Article Text

Abstract
Purpose The aim of this study is to evaluate the efficacy of topical cysteamine 0.55% eye drops in the treatment of corneal cystine crystal deposits in patients with nephropathic cystinosis.
Methods Thirty-two patients with nephropathic cystinosis were prospectively included in the study. Patients with corneal cystinosis were treated with topical cysteamine 0.55% eye drops. They were examined before treatment, on each monthly visit and after treatment at the last follow-up. Photophobia was classified as grade 0 (none) for no photophobia, grade 1 (mild) for photophobia in bright light, grade 2 (moderate) for photophobia in room light and grade 3 (severe) for photophobia in dim light. Corneal cystine crystals were graded as grade 0=none, grade 1=1–10 crystals/mm2, grade 2=11–50 crystals/mm2, grade 3=more than 50 crystals/mm2. The main outcome measure was evaluation of photophobia and resolution of corneal cystine crystals.
Results There were 13 male and 19 female patients. The mean age was 8 years with an age range of 8 months to 19 years. The mean follow-up period was 4.1 years with a range of 2–8 years. Improvement of photophobia was not clinically significant in symptomatic patients. Patients displayed statistically significant worsening of corneal cystine deposits during the follow-up period.
Conclusions This study has shown that topical 0.55% cysteamine eye drops may have limited effects in decreasing the corneal cystine deposits in patients with severe forms of nephropathic cystinosis.
Trial registration number NCT02766855, Results.
- Cornea
- Treatment Medical
- Genetics
Statistics from Altmetric.com
Cystinosis is a rare autosomal recessive disorder due to impaired transport of cystine out of cellular lysosomes. The estimated incidence is 1 in 100 000 live births.1 The disease results in intracellular accumulation of cystine in several organs and tissues including the kidneys, eyes, bone marrow, liver, spleen, pancreas, thyroid, muscle and brain.2 The implicated gene is CTNS. CTNS encodes cystinosin which is a 367 amino acid integral lysosomal membrane protein that transports cystine out of the lysosome. As a result of deficient or absent cystinosin, cystine accumulates within lysosomes and forms crystals in tissues including the cornea.3
Three phenotypes of cystinosis have been described based on age of onset and severity of symptoms. These can be either nephropathic or non-nephropathic. Nephropathic cystinosis is divided into infantile (classic) and intermediate (juvenile-onset or adolescent) types. Non-nephropathic cystinosis was formerly called benign or adult type cystinosis but is now termed ocular cystinosis.3 Nephropathic or classic infantile cystinosis is the most severe phenotype. If untreated, it inevitably leads to terminal renal failure in the first decade of life.2 ,3 Early manifestations include Fanconi's tubular syndrome, which develops in 95% of patients as early as 6–12 months of life. By the age of 10 years, 50% of patients develop hypothyroidism and photophobia. Other manifestations of nephropathic cystinosis include impaired growth and rickets.4
The intermediate form of cystinosis (late-onset nephropathic) has the same manifestations of the nephropathic form but displays a late age of onset.3
Non-nephropathic or ocular cystinosis is characterised by corneal crystals only and photophobia but is not associated with systemic manifestations.3
Different CTNS mutations produce the three different phenotypes, which vary based upon the amounts of residual cystinosin activity.3
Cystinosis should be suspected in all patients with failure to thrive who have signs of renal Fanconi syndrome.2 ,5 At 1 year of age, cystine crystals are observed in the cornea and is pathognomonic of cystinosis. Detection of elevated intracellular cystine content is the mainstay for the diagnosis. Several biochemical methods are used for cystine measurement, such as a cystine-binding assay, amino acid chromatography or high performance liquid chromatography.2 ,5 The diagnosis is confirmed by cystine measurement in a mixed white blood cell preparation enriched in polymorphonuclear leucocytes. The measurement is performed using the cystine binding protein assay or mass spectrometry.2
The purpose of this study is to evaluate the effects of 0.55% cysteamine eye drops on the signs and symptoms associated with corneal cystine crystals in patients with nephropathic cystinosis.
Methods
Patients
The study included a total of 32 patients with confirmed diagnosis of nephropathic cystinosis during the period of 2004 to 2012. All patients were attending the nephrology clinic at King Faisal Specialist Hospital & Research Center and were on oral cysteamine therapy.
Diagnosis of cystinosis
The diagnosis of cystinosis was made by a paediatrician. It was confirmed by demonstrating leucocyte cystine concentration level of more than 2.0 nmol half-cystine/mg protein and clinical evidence of corneal deposition of cystine. All patients were evaluated by an ophthalmologist, a paediatrician and a paediatric nephrologist.
