Article Text

Abstract
BACKGROUND/AIMS Hyaluronan (sodium hyaluronate) has been shown to confer objective and subjective improvement in patients with dry eye syndrome. This study compared the efficacy and safety of a 0.1% solution of hyaluronan with 0.9% saline, when administered topically to the eye, in the treatment of symptoms of severe dry eye syndrome.
METHODS A randomised, double blind, crossover clinical trial in which subjects were randomised to receive either hyaluronan or saline, applied as one or two drops to the eye, three or four times a day or as required. After 28 days’ treatment, subjects crossed over to the other study medication for a further 28 days’ treatment.
RESULTS 70 subjects were included in the analyses of efficacy and significant improvements in Schirmer’s score (p=0.0006) and rose bengal staining score (p=0.0001) were observed during treatment with hyaluronan. In a subjective assessment of the effectiveness of two treatments, a majority of subjects felt that hyaluronan was more effective than saline in alleviating the symptoms of burning and grittiness (p<0.001). No adverse events attributable to hyaluronan treatment were reported.
CONCLUSION The study demonstrates a clear benefit of hyaluronan over saline, in both subjective and objective assessments of dry eye syndrome. Hyaluronan was shown to be well tolerated.
- Hyaluronan
- dry eye
- clinical trial
Statistics from Altmetric.com
Hyaluronan, a polymer ofN-acetylglucosamine and glucuronic acid, is widely distributed in the skin, connective tissue, and synovial fluid. In the eye, hyaluronan is found in the vitreous, the aqueous humour, and in the connective tissues of the drainage angle.1 Dry eye results from a diminished supply of tears to the eye when age related atrophy reduces the formation of tears. Some destructive processes also affect the lacrimal gland and cause dry eye. In keratoconjunctivitis sicca (KCS), lacrimal gland secretion is decreased, the precorneal tear film is hypertonic, and the tears have a decreased lysozyme content. Sjögren’s syndrome is a chronic autoimmune disease characterised by lymphoid cell infiltration of the lacrimal and salivary glands. This lymphocyte influx is paralled by acinar and ductal cell destruction leading to diminished glandular secretions. In primary Sjögren’s syndrome there is no associated connective tissue disease while in secondary disease, patients exhibit connective tissue disorders such as rheumatoid arthritis and systemic lupus erythematosus.
A topical application of sodium hyaluronate has been shown to confer both subjective and objective improvement in patients with dry eye syndrome arising from Sjögren’s syndrome or KCS.2-5Hyaluronan has also been reported to protect the corneal epithelium.6
The aim of the current study was to compare the efficacy and tolerability of a 0.1% (w/v) solution of high molecular weight (2.5 million Da) hyaluronan, as sodium hyaluronate (Fermavisc, Fermentech Medical Ltd, Edinburgh), manufactured from a bacterial source by a process of continuous fermentation, with a physiological saline solution, in patients with dry eye syndrome of known aetiology.
Patients and methods
OBJECTIVE CLINICAL ASSESSMENTS
Natural tear production was assessed by the Schirmer’s test, in which the extent of tear flow down a piece of filter paper inserted into the lateral part of the inferior fornix of the eye is measured over a 5 minute period. The use of local anaesthesia during the conduct of the test was recorded. The rose bengal test is used to locate degenerated corneal epithelial cells. The staining of the medial bulbar conjunctiva, lateral bulbar conjunctiva, and the cornea was visualised using a slit lamp microscope and the intensity of staining scored to a maximum of three points (maximum possible total score of 9).7 A higher intensity of staining indicates increased cell degeneration.
