Article Text

Abstract
Aim: To investigate the value of whole body positron emission tomography/computed tomography (PET/CT) in screening for metastatic choroidal melanoma in patients initially diagnosed with choroidal melanoma.
Methods: 52 patients with choroidal melanoma underwent whole body PET/CT as part of their metastatic investigation. PET/CT scans were used as a screening tool at the time of their initial diagnosis. A physical examination, liver function tests, and a baseline chest x ray were also obtained. PET/CT images (utilising intravenous18-fluoro-2-deoxyglucose (FDG)) were studied for the presence of metastatic melanoma. The standards for reference were further imaging and/or subsequent biopsies.
Results: Two of 52 (3.8%) patients were found to have metastatic melanoma before treatment. The most common sites for metastases were the liver (100%), bone (50%), and lymph nodes (50%). Brain involvement was also present in one patient. One patient (50%) had involvement of multiple sites. Haematological liver enzyme assays were normal in both patients. PET/CT showed false positive results in three patients (5.7%) when further evaluated by histopathology and/or additional imaging. In seven patients (13.4%) PET/CT imaging detected benign lesions in the bone, lung, lymph nodes, colon, and rectum.
Conclusion: PET/CT imaging can be used as a screening tool for the detection and localisation of metastatic choroidal melanoma. Liver enzyme assays did not identify liver metastases, while PET/CT revealed both hepatic and extrahepatic metastatic melanoma. PET/CT imaging may improve upon the conventional methods of screening for detection of metastatic disease in patients initially diagnosed with choroidal melanoma.
- AJCC, American Joint Cancer Committee Classification
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET/CT
- melanoma
- metastasis
- imaging
- AJCC, American Joint Cancer Committee Classification
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET/CT
- melanoma
- metastasis
- imaging
Statistics from Altmetric.com
- AJCC, American Joint Cancer Committee Classification
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET/CT
- melanoma
- metastasis
- imaging
- AJCC, American Joint Cancer Committee Classification
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET/CT
- melanoma
- metastasis
- imaging
Metastatic disease influences patient management; therefore, depending on the primary tumour, various screening procedures are recommended.1–6 Choroidal melanoma metastases are most commonly found in the liver, therefore the COMS (Collaborative Ocular Melanoma Study) Group suggested baseline and periodic subsequent examinations (physical examination, liver function tests, and radiographic imaging of the chest).1–3 Abnormal elevated liver enzyme assays would prompt a subsequent MRI (magnetic resonance imaging) or CT (computed tomography) abdominal scans and biopsy for histopathological evaluation.3 Others have recommended liver ultrasonography as a screening test.4 However, recent reports have shown that liver ultrasonography, chest radiographs, and liver function tests have high specificity but low sensitivity in the diagnosis of metastatic uveal melanoma.5,6 Clearly, baseline and regular screening is warranted given the probability of micrometastases (at the time of diagnosis) and the current availability of treatments (both standard and experimental) for metastatic disease.7,8,9,10,11
Whole body PET/CT imaging is gaining worldwide acceptance in the initial staging, screening, and management of patients with cancer.12–18 It combines the anatomic characteristics found on CT with the functional metabolic aspects revealed by PET. We have evaluated the role of whole body 18-fluoro-2-deoxyglucose (FDG) PET/CT (positron emission tomography/computed tomography) imaging in the initial staging of patients diagnosed with choroidal melanoma.
MATERIALS AND METHODS
Since August 2003, 52 untreated patients with choroidal melanoma were referred for whole body PET/CT to screen for metastatic disease (table 1). Standard radiology related informed consents were obtained from all patients before PET/CT imaging as PET/CT has been approved for the staging of malignant melanoma. A physical examination, liver function tests (γ-glutamyl transpeptidase, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, lactate dehydrogenase, bilirubin), and a chest x ray were also obtained.
Whole body PET/CT in initial staging of choroidal melanoma: results of PET/CT scans
Patients underwent subsequent CT or MRI (with contrast) and fine needle aspiration biopsy if abnormalities were noted on the PET/CT scan. The subsequent imaging studies were required to aid in performing a biopsy of the lesions detected by PET/CT scans (for histopathological confirmation of the diagnosis).
PET/CT imaging
Patients were instructed to refrain from eating a carbohydrate based dinner the previous night and to fast 4–6 hours before injection of 18-fluoro-2-deoxyglucose (FDG). These measures diminish physiological glucose utilisation and reduce insulin serum levels to baseline. The full body PET/CT scan began at the top of the head and ended at the bottom of the feet.
The CT portion (General Electric Discovery ST, Piscataway, NJ with BGO (bismuth germanate) crystal) consisted of a multi-detector helical CT scanner. The FDG was injected via an intravenous line followed by 10 ml normal saline.
