In this group, there were 3951 (54.5%) boys, 3298 (45.5%) girls and one infant with unknown gender. Median GA of the study group was 28.3 weeks (range 21.6–30.6) and median BW was 1109.5 g (range 307–3245); see table 1.
Background data, incidence of retinopathy of prematurity (ROP) and frequency of treatment in the study population of infants with gestational age (GA) ≤30 weeks
Overall, 2310 (31.9%) infants in the study group had some stage of ROP and 440 (6.1%) infants were treated for ROP (table 1). Type 1 ROP in at least one of the eyes was found in 87% (383/440) of the treated infants. Among the 1224 infants with a GA above 30 weeks, 46 infants had some stage of ROP, including 5 with ROP stage 3. Four of the latter children were severely ill and therefore referred for screening and one previously described14 extremely ill infant was treated for the ROP.
The total incidence of ROP remained similar during the study period but, over time, infants with ROP had lower GA and BW (GA slope −0.03, CI −0.06 to 0.00; p=0.030/BW slope – 5.14, CI −8.95 to −1.32; p=0.008). For incidence of ROP in infants with different GA at birth, see table 2. Of treated infants, 251 (57%) were boys and 189 (43.%) girls. Median GA and BW of the treated infants were 24.3 weeks (range 21.6–29.5) and 647 g (range 370–1700), respectively. Regarding frequency of treatment in the different gestational weeks, see table 2. The frequency of infants treated for ROP increased during the study period (OR 1.04, CI 1.01 to 1.08; p=0.023) and, over time, more immature infants and fewer with higher GA and BW were treated for ROP (GA slope – 0.07, CI −0.11 to −0.02; p=0.004/BW slope −8.53, CI −13.95 to −3.11; p=0.002); see figure 1A,B.
Incidence of retinopathy of prematurity (ROP) and frequency of treatment in relation to gestational age (GA)

(A) Annual mean gestational age (GA) (weeks) and (B) mean birth weight (grams) in the 440 treated infants during the study period.
Treatment was performed in 434 right and 433 left eyes. At the first treatment, 389 (89.6%) right eyes and 384 (88.7%) left eyes were treated with laser only. Anti-vascular endothelial growth factor (VEGF) injections alone were given in 44 (10.1%) right eyes (7 bevazicumab/37 ranizicumab) and 43 (9.9%) left eyes (5 bevazicumab/38 ranizicumab). Altogether, 76 infants were given anti-VEGF injections, as the only treatment or at retreatment in combination with laser and/or vitrectomy. Encircling bands were used in seven right eyes and eight left eyes and vitrectomies were performed in five right and nine left eyes.
Recurrence was noted in 199/773 (25.7%) of the eyes treated with laser only at the first treatment and retreatment was performed after mean 2.6/2.7 weeks (right/left eyes). Among eyes treated with anti-VEGF alone at the first treatment, there was a recurrence in 58/87 (66.7%) of the eyes (50% in eyes treated with bevazicumab and 68.4% in eyes treated with ranizicumab). Retreatment was performed after mean 8.5/8.6 weeks (right/left eyes) (11.5/12.8 weeks after bevazicumab and 8.3/9.0 weeks after ranizicumab).
Chronological aspects
PNA and PMA at detection of ROP, detection of ROP stage 3 and first treatment in infants of the total study group as well as in relation to GA are illustrated in table 3.
Postnatal (PNA) and postmenstrual age (PMA) at detection of retinopathy of prematurity (ROP), ROP stage 3 and first treatment, time from detected ROP to treatment and number of examinations in relation to gestational age (GA)
At the first screening examination, 404 (5.6%) infants already had some stage of ROP, see table 4, and were excluded from analyses of age PNA and PMA at detection of ROP. GA and BW were significantly lower in these 404 infants as compared with the rest of the study group (n=6845; p<0.001). In the remaining 1906 infants who developed ROP, median PNA and PMA (weeks) at detection of ROP in at least one of the eyes were 9.0 weeks (range 4.1–27) and 34.9 weeks (range 29.4–51.3). The first treatment was performed at a median PNA of 12.6 weeks (range 7–63.1) and PMA of 36.9 weeks (range 32.1–87.3).
