Article Text

Abstract
AIMS To evaluate the claim that topical proxymetacaine produces little or no discomfort on instillation by comparing it against topical amethocaine.
METHODS This randomised, masked, double blind, prospective study involved 53 consecutive patients. Each patient received one drop of amethocaine 0.5% in one eye and one drop of proxymetacaine 0.5% in the other. The duration of the stinging sensation and degree of discomfort (using descriptive and a linear analogue method) for each topical anaesthetic was assessed.
RESULTS The mean duration of stinging was 3.2 seconds for proxymetacaine and 22.1 seconds for amethocaine the difference being statistical significant (p <0.001). The mean descriptive discomfort score was 2.6 for proxymetacaine and 14.2 for amethocaine (p=0.01). The mean linear analogue score was 5.8 for proxymetacaine and 35.6 for amethocaine (p<0.001). Proxymetacaine had a successful tonometry rate of 93% and amethocaine 98%.
CONCLUSION This clinical study confirms that proxymetacaine is more comfortable on instillation than amethocaine. Minimising unnecessary patient discomfort is not only ideal, but encourages cooperation in apprehensive patients especially in children.
- patient comfort
- proxymetacaine
- amethocaine
Statistics from Altmetric.com
Topical ophthalmic anaesthetic agents available since the 1930s1 are among the commonest eye drops used in diagnostic and therapeutic ophthalmology. Most topical anaesthetics cause stinging and discomfort on instillation, as evidenced by lacrimation and blepharospasm. It is easy to disregard these uncomfortable effects as “necessary” without considering alternatives. Among the various topical anaesthetics, it has been suggested that proxymetacaine produces little or no discomfort on instillation.2 The aim of our study was to evaluate such a claim in a clinical setting, by comparing it against an established anaesthetic agent such as amethocaine.3
Study design and methods
This randomised, masked, double blind, prospective study involved a sample of 53 consecutive patients attending the ophthalmic outpatient department requiring tonometry. The exclusion criterion are as follows: ophthalmic conditions that alter corneal sensation, ocular inflammatory conditions, infections, uveitis, scleritis, blepharitis, corneal ulcerations, corneal dystrophies, patients undergoing anti-inflammatory treatments, acute glaucoma, foreign bodies, photophobia, and any pathology that can cause ocular irritation. Informed consent was obtained from participating patients.
Amethocaine 0.5% and proxymetacaine 0.5% eye drops were randomly assigned to either “A” or “B”. This assignment was unknown to the researchers until the study was completed and the code revealed. A recruited nurse, independent of the examiner instilled either “A” or “B” into the middle portion of the lower conjunctival fornix of one eye. On instillation of the drop the patient was asked to look up and the lower eyelid was gently retracted from the globe. For both drops minims, sterile, single use, disposable applicators was used. Each minim applicator contains 0.5 ml of the anaesthetic drop. One drop (50 μl) was instilled into the lower fornix. The duration of the pain was recorded. After 1 minute the tonometry was performed to assess the anaesthetic effect. The opposite eye was then instilled with the other eye drop. For example, if the right eye received “A” then the left eye would receive “B”. Each patient received one drop of amethocaine 0.5% in one eye and proxymetacaine 0.5% in the other.
The duration of the stinging sensation immediately after the instillation of “A” or “B” was measured. The severity of discomfort following the eye drops was assessed using both a descriptive method and a linear analogue method. In the descriptive method, patients assigned the sensation of discomfort into categories—“no pain”, “mild pain”, “moderate pain”, “severe pain”, and “very severe pain”. These five categories were arbitrarily scored from 0 to 4 respectively. This was followed by assessments using a 100 mm unmarked linear analogue discomfort scale.4 Subjects were asked to score the severity of their discomfort on the linear analogue scale ranging from “no pain” to “very severe pain”.
