Article Text

Abstract
Aim: To explore the influence of a cilio-retinal artery on diabetic maculopathy.
Methods: In the county of North Jutland 481 diabetic subjects underwent examination for diabetic retinopathy during the period 1 June 2000 to 30 June 2001. A unilateral cilio-retinal artery was observed in 104 patients among which 29 revealed variation in right and left eye maculopathy. A bilateral cilio-retinal artery was observed in 15 diabetic subjects. The influence of a cilio-retinal artery on diabetic maculopathy was explored in a paired study.
Results: Diabetic maculopathy was found to be more severe in 26 of 29 eyes with a cilio-retinal artery (p<0.01) compared to eyes without it. The number of red dots (p<0.0001) and hard exudates (p=0.0002) were found to be significantly increased in eyes with a cilio-retinal artery, as also the number of eyes with central photocoagulation (p<0.05). In addition, clinically significant macular oedema was found to be significantly increased in eyes with a cilio-retinal artery compared to eyes without it (0.01<p<0.02).
Conclusion: In some patients, the presence of a cilio-retinal artery may worsen diabetic maculopathy.
- diabetes
- maculopathy
- retinopathy
- cilio-retinal artery
Statistics from Altmetric.com
Diabetic maculopathy is a leading cause of deterioration of visual acuity or blindness in diabetic subjects.1,2 Studies on the pathogenesis of diabetic maculopathy have been focused on retinal lesions such as microaneurisms, retinal bleeding, soft exudates, hard exudates, retinal thickening, and partial retinal capillary occlusion.3–6 Vascular endothelial growth factor and angiotensin II are also reported to be increased in diabetic subjects with macular oedema.7 Numerous studies, therefore, point towards retinal vascular lesions as a background for development of diabetic maculopathy and treatment has therefore been focused on retinal photocoagulation.8 However, these studies do not take into account a possible choroidal influence on diabetic maculopathy which so far has only been explored briefly.9,10
A cilio-retinal artery represents a vessel carrying blood from the choroidal to the retinal vascular structure. If this vascular structure or substances from the choroid could influence diabetic maculopathy, more severe maculopathy may be observed in eyes with a cilio-retinal artery. The present study therefore explored a possible association between a cilio-retinal artery and worsening of diabetic maculopathy.
PATIENTS AND METHODS
Selection of diabetic subjects
Examination for diabetic retinopathy has recently (2000) been introduced in the city of Aalborg in the county of North Jutland, Denmark. All 481 diabetic subjects undergoing diabetic retinopathy examination during the period 1 June 2000–30 June 2001 were included in the present study. Based on fundus photography diabetic subjects with a unilateral cilio-retinal artery were identified.
Examination of diabetic subjects
The diabetic retinopathy examination included visual acuity testing, pupil dilatation (Mydriacyl 1% (tropicamide) and Metaoxedrin 10% at (phenylephrine)), and fundus photography. Two colour fundus photographs (50°) of the right and left eyes, respectively, were recorded using a Zeiss digital camera (DCS 420) followed by storage on a central server. One of these two photographs was centred on the foveal region and used for macular gradation. The other represented the nasal part of the retina with the optic disc at the margin of the picture (Figs 1 and 2).

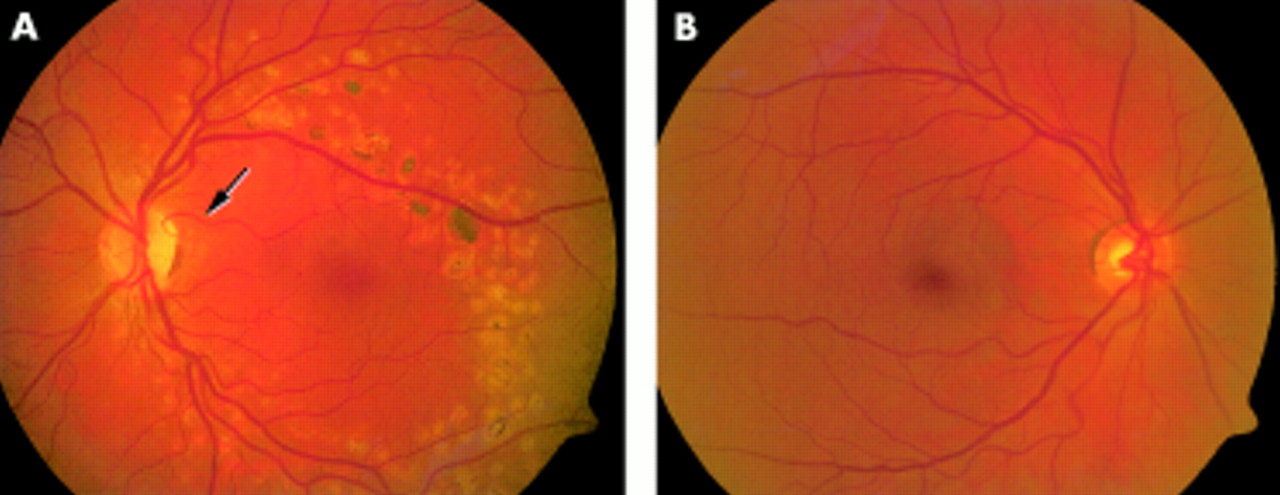
(A) Fundus photograph from a diabetic subject with unilateral cilio-retinal artery. Arrow indicates a cilio-retinal artery. An increased number of red dots are seen in this eye compared to the other eye (B). (B) Fundus photograph from the same patient (A) but from the other eye, without a cilio-retinal artery.