STUDY DESIGN
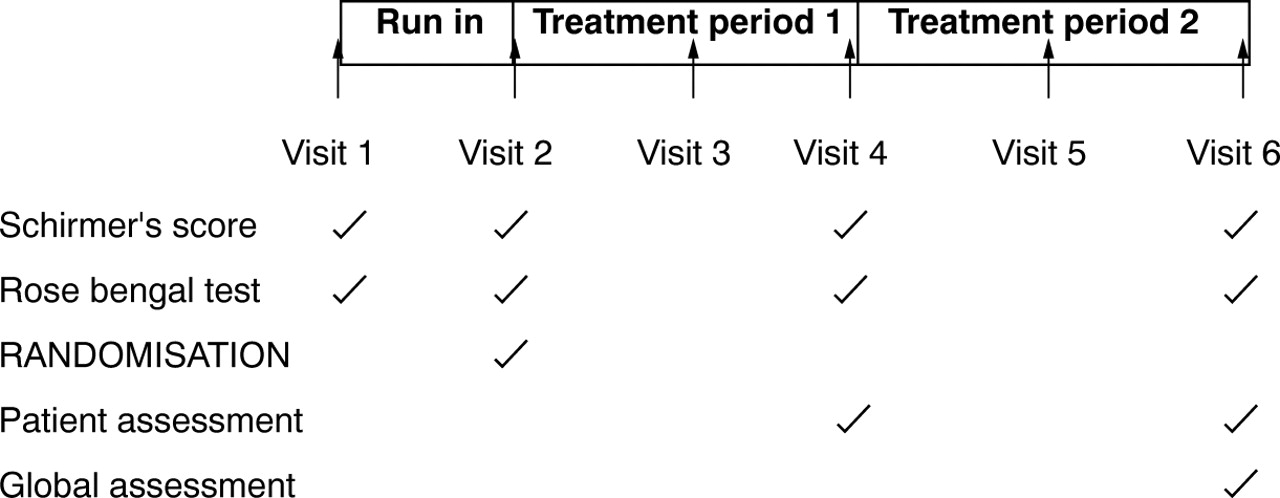
The study design was that of a randomised, double blind, two period crossover, multicentre study. Local ethics committee approval was obtained from five participating centres in the United Kingdom and Ireland before recruitment commenced. Schirmer’s and rose bengal tests were performed at baseline and subjects entered a 7 day run in during which all dry eye medication, except saline, was excluded. After 7 days, the clinical assessments were repeated and subjects were randomised to receive either 0.1% (w/v) hyaluronan or 0.9% (w/v) saline. After 28 days’ treatment, patients crossed over to the other study medication for a further 28 days’ treatment. There was no washout period between the two treatments. The clinical assessments were repeated after the completion of each of the two treatment periods (visit 4 and visit 6) and subjects were asked to record their treatment preference (see Fig 1).
{kind=link}
Study design.
The study was conducted according to the principles contained in the Declaration of Helsinki and the guidelines of good clinical practice.
STUDY MATERIALS
Hyaluronan, as sodium hyaluronate (Fermentech Medical Ltd), was manufactured by a process of continuous fermentation fromStreptococcus equi and formulated to a 0.1% solution in phosphate buffered saline. The comparator medication was 0.9% (w/v) phosphate buffered saline. Both medications were supplied as 0.4 ml solution in sterile, single use, plastic ampoules, without preservative. Dosage was 1–2 drops administered 3–4 times a day, or as required.
STUDY POPULATION
Trial subjects were aged 18 years or more, with a documented history of dry eye syndrome, due either to KCS or Sjögren’s syndrome. Written informed consent was obtained before any study specific investigations were performed. Females were either postmenopausal or using a recognised, reliable method of contraception. Pregnant or lactating females were excluded.
Subjects with unilateral dry eye were excluded, as were those with a current history or diagnosis of glaucoma, since treatments for raised intraocular pressure can affect tear production. Oral antihistamines and systemic β blockers may also affect tear flow and subjects receiving these therapies before study entry were instructed that the dose should not be changed during the course of the study. Previous anterior segment inflammation, surgical or other trauma to the eye, and contact lens use excluded study entry. Subjects with a known sensitivity to sodium hyaluronate or those who had received another experimental drug within the previous 6 weeks were also excluded.
EFFICACY AND SAFETY VARIABLES
The primary efficacy variable was the patients’ assessment of the symptoms of burning and grittiness at visits 4 and 6, after the completion of each treatment period. At visit 6, the subject was asked to make a comparative assessment of the effectiveness of the two study medications. Safety was assessed by monitoring all adverse events throughout the course of the study.
STATISTICS
A sample size of 75 fully evaluable patients was chosen to have a 90% power to detect a statistically significant difference between the treatments at the 5% level, assuming that 40% of patients expressed a clear preference for hyaluronan while the other 60% expressed preferences at random. Allowing for a withdrawal rate of 25%, it was estimated that 100 patients required to be recruited.
A single randomisation scheme, using a block size of four within centres, was produced for the study. The packaging of the two medications was identical, in order to maintain the blinding of the study, and clearly labelled with a visit number and a unique study number. Patients were randomised by selecting the lowest study number available. Code break envelopes were supplied to the centres should identification of a patient’s study medication be necessary.
Data at visits 4 and 6 were analysed according to the methods described for two period crossover clinical trials.8 All analyses were performed to allow for the presence of an order effect in the data whereby results from the first period of treatment may be systematically different from those in the second period, irrespective of the actual treatments received. Two tailed tests of significance were applied throughout. For continuous outcome measurements (Schirmer’s test, rose bengal test), parametric tests were employed (t tests). In situations where observations at the end of each treatment period were categorised on a short ordered scale (for example, relief from burning sensation), for the purposes of significance testing, it was simply noted whether the higher value was obtained in the first treatment period or the second treatment period, or whether both were identical. Prescott’s test9 to determine the statistical significance of a treatment effect, allowing for order, was then applied. For the direct comparison of efficacy obtained at the end of the trial, χ2 tests for trend (Mantel−Haenszel tests) were applied to compare the two treatment sequences.
Results
Eighty nine patients entered the run in phase of the trial and 84 were eligible for randomisation. Five patients who withdrew in the run in period were not randomised. A further eight subjects withdrew before study completion (one death from unrelated cause, one corneal abrasion while receiving saline treatment, one non-compliance, one lack of efficacy, three reasons unrelated to study, one reason unknown). Six patients who completed both treatment periods were excluded from the efficacy analysis (two errors of dispensing medication, one unilateral dry eye, one receiving other concurrent dry eye medication, one investigator error in completing the case report form, one patient not recorded on database for unknown reasons). Seventy subjects who completed both treatment periods were eligible for the efficacy analyses. This includes one subject who stopped therapy with systemic β blockers during the study.
The baseline characteristics of the 70 subjects included in the efficacy analysis are summarised in Table 1. No formal tests of significance have been applied to these data as it is known that the two groups were generated randomly and there is no sensible hypothesis to test. There are some minor differences between the patients in the two treatment sequence groups in baseline values for Schirmer’s score and rose bengal test. Such differences will have no effect on the subsequent comparison of treatments from the randomised phases of the study.
Baseline characteristics shown as mean (SD) or number
EFFICACY RESULTS
The primary efficacy variable is the patients’ assessment of outcome and Table 2 shows a three to one patient preference for hyaluronan (χ2 trend = 13.9, p <0.001). These preferences showed between centre differences, with the largest centre showing the strongest treatment effect (Table 3). No obvious explanation for this difference is available but in general the most reliable results would be expected from the largest centre. There were no between centre differences for any other variable.
Patient assessment of treatment preference
Overall patient preference by centre (combining centres 1 and 4 and comparing preference for HA with other two columns combined)
In terms of relief from burning sensation, 25 of 59 (42%) reported relief for over 3 hours while using hyaluronan compared with 14 of 57 on saline (25%). Thirty patients reported a longer duration of relief with hyaluronan and 13 with saline, a difference which is statistically significant at the 1% level when Prescott’s test, allowing for an order effect, was applied.
Relief from grittiness tended to last marginally longer than relief from burning sensation, but the treatment differences remained, and were indeed slightly enhanced, in favour of hyaluronan. Thirty three of 68 (49%) reported relief for more than 3 hours while using hyaluronan compared with 21 of 68 (31%) while using saline. Thirty three patients experienced relief for a longer period while using hyaluronan compared with 12 who received a greater duration of relief with saline (p=0.002).
The results of the Schirmer’s test show a highly significant difference between hyaluronan and saline, with subjects receiving the former having an increased tear flow in both phases of the crossover (Table 4). Statistically significant differences were observed in both right and left eyes separately and, when both eyes were combined over the two phases of the trial, the difference between hyaluronan and saline was very highly significant (t=3.6, df=68, p=0.0006).
Results from Schirmer’s test in crossover phase
Local anaesthesia was administered on only seven occasions in the conduct of the Schirmer’s test. When the tests of significance for treatment differences were recalculated, with the exclusion of results from subjects receiving anaesthesia in the randomised phases, the statistical significance of the treatment difference for the left eye was marginally reduced (t=2.5, p=0.015 versus t=2.6, p=0.013). For the right eye (t=4.0, p=0.0002 versus t=3.4, p=0.0013) and the sum from both eyes (t=3.9, p=0.0002 versus t=3.6, p=0.0006) the significance was slightly increased. The occasional use of anaesthesia in the conduct of the Schirmer’s test has therefore not influenced the results.
The results of the rose bengal test show a more pronounced benefit for hyaluronan compared with saline (Table 5). The total staining scores from each eye were consistently about one point lower when the patient was receiving hyaluronan compared with saline. Overall the treatment difference is statistically significant at the 0.01% level.
Results from rose bengal test (total score) in crossover phase
SAFETY
Eighty four patients who were randomised and issued with study medication were eligible for the safety assessment. There were a total of five adverse events reported in these subjects. Four of these were non-serious and not considered related to the study medication (headache, mild cardiac failure, influenza, corneal abrasion). The corneal abrasion occurred in a patient during saline treatment as a result of touching the surface of the eye when applying the drops. One death which occurred on study was due to leukaemia and unrelated to the study medication.
Discussion
The study shows a clear benefit of hyaluronan over saline, both in the subjective assessment of symptom relief and duration of this relief, and the objective tests of ocular structure and function. The study also demonstrates that hyaluronan is well tolerated as topical eye medication when applied, as required, over a 4 week period. Unlike other artificial tears, hyaluronan is a natural tear substitute and its concentration in tear fluid increases in response to ocular damage and during corneal wound healing.10
The symptomatic improvement reported by patients using hyaluronan and the longer duration of relief may be, in part, due to an increased stability of the precorneal tear film. This has been shown in previous studies, with a solution of at least 0.1% sodium hyaluronate required to delay breakup of the precorneal tear film.11 12 The benefit seen may also be related to the superior ability of hyaluronan to maintain the corneal epithelial barrier by improving the integrity of corneal superficial cells,13 14 possibly as a result of the ability of hyaluronan to promote corneal cell migration.15 The degree of corneal epithelial cell disruption, as measured by the rose bengal staining score, was highly significantly improved on treatment with hyaluronan and this has been observed in other studies.4 The pathological changes seen in the corneal epithelium, induced by hyposecretion of tears, have been correlated with a decrease in corneal sensitivity.16
The apparent improvement in tear production in patients receiving hyaluronan, as determined by the Schirmers’s score, may reflect the water retentive properties of hyaluronan resulting in an increased precorneal residence time of the artificial tear and increased corneal wettability17 and reduced tear evaporation from the ocular surface.18
The symptomatic benefit of hyaluronan to patients with dry eye has been clearly demonstrated in this and other studies. Further work is indicated to elucidate the mechanisms by which hyaluronan exerts its effect.
Acknowledgments
The authors would like to thank all investigators and study site personnel involved in the recruitment and treatment of subjects in this study including T Kennelly, Waterford; J Singh, Edinburgh; and V Thaller, Plymouth.