Patients’ preference of either drop “A” or “B” or lack of preference was noted. To confirm the proper instillation of the anaesthetic agents, scheduled tonometry using a Tonopen was performed 5 minutes after drop instillation, providing evidence of satisfactory anaesthetic effect. Tonometry was regarded as a success if it was easily performed and without patient discomfort. Tonometry was regarded as unsuccessful if the patient felt uncomfortable. Another drop of the same anaesthetic agent was instilled should this happen and the procedure was repeated. Any adverse reactions were documented.
Results
In the sample of 53 consecutive patients, 17 were males and 36 females. The mean age was 64.7 years (SD 19.5, range 19–87 years).
Figure 1 shows the distribution of the duration of stinging in individual patients. The mean duration of stinging for proxymetacaine was 3.2 (SD 6.3) seconds compared with the mean of 22.1 (10.7) seconds of stinging for amethocaine. There was statistical significance (p <0.001) in the difference of the above means. The mean duration of stinging overall in both groups was 12.7 (12.9) seconds.

Duration of stinging sensation reported by individual patients receiving topical amethocaine and proxymetacaine.
The percentage of patients who felt that the duration of stinging was longer using amethocaine compared with proxymetacaine was 94.3% (n=50). Only one patient (1.3%) felt that duration of stinging was longer using proxymetacaine. Two patients (2.6%) felt that there was no difference in the duration of the stinging between proxymetacaine and amethocaine.
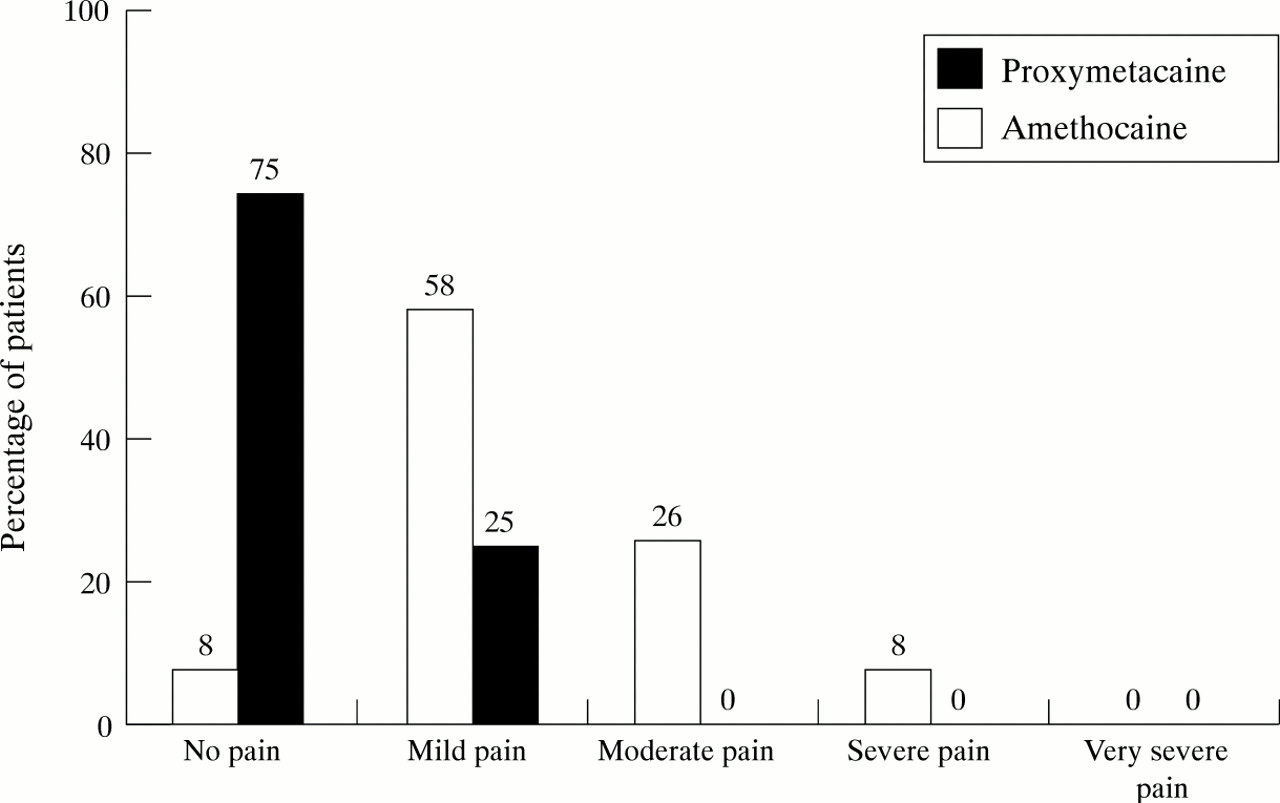