The resolution of the PET scan was 4 mm. The PET scan reconstructed the images and utilised the CT scan to correct for attenuation. Then Xeleris workstation (General Electric software, Piscataway, NJ, USA) was used to fuse and display the PET and CT images and to produce the final image (fig 1).

Patient 1. PET/CT fused coronal images demonstrate multiple areas of high SUV FDG uptake in the liver that correspond to low attenuation lesions seen on the transmission CT scan. These lesions were compatible with metastasis (arrow).
PET/CT image evaluation
The PET/CT images were studied for the presence of lymph node and distant metastases and were based on qualitative and quantitative analysis. Data were evaluated for areas of focally increased glucose uptake and by maximally standardised uptake values (SUV). Glucose uptake above levels of the surrounding tissue qualitatively and an uptake value above 2.5 SUV quantitatively indicated malignancy. Distant metastases were determined on an organ to organ basis.
RESULTS
Fifty two patients (24 males and 28 females) with a mean age of 64 years (range 39–95) with a diagnosis of choroidal melanoma (24 RE and 28 LE) were referred for a whole body PET/CT scan (table 1). There were 13 anterior and 39 posterior tumours. There were 16 T1 (30.8%), 28 T2 (53.9%), and eight T3 (15.4%) tumours within the AJCC (American Joint Cancer Committee) classification. Using the COMS (Collaborative Ocular Melanoma Study) Group classification, there were 16 small (30.8%), 28 medium (53.9%), and eight large (15.4%) tumours.
Two patients (3.8%) were found on PET/CT imaging to have distant metastatic disease (table 2). The mean age of the patients was 80 years. One patient had a ring melanoma. Both tumours were classified as T3 (AJCC) and as large (COMS) tumours.
Metastatic disease detected at pretreatment evaluations
Metastases were detected in the liver, bone, lymph nodes, and the brain (table 1). One patient (50%) was found to have metastases in more than one site. Hepatic metastases were detected in both patients ((100%) (figs 1 and 2)), bone in one ((50%) (fig 3)), lymph nodes in one (50%), and brain involvement in one (50%).

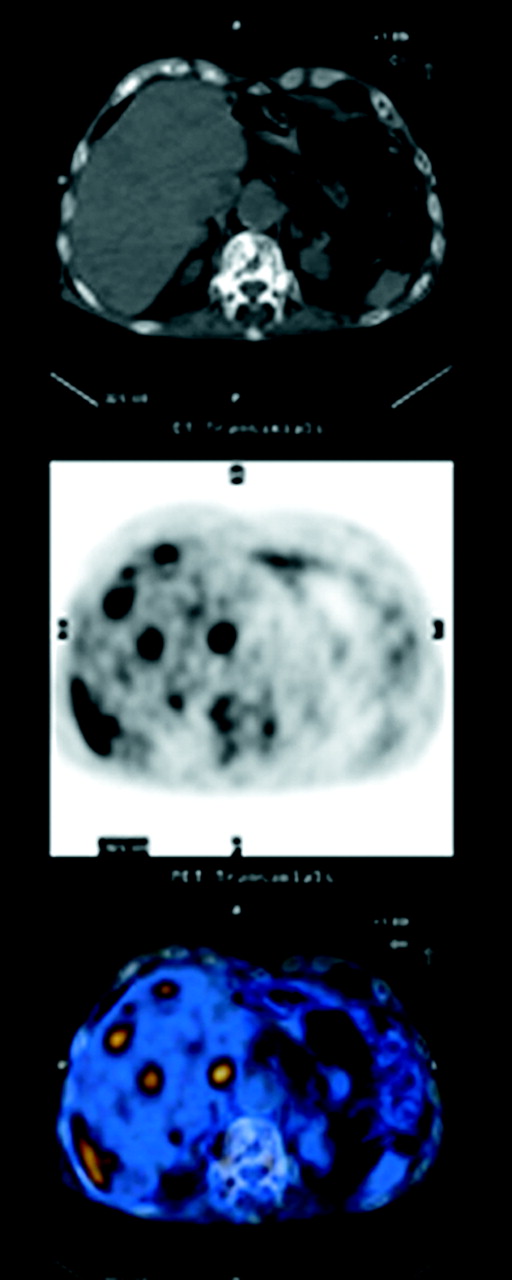
Patient 2. Abnormal PET/CT fused transaxial scans demonstrate diffuse metastatic lesions involving the liver.

{kind=link}
{kind=link}
{kind=link}
Patient 2. PET/CT fused sagittal images demonstrate high SUV metastatic melanoma in multiple vertebrae (arrows).