Gestational age (GA), birth weight (BW), stage of retinopathy of prematurity (ROP) at first examination, final stage of ROP and treatment in 404 infants with ROP in at least one eye at the first examination
PMAs were lower and PNAs higher at detection of first ROP (PMA slope −0.46, CI −0.51 to −0.41; p<0.001/PNA slope 0.53; CI 0.48 to 0.58; p<0.001) and at detected ROP stage 3 in infants with the lower GAs (PMA slope −0.25, CI −0.37 to −0.12; p<0.001/PNA slope 0.74; CI 0.61 to 0.87; p<0.001). Regarding age at treatment, only PMA of the infants was associated with GA (slope 0.92, CI 0.74 to 1.11; p<0.001).
Time of progression from first detected ROP to first treatment was longer in infants with the highest GAs (slope 2.93; CI 1.53 to 4.32; p<0.001); see table 3.
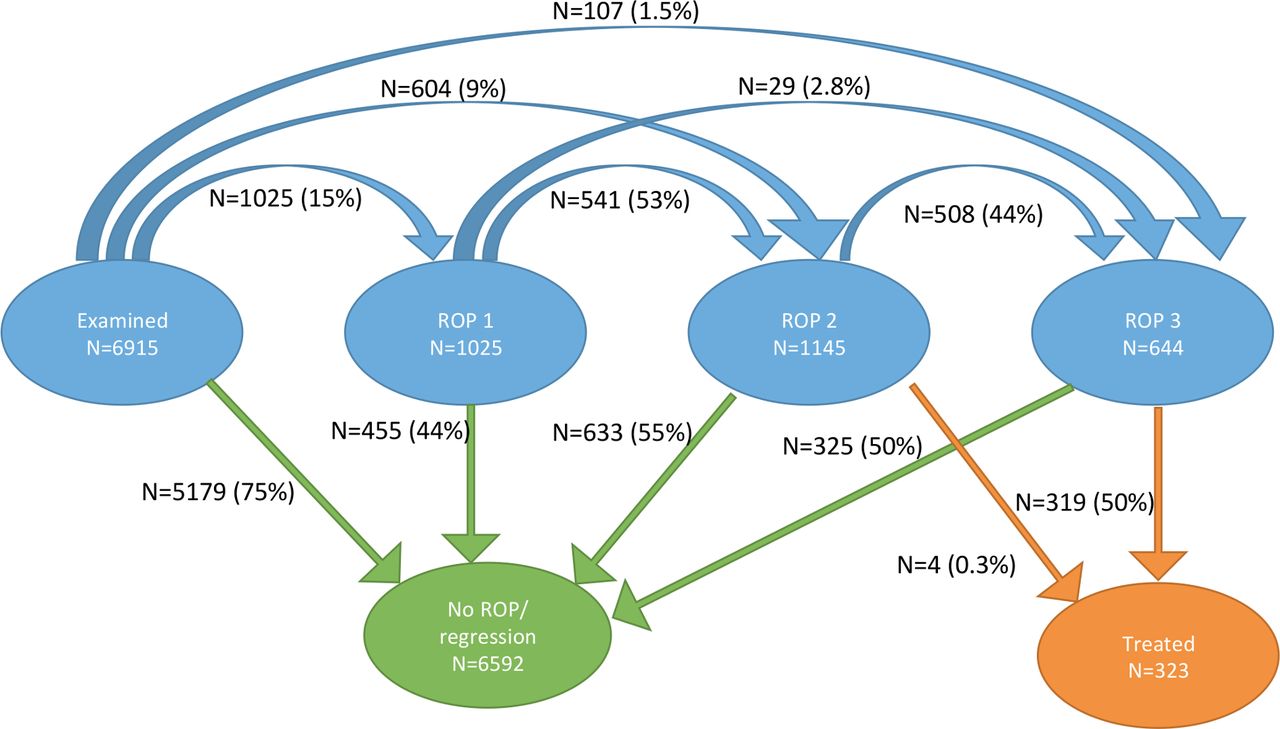
The course of ROP (ROP stages 1–3) in the worst eyes (or right eyes if there were similar stages of ROP in both eyes) of the infants, including regression and progression as well as progression to requirement of treatment, is illustrated in figure 2. For this calculation, eyes that already had some stage of ROP at the first examination, as well as eyes with missing data, have been excluded.

Flow chart showing the sequence course of retinopathy of prematurity (ROP), including regression and progression to treatment, in the worst eyes (or right eye if similar stages right/left eyes) of the infants in the study group. Infants with ROP in the worst eye at first examination or with missing data were excluded from the analysis.
Screening aspects
Overall, 46 038 eye examinations had been performed in 7249 infants during the 10-year period (26 infants lacked information on number of examinations). Median number of examinations per infant were 4 (range 1–42). The total number of examinations in relation to GA at birth is presented in table 2. Median PNA at first examination was 5.4 weeks (range 0.9–20.3) and median PMA was 33.7 weeks (range 25.9–50.4).
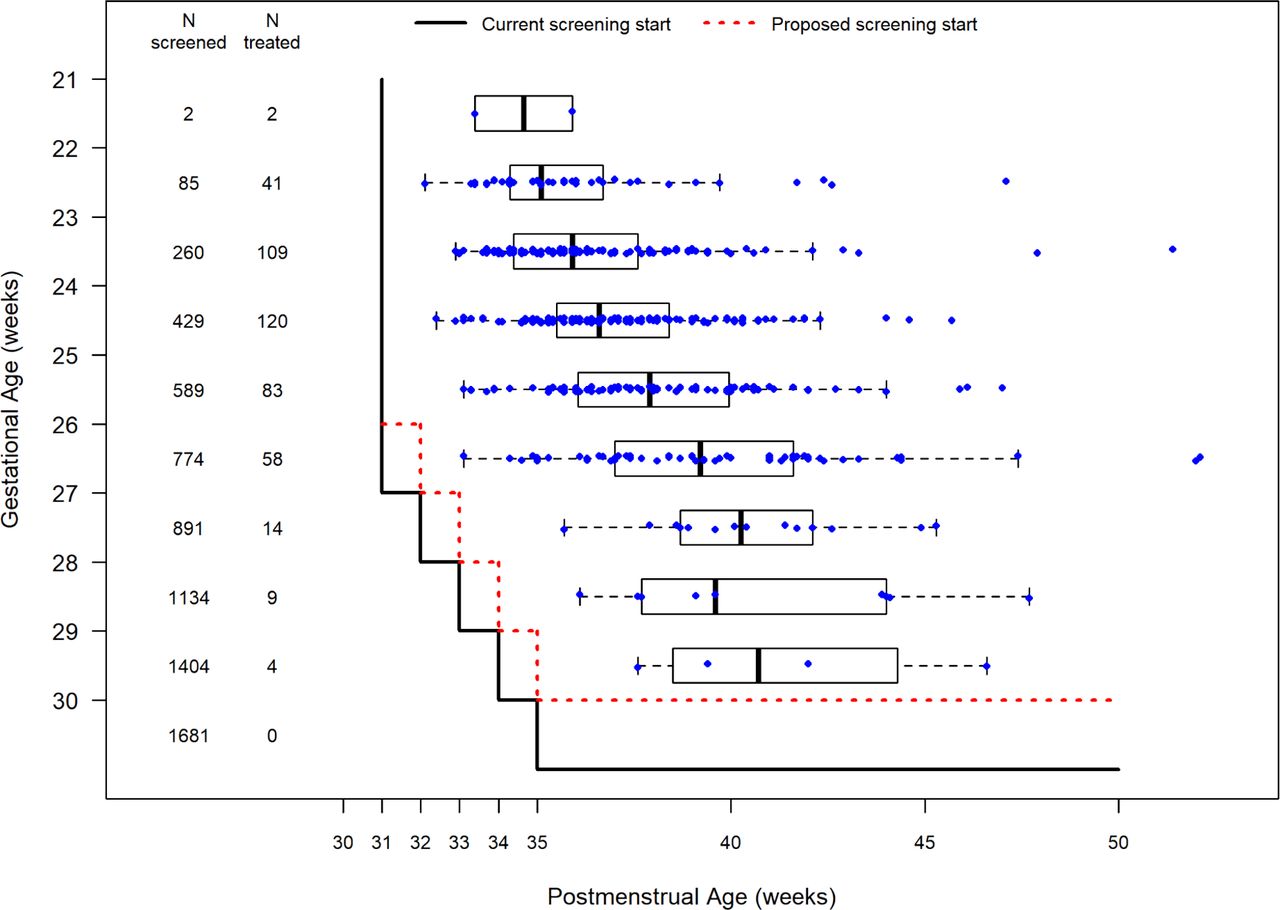
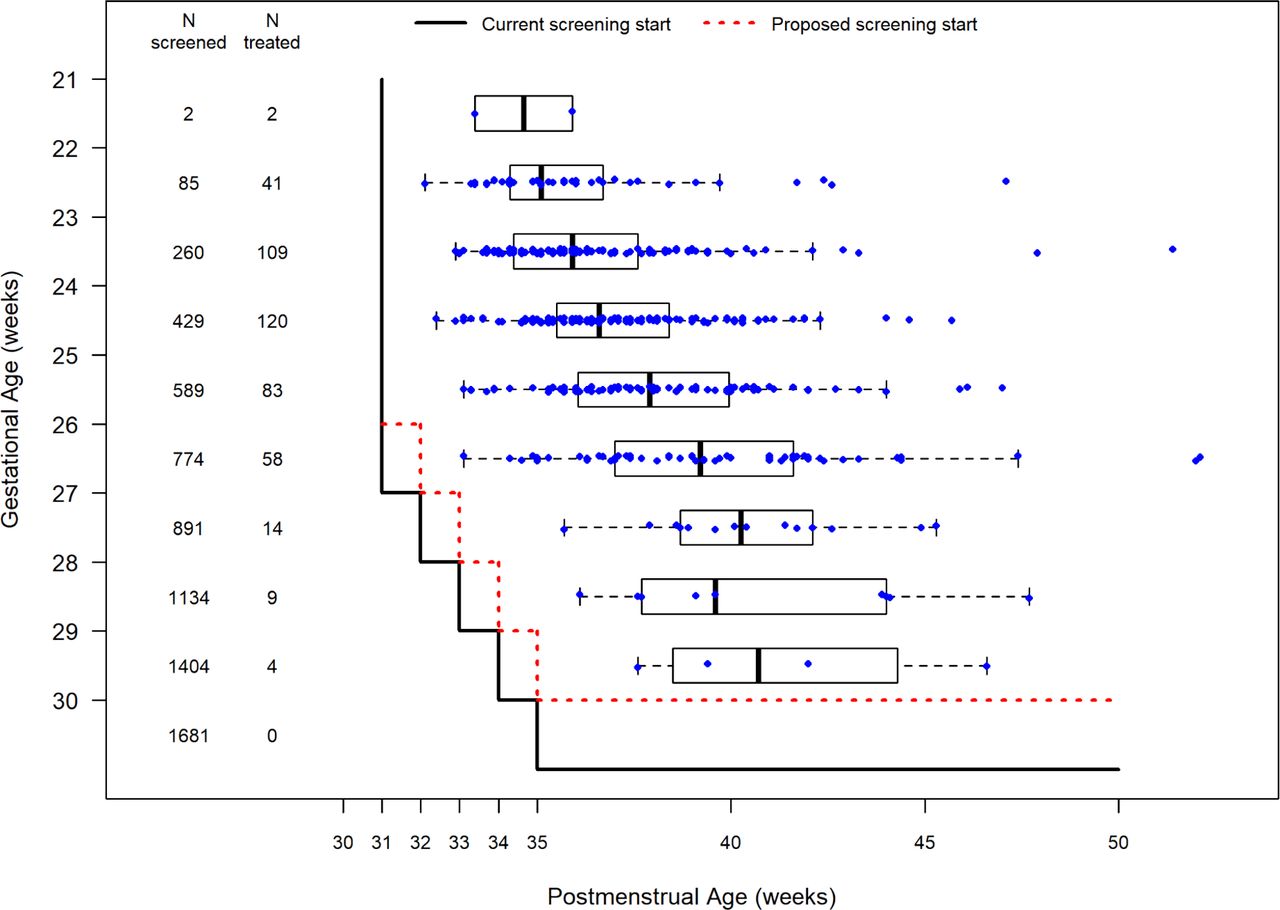
Current guidelines for screening in relation to GA at birth as well to PMA at treatment are illustrated in figure 3. At present, screening is started at PMA 31 weeks in infants with PMA 26 weeks or less and at 5-week PNA in infants with higher GA. Lowering the upper limit of screening inclusion by 1 week to GA <30 weeks would have reduced the number of screened infants with 1681 and the number of examinations with 5232 over the study period. Postponing the first examination by 1 week in infants born at GA 26–29 weeks would have reduced another 4203 examinations. Altogether, screening examinations would have been reduced with 9435/46 038 (20.5 %) examinations.
{kind=link}
{kind=link}
{kind=link}
Current and proposed start of screening in relation to gestational (weeks) and postmenstrual age (PMA) (weeks) at treatment. The distribution of PMA at treatment is presented both on individual level (dots) and in box plots. The box plots include the median (vertical line in the middle of the box) and 25th and 75th percentile (outer margins of the box). The whiskers are extends from the box to the most extreme value, which is no more than 1.5 times the interquartile distance from the box.
Discussion
The present study on 10-year data from the SWEDROP, with a high coverage of 97.6 %, shows a similar incidence of ROP over time and a significant increase in the frequency of treatment. Analyses of the early course of ROP and of PNA and PMAs at treatment indicate that modifications of the national guidelines for ROP screening can be undertaken.
During the study period, there was an increase in the treatment of more immature infants and a decrease in the treatment of those with higher GA, mirroring improved neonatal care, which increased the survival of very immature infants and improved the health of those with higher GA in the country during the last decade. It was recently demonstrated by Norman et al that 1-year survival among infants at 22–26 weeks’ GA without any major neonatal morbidity, including severe ROP, was significantly higher during 2014–2016 than during 2004–2007.15
We found an increase in the frequency of ROP treatment over time. As expected, the frequency of treatment-requiring ROP decreased in the less immature infants. No infant with a GA of 30 weeks, four infants with GA 29 weeks and nine infants with GA 28 weeks were treated for ROP during the 10-year study period. Apart from one extremely sick infant with a GA at birth of 27 weeks and BW 1700 g with Apgar 2-1-1, resuscitation with cardiac massage, pneumothorax, sepsis, oxygen for 114 days, there was no infant in the study group with a BW above 1250 g who had been treated for ROP.
Indication for treatment, that is, type 1 ROP, was fulfilled in at least one eye in 87% of the treated infants, which accords with findings in the American G-ROP study,16 but is higher than in a recent British study.17 The majority of infants were treated with laser, but injections with anti-VEGF were given as primary treatment in 10% of the infants, thus according with the British study.17 Reassuringly, the annual frequency of anti-VEGF treatments remained similar at the end of the study period. In accordance with the British study, retreatment frequency was higher in infants treated with anti-VEGF (67%) than with laser (26%), emphasising the challenge of follow-up in these infants.17
Analyses of chronological aspects and early course of ROP and its different stages in relation to GA at birth are helpful when giving information to parents and neonatologists and provide basis for the evaluation of guidelines for ROP screening. In accordance with a previous Swedish study of extremely premature infants with GA of less than 27 weeks,18 the present study shows that PMA at first detection of ROP was lower in the most immature infants, who also had the fastest progression to the requirement of treatment, emphasising the importance of strict surveillance of these infants. However, regardless of GA at birth, no infant developed ROP stage 3 before a PMA of 30.7 weeks and no infant was treated before a PMA of 32.1 weeks, including four infants GA 26 and 27 with ROP 3 at their first examination; see table 4.
Based on the findings of this study, changes of Swedish guidelines for inclusion in ROP screening are proposed including infants with a GA of less than 30 weeks (GA ≤29 weeks + 6 days). During the 10-year period, such a change would have spared 1681/7249 (23%) of the infants from potentially stressful examinations and would have reduced the workload for ophthalmologists with 5232/46 038 (11%) eye examinations. Regarding start of screening, the first examination should as currently be performed at PMA 31 weeks in infants with the lowest GAs of 21–25 weeks, but is proposed to be postponed to PNA 6 weeks in infants with GAs 26 weeks or more. Although the infants born at GA 27–29 weeks were treated at later PMAs, as seen in figure 3, for safety reasons and for more congruent rules, we have chosen to give the same recommendations for all infants with a GA of 26 weeks or more. This would have spared 4203 infants from at least one examination. Altogether, the proposed changes of guidelines would have spared many infants from distressing eye examinations and reduced the screening examinations by at least 9435/46 038 (20.5%).