Figure 2 shows the percentage of patients experiencing “no pain”, “mild pain”, “moderate pain”, “severe pain”, and “very severe pain” on the descriptive discomfort scale for eyes receiving amethocaine and proxymetacaine. Using the scoring described above, the mean descriptive discomfort score was 2.6 for proxymetacaine and 14.2 for amethocaine, the difference being statistically significant (p= 0.01) using the Wilcoxon rank sum test.

Percentage of patients experiencing “no pain”, “mild pain”, “moderate pain”, and “severe pain” as expressed on the descriptive discomfort scale.
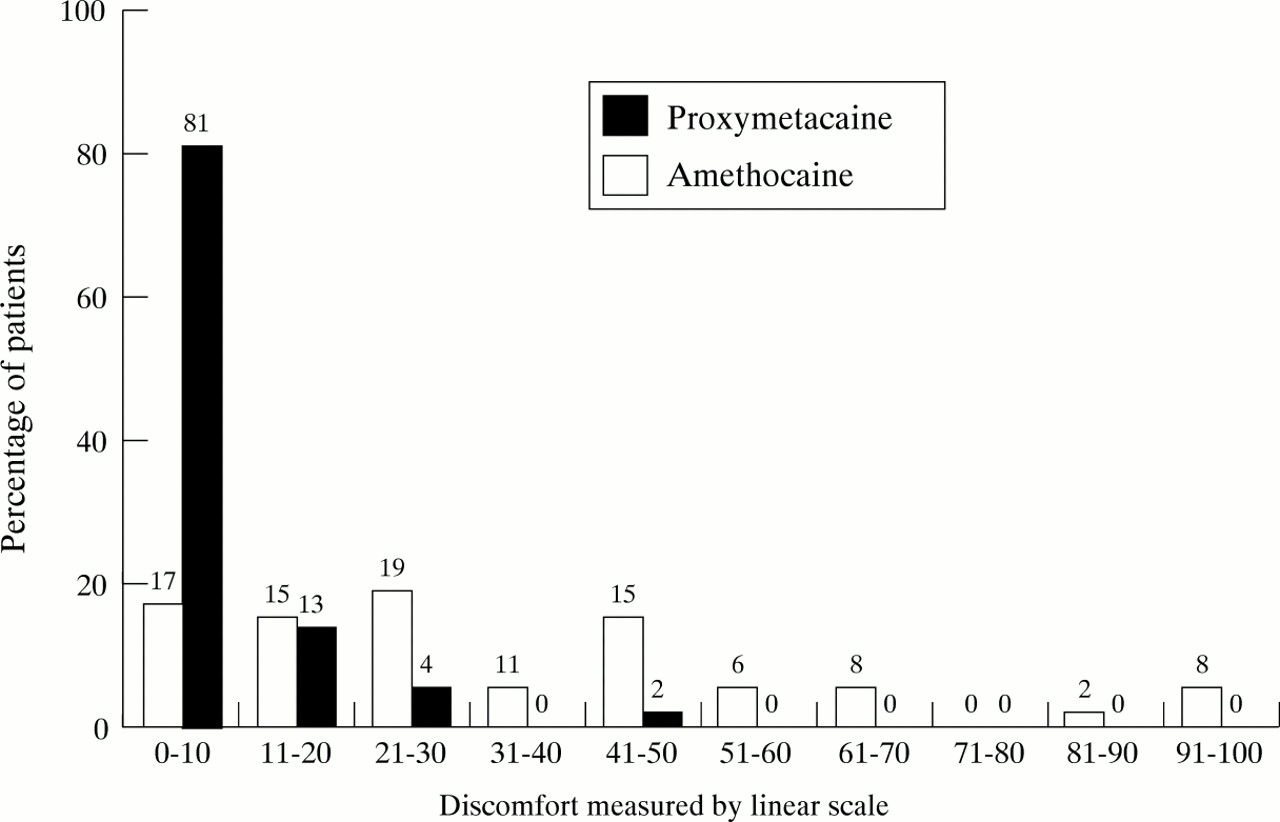
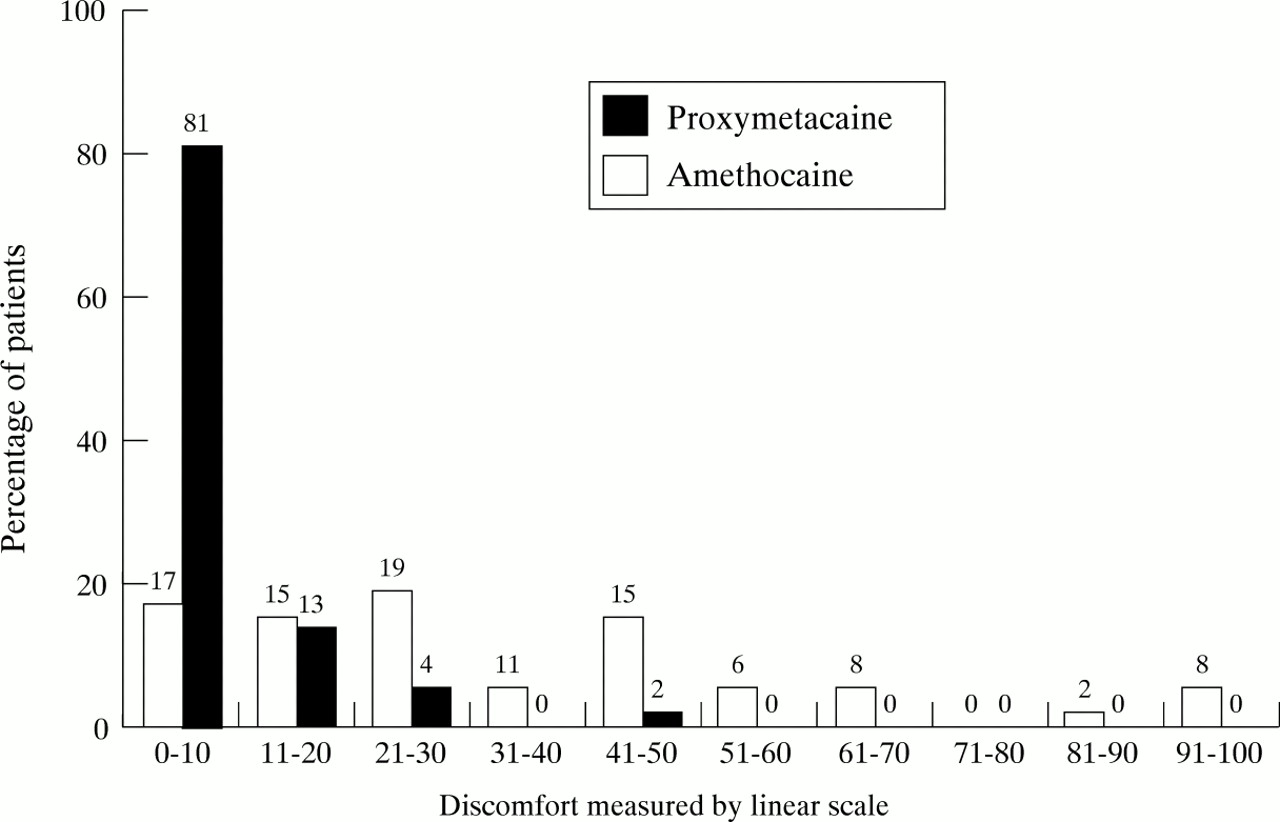
Figure 3 shows the distribution of discomfort along the unmarked linear analogue scale of length 100 mm for eyes receiving amethocaine and proxymetacaine. The mean linear analogue score was 5.8 (0.9) mm for proxymetacaine and 35.6 (2.6) mm for amethocaine. The differences between the means was statistically significant at (p<0.001) using thet test.