Examination
Patients had ophthalmic examination before initiation of topical cysteamine 0.55% eye drops, at monthly intervals and at the conclusion of therapy. The following parameters were recorded: photophobia, slit lamp assessment of the density of corneal cystine crystals and visual acuity. Photophobia was classified as grade 0 (none) for no photophobia, grade 1 (mild) for photophobia in bright light, grade 2 (moderate) for photophobia in room light and grade 3 (severe) for photophobia in dim light. Corneal cystine crystals were graded as grade 0=none, grade 1=1–10 crystals/mm2, grade 2=11–50 crystals/mm2, grade 3=more than 50 crystals/mm2. The density and level of cystine crystal deposits in the corneal layers were recorded and the location whether peripheral or central was identified. The presence of conjunctival cystine crystals, iris deposits and fundus deposits were recorded whenever possible. Best corrected visual acuity was measured by Snellen chart. In the preschool children, picture optotype visual acuity charts were used.
Cysteamine eye drops
Cysteamine 0.55% eye drops were prepared under laminar flow and aseptic conditions at King Faisal Specialist Hospital & Research Center pharmacy. Pretreatment consent was signed by the patient guardian and a thorough explanation of the purpose of the treatment was explained. Patients were asked to use the eye drops every 2 hours while awake to both eyes. Patients were supplied with a checklist sheet to test the compliance on a daily basis and were given instructions on the method of application of the eye drops. Patients were supplied with a fresh bottle of cysteamine 0.55% eye drops every 10 days during the study period.
Statistics
Statistical analysis was performed using SPSS software V.17.0.1 for Windows (IBM Corp., New York, New York, USA). The extended Mantel-Haenszel χ2 method for linear trends was applied to assess the treatment effectiveness by correlating the baseline results with the results of the last follow-up. A level of p<0.05 was set as statistically significant.
Results
A total of 32 patients with nephropathic cystinosis were included. There were 13 male and 19 female patients. The mean age was 8 years with an age range of 8 months to 19 years. The mean follow-up period was 4.1 years with a range of 2–8 years.
At first presentation, there was no photophobia (grade 0) in 14 patients, photophobia to bright light (grade 1) in 9 patients and photophobia to room light in 9 patients (grade 2). Corneal cystine crystals were found in all patients; 8 patients had grade 1 crystals, 5 patients had grade 2 crystals and 19 patients had grade 3 crystals. The crystals were found in the epithelial layer in 6 patients, in the epithelium and stroma in 5 patients and affected all corneal layers in 21 patients (figure 1). The location of the identified crystals varied across the cornea from patient to patient. The crystals were located in the periphery of the cornea in 5 patients, centrally in 1 patient and at both the centre and the periphery of the cornea in 26 patients. Cystine deposits were also found in the conjunctiva in 27 patients, in the iris in 14 patients and in the retina of 3 patients (figure 2).