Both patients with hepatic metastases had normal liver enzyme assays and were found to have liver tumours on PET/CT. Liver biopsies confirmed the diagnosis and they were referred to our medical oncologist (ACP) for further management.
Two other patients were found to have small lung (n = 1) and breast tumours (n = 1) on whole body PET/CT imaging. Histopathological evaluations revealed these tumours to be synchronous primaries and not metastatic melanoma. These lesions were not detected on a previous chest x ray or mammogram.
PET/CT imaging also detected inflammatory and other benign lesions in seven (13.4%) of our patients. Benign lesions such as old fractures (n = 2), benign pulmonary nodules (n = 2), inflamed lymph nodes (n = 1), lesions of the colon (n = 1) and rectum (n = 1) were detected. PET/CT imaging was effective in differentiating these lesions from malignancy by determining the glucose uptake in these lesions compared to the surrounding tissues and by quantitatively comparing them by standardised uptake values (SUV). PET/CT imaging also detected false positive lesions in three patients (6%). But quantitative analysis (SUV) of these lesions, subsequent biopsies, and/or additional radiographic imaging (CT/MRI) helped interpret the benign nature of these lesions.
DISCUSSION
PET/CT imaging has been used in the diagnosis, staging, and restaging of various cancers.12–18 The combination of metabolic and structural information provided by the PET and CT portions, respectively, has improved the accuracy of tumour staging, detection of recurrences, and has an enormous impact on patient management.12–18 Currently, clinical studies most commonly use FDG as the radioactive tracer in PET/CT imaging. Newer radiopharmaceuticals have been found to be useful in the management of cancers (table 3). New tracers may allow quantification of cellular processes (such as hypoxia and apoptosis) and enable identification of tumours that may respond to certain targeted therapies (for example, radiotherapy).15
Newer radiopharmaceuticals in PET/CT imaging
PET/CT has been compared to PET imaging alone and whole body MRI imaging in the staging of malignancies.14,15 Cohade and colleagues compared the use of PET/CT and PET in patients with colorectal carcinoma.14 There was poor visualisation of normal organs and tissues on PET scans making lesion localisation suboptimal and there was a significant increase in the certainty of lesion localisation and characterisation with PET/CT and was valuable in determining biopsy areas. The number of definite benign or malignant lesions was increased by PET/CT as it enabled determination between physiological variants and true abnormalities.
Whole body PET/CT imaging has also been compared with whole body MRI for tumour staging.15 Both imaging procedures showed a similar performance in detecting distant metastases in 98 oncology patients, but superior performance of PET/CT in overall TNM staging was established. This study suggested the use of PET/CT as a first line modality for whole body tumour staging.
Even-Sapir and others found that PET/CT imaging was both sensitive and specific for the detection of lytic and sclerotic malignant lesions.16 It accurately differentiated malignant and benign bone lesions. We found that PET/CT imaging was valuable in the detection of bone metastases in our patients. Benign bone lesions such as old fractures were distinguishable on PET/CT imaging.
Finger and colleagues reported the first use of PET/CT in a patient with uveal melanoma and multiple hepatic and extrahepatic metastases.17 Also, Freudenberg and others found PET/CT imaging to be valuable in the detection of previously undetected hepatic metastasis and staging of advanced uveal melanoma.18
Similar to the COMS Group findings that liver function tests were highly specific but not sensitive for the detection of hepatic metastases, we found that liver enzymes were not elevated our patients with hepatic metastases.7 The detection of metastatic disease at the time of diagnosis influences management of the patient. This is particularly important in patients with large choroidal melanomas in eyes that are not painful, where enucleation can be avoided. Specification of the site of metastatic disease helps to develop better strategies for the evaluation and management of patients as PET/CT imaging can directly guide biopsies or other surgical interventions.
Though the whole body PET/CT examination is (in itself) expensive, discovering occult metastatic foci can be cost effective. The detection of extrahepatic tumours (as seen in our patients) may decrease the use of chemotherapy perfusions of the liver and surgical hepatic resections (both more expensive than PET/CT).
We currently recommend whole body PET/CT as an imaging tool for initial staging at the time of diagnosis. It appears to be more sensitive than liver function tests and is especially useful in the detection of extrahepatic tumours.
Though a prospective randomised or comparative study would be required to establish a statistical proof of the relative efficacy of whole body PET/CT imaging versus other imaging modalities (for the detection of metastatic uveal melanoma), this study suggests that PET/CT can be used for staging of uveal melanoma.
REFERENCES
Footnotes
-
Supported by The EyeCare Foundation, Inc, and Research to Prevent Blindness, New York City, New York, NY, USA
-
Competing interests: none declared