A missed case of severe ROP may lead to life-long blindness. Thus, screening must have a sensitivity of close to 100%. Regarding screening guidelines for ROP, outliers are inevitable, as mentioned by Binenbaum et al,6 but the number must be limited to the utmost. The already present recommendations to neonatologists to refer also more mature, but severely diseased infants, therefore remain important. During the 10-year study period, there was only one infant referred above screening limits, who was treated for ROP. That infant had a GA of 31 weeks and a BW of 1225 g and was extremely ill, as reported in a previous paper.14 Further, there were 10 infants with a GA of 30 weeks who had ROP stage 3; see table 3. Reassuringly, they seemed to have a mild type of ROP stage 3 since six of them had ROP stage 3 in only one eye and the remaining four had ROP stage 3 in zone 3. Regardless of screening limits, however, there always remains a risk of non-adherence to screening programme. In the present study, 24 infants had their first examination at PMA 40 weeks or more, of which 21 were born at a GA 29–30 weeks and two at 27-week GA, but none of them had ROP when examined. Another infant born at 23-week GA had its first examination at PMA 43 weeks. At that examination, the infant had ROP stage 2, which regressed spontaneously. Finally, in a recent Swedish study, based on population data, 11/17 (65%) of severe visual impairment due to ROP was considered avoidable.19 This clearly illustrates that modifications and improvements of the national screening guidelines have to be combined with continuous education and information of the current guidelines. To further improve the safety of screening guidelines, inclusion of predictive factors for ROP and visual dysfunction may be a way to go forward, which has previously been shown in several sophisticated calculated models and risk-adjusted studies3–6 20 21
Strengths and limitations
SWEDROP has a high coverage rate (97.6%) and by the help of personal identification numbers in Sweden, it is possible to identify infants moving around in the country during the neonatal period. Further, Sweden is a small country with a population of around 10 million and a rather equalised neonatal care throughout the country.15
The ROP register is based on prospectively collected data. Further, and as opposed to the recently updated American guidelines,22 the present recommendations for national guidelines for ROP screening are based on recent data of a population of children born during the years 2008–2017. This enables us to include also information of 776 extremely immature infants born as early as at GAs of 21–24, as opposed to other studies.
A limitation of this study is that the results are applicable only to the country per se, as is the case with all national studies. Regarding the natural course of ROP, reports on the first detection of ROP and of the different stages of ROP do not tell exactly at which age the different stages started since intervals between examinations may be up to 2 weeks. Further, many doctors are involved in the national screening programme. This emphasises the importance of continuous education and information regarding technique of examination, classification of ROP, indication of treatment, follow-up after treatment, filling in protocols and registration of data, when new colleagues are starting ROP screening.
Conclusion
The present study on the SWEDROP presents 10-year data on various aspects on ROP screening in the country. Based on the results, new guidelines for screening in Sweden are proposed, reducing the upper limit for screening by 1 week, that is, including only infants with a GA of less than 30 weeks, and postponing the first examination in infants with a GA of 26 weeks or more to a PNA of 6 weeks. The proposed changes would spare many infants from stressful examinations and would reduce the economic burden of ROP screening.
Acknowledgments
We thank statistician Marcus Thuresson, Statisticon AB, for help with the statistical analyses. We also thank previous members of the SWEDROP steering group during the study period, Abbas Gorgah Al-Hawasi, Peter Jacobson, Kent Johansson, Pia Lundgren and Åsa Nilsson, as well as all ROP screening colleges in Sweden.
References
Footnotes
Contributors GH and EL are responsible for data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics committee of the Faculty of Medicine, Uppsala University, Sweden (Dnr 2010/117/2).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request. All data relevant to the study are included in the article or uploaded as supplementary information.
Linked Articles
- At a glance