Slit-lamp colour photography demonstrates cystine crystals affecting all layers of the cornea.

{kind=link}
{kind=link}
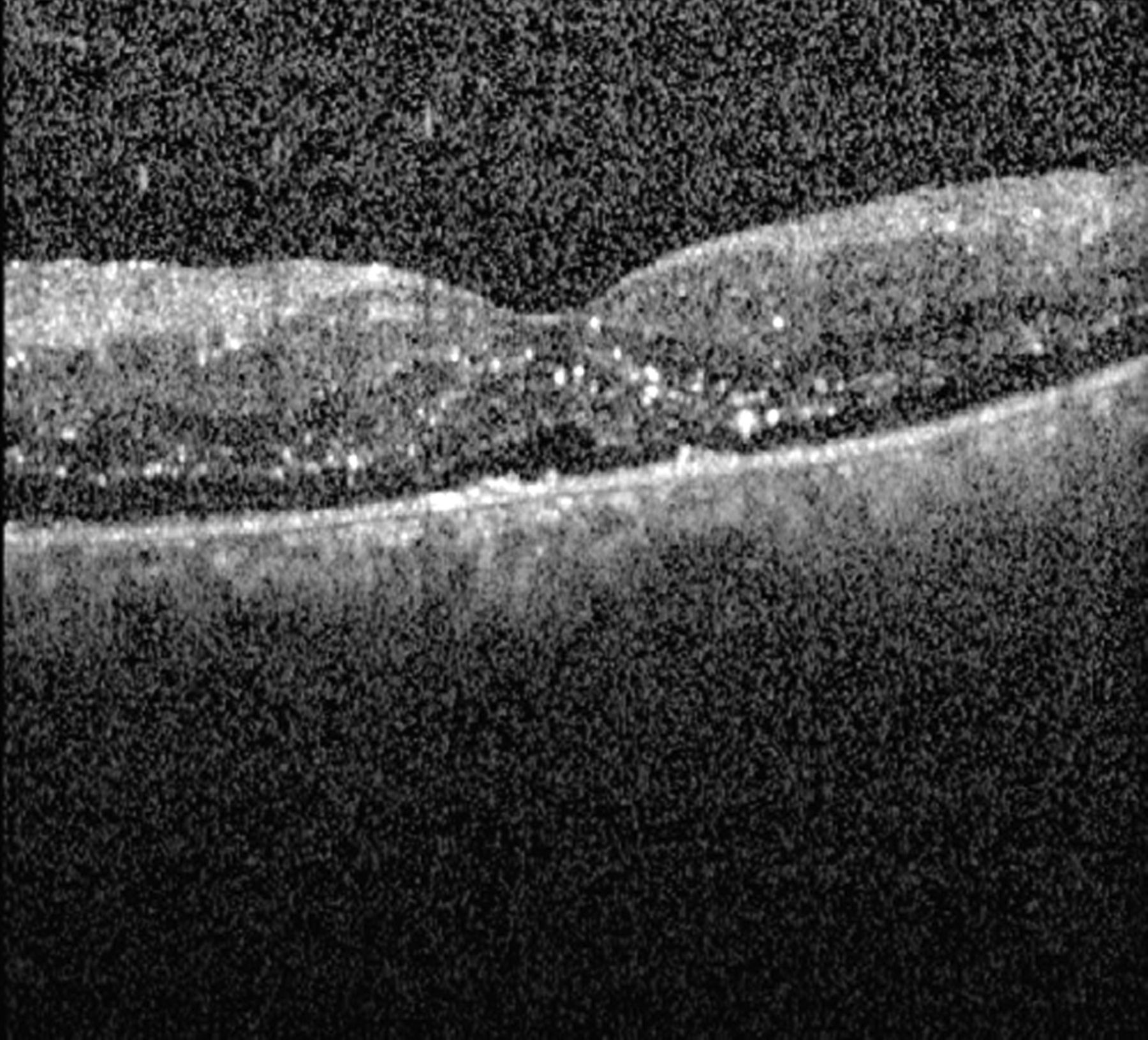
Spectral optical coherence tomography scan demonstrates cystine crystals in the retina.
Among the 14 patients with no photophobia, 10 patients did not develop any increase in symptoms and 4 patients progressed to grade 1 despite treatment. Among the 18 patients with photophobia, 7 (39%) patients had improved symptoms, 6(33%) patients were stable and 5 (28%) patients developed more severe photophobia (p=0.165). The response to treatment was not correlated to the density, level or location of the corneal cystine deposits at the time of presentation. The response of corneal cystine crystals to topical cysteamine therapy was also variable. In 21 patients the condition was stable and the patients maintained the same grade of corneal deposit before and after treatment while in the remaining 11 patients there was an increase in the density of the crystals despite the application of topical cysteamine eye drops (p=0.037). The response to treatment was not affected by the level or location of the corneal crystal deposits. Visual acuity could be measured before and after treatment in 36 eyes of 26 patients. There was no statistically significant change in visual acuity. The mean visual acuity before treatment was 0.8 (range 0.5–1.0) and after treatment was 0.8 (range 0.3–1.0).
Discussion
The most commonly encountered ocular symptoms of corneal cystinosis include photophobia, foreign body sensation and pain.3 ,4 In our study, 18 (56%) patients had photophobia at presentation. Corneal cystine crystals were found in all patients in the study group at the time of presentation. Nineteen (59%) patients out of the 32 patients had grade 3 crystals with more than 50 corneal cystine crystals/mm. In the majority of the patients (66%), the crystals affected all corneal layers. The crystals affected both centre and periphery of the cornea in 81% of patients.
Accumulation of cystine crystals within the cornea and conjunctiva are pathognomonic of cystinosis.3 On slit-lamp examination, the crystals appear as needle-shaped, reflective corneal opacities.3 They tend to diffusely span the entire cornea with involvement of the epithelium, stroma and endothelium. There is progressive accumulation of corneal crystals with increasing age. By the age of 12 years, most affected corneas demonstrate marked crystal deposits.3 ,4 Corneal cystine crystals begin in infancy and can be identified on slit-lamp examination in all nephropathic cystinosis patients by 16 months of age. The majority of affected corneas demonstrate marked crystal formation by the age of 12 years.3 ,4
In addition to corneal involvement, crystal accumulation within the conjunctiva, iris, ciliary body, choroid, fundus and optic nerve have been reported.3 ,4 ,6 ,7 Among our patients, cystine deposits were also found in the conjunctiva in 27(84%) patients. Deposition of biomicroscopically evident cystine crystals was found in the iris of 14 (39%) patients and in the retina of 3 (9%) patients.