{kind=link}
{kind=link}
{kind=link}
Percentage of patients experiencing discomfort measured by the 100 mm unmarked linear analogue scale.
Eighty nine per cent of patients (n=47) preferred proxymetacaine while only one patient preferred amethocaine. Nine per cent (n=5) felt that there was no difference in either using proxymetacaine or amethocaine.
Proxymetacaine had a successful tonometry rate of 93% (n=49) and unsuccessful tonometry of 7% (n= 4). Amethocaine had a success rate of 98% (n=52) and unsuccessful of 2% (n=1). The differences between the success rates between proxymetacaine and amethocaine were not statistically significant (p=0.08).
When tonometry was regarded as unsuccessful, a further one drop of the same anaesthetic agent was instilled. Tonometry was then subsequently comfortable in all patients. No adverse reactions or side effects were observed.
Discussion
Topical anaesthetics act by producing reversible blockade of the sensory nerve endings5 and blocking action potentials responsible for nerve conduction at the cell membrane level.6 7 Amethocaine (a para-aminobenzoic acid) and proxymetacaine (a benzoate ester) are naturally weak bases and are slightly soluble in unionised forms.8 To improve the solubility, commercial anaesthetic agents are usually made acidic as soluble hydrochlorides.9 This allows for a longer and more stable shelf life.
The pH of anaesthetic agents affects the degree of comfort on instillation. Amethocaine has a pH of 4.54 and proxymetacaine a pH of 4.64.3 This probably explains why amethocaine (being more acidic) “stings” more than proxymetacaine. Although tears can dilute and buffer topical anaesthetic agents, this effect is not sufficient to cope with the immediate relatively large volume of anaesthetic instilled, resulting in discomfort on instillation.
This study shows that proxymetacaine is more comfortable than amethocaine for the duration of stinging (Fig 1) and for the severity of the discomfort on both descriptive (Fig 2) and linear analogue assessments (Fig 3). When one drop of anaesthetic agent was used, successful tonometry was 93% using proxymetacaine compared with 98% using amethocaine. Although these observations were not statistically significant, there is a possibility that proxymetacaine may be less efficient as an anaesthetic agent than amethocaine. The reason for the difference may be due to the difference in the pH between the two anaesthetic agents, amethocaine being more acidic. 3 10
The current retail price in the United Kingdom for a box of 20 0.5 ml minims of proxymetacaine is £6.95 and £5.75 for amethocaine.9 Although there is a 6 pence price difference per unit dispensed, the retail prices can be affected by bulk purchase.
Conclusion
This clinical study indicates that proxymetacaine is more comfortable on instillation than amethocaine. Minimising unnecessary patient discomfort is not just an ideal but is likely to encourage cooperation in apprehensive patients. In the paediatric ophthalmology, the use of eye drops which “hurt” encourages mistrust, hampering subsequent cooperation which can limit the success of the visit.
Acknowledgments
We wish to acknowledge Lin Cordey, Ann Holden, and Sara Davies for their contribution to this study.