{kind=link}
{kind=link}
(A) Fundus photograph from a diabetic subject with unilateral cilio-retinal artery. Arrow indicates a cilio-retinal artery. Central photocoagulation has previously been given to this eye. (B) Fundus photograph from the same patient (A) but from the other eye without a cilio-retinal artery. No central photocoagulation has previously been given to this eye.
Gradation of diabetic maculopathy and macular lesions
In this study the macular region was defined as the area within the two temporal arcades—that is, the two major temporal arteries and gradation of specific lesions were carried out within this area, using a high resolution screen (Nokia 850). The number of red dots were counted after a black and white conversion of colour fundus photographs using the software program ACDSee (version 3.0). The number of hard exudates and soft exudates were corrected using the original colour fundus photographs as presented on the high resolution screen.
Diabetic maculopathy was classified as equal on both eyes or as worse in one eye. This gradation was based on the number of red dots, hard exudates, and soft exudates, where an increased number of these lesions in one eye resulted in the classification “worst maculopathy. In all except one patient an increased number of red dots were seen together with an increased number of hard exudates. In one patient the number of hard exudates was found equal in both eyes; however, the variation in the number of red dots in right and left eyes was observed in this patient. Diabetic subjects with an increased number of soft exudates in one eye also revealed an increased number of red dots or hard exudates in this eyes.
Previous central and/or panretinal photocoagulation was registered from fundus photography and confirmed from the case records of each patient.
Diabetic subjects with possible clinically significant macular oedema (94 of 481 subjects) were called for clinical examination including three dimensional evaluation of the macular region (90 dioptre lens).
Visual acuity testing
Visual acuity testing was carried out in dim light using the same projector for all visual acuity tests. Best visual acuity with own correction or pinhole was registered.
Definition of cilio-retinal artery
In this study a cilio-retinal artery was defined as a vessel starting at the optic disc, without connection to the central vascular tree and with a curvation of 90 degree or more at the margin of the optic disc. Very thin vessels (diameter <10% of central vascular structure) were not included.
Statistics
Non-parametric four sign test was used to compare the number of worst case maculopathy, the number of previously given central and panretinal photocoagulations. Significance levels were found in the Ciba Geigy tables.11 A two tailed paired t test was used to compare the number of red dots, hard exudates, soft exudates, and visual acuity. Calculations were carried out with the software package graphpad prism, version 4.0. Mean values and 95% confidence limits are given together with p values and significance at a 5% level. Mean visual acuity was calculated on logarithmically transformed parameter values.
The fractions of normal and increased urinary albumin excretion were compared in diabetic subjects with and without variation in right and left eye maculopathy using a χ2 test, which was also used to compare the clinically significant macular oedema in eyes with and without a cilio-retinal artery.
Laboratory values
HbA1c was analysed in the Bio-Rad Variant II-system (Bio-Rad Laboratories, Herkules, CA, USA) (normal values in our laboratory: 4.5–6.0%), while urinary excretion of albumin was measured by a nephelometric method. Increased urinary albumin excretion were defined either as urinary albumin: creatinine ratio greater than 2.5 g/mol or as an excretion rate greater than 20 μg/min in two out of three timed overnight urine samples. Creatinin was analysed using the Jaffa reaction.
RESULTS
Fundus photography evaluation of 481 diabetic subjects revealed a unilateral cilio-retinal artery in 104 subjects and bilateral cilio-retinal artery in 15 subjects. An examination of the macular region revealed variation in left and right eye maculopathy in 29 subjects and identical maculopathy in 75 subjects.
A careful examination of the macular region was carried out among the 29 diabetic subjects with variation in right and left eye maculopathy (Table 1). Significantly increased worse case maculopathy was found in eyes with a cilio-retinal artery compared to eyes without this manifestation (26 v 3; p<0.01). In addition, the number of red dots were found significantly increased in eyes with a cilio-retinal artery compared to eyes without it (8.2 v 4.9; p<0.0001). The number of hard exudates was also found increased in eyes with a cilio-retinal artery compared to eyes without it (6.1 v 1.7; p=0.0002). Finally, a significantly increased number of previously given central photocoagulation was observed in eyes with a cilio-retinal artery compared to eyes without it (11 v 1; p<0.05). The number of soft exudates, the visual acuity, and the number of eyes given panretinal photocoagulation were found to be equal in both groups.
Macular lesions in 29 diabetic subjects with (plus cilio-retinal artery) and without (minus cilio-retinal artery) a cilio-retinal artery
Macular lesions among the 29 diabetic subjects with variation in right and left eye maculopathy were further classified as worse in the superior part, worse in the inferior part, or equal in these two regions of the macula. The location of the cilio-retinal artery was classified as mainly superior, mainly inferior, or mainly central and compared to the macular lesions. Agreement between worse maculopathy and location of the cilio-retinal artery was observed in 19 eyes, disagreement was observed in two eyes, and in eight eyes superior and inferior maculopathy was found equal in eyes with a superior or inferior location of the cilio-retinal artery.
Eyes with possible clinically significant macular oedema were called for clinical examination including three dimensional evaluation of the macular region (90 dioptre lens) (94 of 481 diabetic subjects). Clinically significant macular oedema was observed in 13 of 134 eyes with a cilio-retinal artery while 38 of 828 eyes without this artery had clinically significant macular oedema. A χ2 test revealed a significantly increased clinically significant macular oedema in eyes with a cilio-retinal artery (0.01<p<0.02).
The group of 75 diabetic subjects with identical maculopathy was compared with diabetic subjects with variation in right and left eye maculopathy (29) (Table 2). The group of diabetic subjects with variation in right and left eye maculopathy was found to be older (p=0.012), heavier (p=0.008), and with longer duration of diabetes (p=0.021). In diabetic subjects with variation in right and left eye maculopathy, elevated systolic blood pressure was found close to the significance level of 5% (p=0.053). Diastolic blood pressure (p=0.703), height (p=0.8126), HbA1c (p=0.777), and fraction of insulin treated diabetic subjects (0.05<p<0.1) was found to be similar in both groups.
The group of diabetic subjects without variation in maculopathy has been compared to the group of diabetic subjects with variation in right and left eye maculopathy. Systolic blood pressure (BT-sys), diastolic blood pressure (BT-dia), duration of diabetes (duration), age, weight, and height has been given
DISCUSSION
In the present study all 104 diabetic subjects with unilateral cilio-retinal artery could be divided into two groups with (29) and without (75) variation in right and left eye maculopathy. Significantly increased worst case maculopathy was observed in eyes with a cilio-retinal artery compared to eyes without it, together with an increased number of eyes with clinically significant macular oedema. Furthermore, a significantly increased number of red dots and hard exudates were found in eyes with this manifestation compared to eyes without it. These data therefore clearly point towards an aggravation of diabetic maculopathy in eyes with a cilio-retinal artery. In this study a significantly increased number of eyes with a cilio-retinal artery received central photocoagulation compared to eyes without it. However, the number of eyes given panretinal photocoagulation was found to be equal in the two groups. These data therefore further support the influence of a cilio-retinal artery on diabetic maculopathy since these vessels mainly supply the macular region.
Diastolic blood pressure, HbA1c, height, and fraction of insulin treated diabetic subjects were found equal in these two groups. However, duration of diabetes, age, and weight were significantly increased in diabetics with variation in left and right eye maculopathy. Systolic blood pressure was found nearly significantly increased at 5% level (p=0.053) in diabetic subjects with variation in right and left eye maculopathy. These data might therefore suggest that a cilio-retinal artery is a separate risk factor for progression in diabetic maculopathy in addition to other risk factors such as glycaemic control and duration of diabetes.
It is normally assumed that diabetic maculopathy is a result of microvascular lesions with leakage from capillaries in the macular region. It has been reported that the appearance of diabetic maculopathy is statistically linked to diabetic nephropathy.12 However, in the present study urinary albumin excretion was found to be normal in most diabetic subjects and the fraction of diabetics with normal albuminuria was not significantly decreased in subjects with unilateral cilio-retinal artery (Table 2). These data therefore possibly suggest that other factors than microvascular lesions could be of importance in the development of diabetic maculopathy. This might include altered blood flow in cilio-retinal artery as well as increased perfusion pressure in this vessel. However, substances from the choroid might also possibly influence diabetic maculopathy.
In a study by Laux and Marquardt13 it was found that blood flow in a cilio-retinal artery was statistically linked to age. In younger patients an increased blood flow was observed in the cilio-retinal artery compared to other retinal vessels. In older patients the opposite result was found—that is, a decreased blood flow in the cilio-retinal artery compared to other retinal vessels. In the present study an increased number of red dots and also hard exudates were observed in both younger and older diabetic subjects. This might possibly indicate that blood flow in the cilio-retinal artery does not influence diabetic maculopathy.
Perfusion pressure in the choroid and the retina might differ in diabetic subjects, thereby possibly leading to aggravation in maculopathy in eyes with a cilio-retinal artery as seen in this study. However, as a result of the cilio-retinal artery, substances within the choroid might be brought to the macular region, possibly influencing diabetic maculopathy. Further studies are therefore necessary for clarification.