The mainstay of treatment for cystinosis is oral cysteamine. If treatment is initiated early in life, it may stabilise glomerular function, improve growth rate and obviate the need for thyroid hormone replacement.8 The effect of oral cysteamine in dissolving corneal crystals is poor; this may be explained by poor corneal tissue absorption of cysteamine at the ocular level.8 Topical cysteamine treatment has been shown in several previous studies to efficiently dissolve corneal crystals and significantly alleviate the symptoms of photophobia, blepharospasm and eye pain that compromise the quality of life.8–12 At room temperature, however, cysteamine oxidises to its disulfide form, cysteamine.8 Cysteamine is not as effective as cysteamine in reducing corneal cystine crystals because cysteamine, theoretically, tends to dissolve both intracellular and extracellular crystals, whereas cysteamine tends to dissolve only intracellular crystals because it must first be reduced to the free thiol by the cytoplasmic-reducing environment.12
In this study, 7 (39%) out of 18 patients with photophobia showed improved symptoms, 6 (33%) patients were stable and maintained the same grade of photophobia and 5 (28%) patients deteriorated despite treatment with topical cysteamine. Eyes treated with cysteamine 0.55% eye drops failed to show decrease in corneal cystine crystals despite good compliance to therapy among the patients. Twenty-one (66%) patients had the same grade of corneal cystine deposits following therapy and 11 (34%) patients developed higher grade of deposits despite therapy. The effect of therapy on photophobia and corneal deposits was not dependent on the initial grade, level or location of corneal deposits.
Several previous reports have shown the efficacy of topical cysteamine in relieving both signs and symptoms of corneal cystinosis.8–12 Our findings, however, demonstrate that there was no statistically significant improvement of photophobia and statistically significant worsening of corneal cystine deposits following topical cysteamine 0.55% therapy. It is possible that the eye drops were washed out of the eyes due to tearing associated with the immediate discomfort following application of the eye drop.
MacDonald et al 13 studied the usefulness of four times daily topical cysteamine 0.3% drops in reducing crystal formation within the corneas of patients affected by nephropathic cystinosis. They found no reduction in crystal formation in their patients after a follow-up period of 7 months.
Another explanation of limited efficacy of cysteamine in the patients is genetic heterogeneity. It has been suggested that cystine storage in tissues is not completely cleared by cysteamine.14 The existence of modifier genes may be responsible for the broad range of phenotype in patients with or without cysteamine.14
Our study demonstrated lack of efficacy with topical cysteamine 0.55% eye drops. The concentration of the eye drops is similar to what was previously reported in the literature. The preparation was compounded at a major pharmacy of King Faisal Specialty Hospital. The lack of response may be due to low concentration of cysteamine, poor absorption and severity of nephropathic cystinosis, and high concentration of cystine in the cornea.
After initiation of successful renal transplantation and cystine depleting therapy, non-renal tissues continue to accumulate cystine. Long-term anterior segment complications in older patients with nephropathic cystinosis included superficial punctate keratopathy, filamentary keratopathy, band keratopathy, peripheral corneal neovascularisation, posterior synechiae, angle abnormalities, pupillary-block glaucoma and phthisis.3 Accordingly, an effective topical therapy is needed to clear the corneal crystals. Future studies are needed to find out the optimal concentration and proper formulation of cysteamine to overcome the instability of the compounded solution and to improve the compliance of the patients. Recently, a synergistic drug delivery system was evaluated for its efficacy in enhancing the therapeutic efficacy, improving the drug stability and minimising the local immune responses in the development of drug delivery systems.15 The application of this novel therapeutic modality on human corneal cystinosis may enhance the efficacy of topical cysteamine in human subjects.15
Unlike previous studies, topical cysteamine therapy had limited effects in the treatment of severe corneal cystinosis in this study. Genetic variations and poor tissue absorption of cysteamine eye drops may have predisposed to the poor outcome following treatment.
Acknowledgments
The authors thank Dr Feras Wafaii for help with data collection.
References
Footnotes
Competing interests None declared.
Ethics approval The Protocol was approved by the Institution Review Board (IRB) of King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia and The Eye Center, Riyadh, Saudi Arabia. The study design complied with the standards set forth by the Declaration of Helsinki and was registered at clinicaltrials.gov (registration number is NCT02766855).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance