Article Text

Abstract
Background/aims: Orbital exenteration is a psychologically and anatomically disfiguring procedure reserved for the treatment of potentially life threatening malignancies or relentlessly progressive conditions unresponsive to other treatments. In this study the authors aimed to review their experience with exenteration, including indications, outcomes, and reasons for the increased rate of exenterations over the past 15 months.
Method: This retrospective study reviewed operating department records via a computerised database to identify all patients who had undergone exenteration of the orbit from 1 January 1991 to 1 April 2004 inclusive, at the Manchester Royal Eye Hospital. Where case records were unavailable, attempts were made to obtain patient data from general practitioners, local health authorities, and referring hospitals.
Results: 69 orbits of 68 patients were identified. The mean age of the cohort was 68.2 years, with 33 males and 35 females having undergone exenterations. In total, 31 patients had previously undergone treatments undertaken by the referring specialty with a mean time from the primary procedure to exenteration of 115 months. 14 different tumours were encountered, of which basal cell carcinoma (28), melanoma (10), sebaceous cell carcinoma (nine), and squamous cell carcinoma (six) were the most common. An increasing incidence was observed in cases of BCCs requiring exenteration. 30 patients received orbital prosthesis within an 11 month period post-exenteration.
Conclusion: Exenteration is a procedure performed with increasing frequency in this unit over the past 15 months, the majority the result of BCCs. A large proportion of these exenterations had undergone previous treatments under a variety of non-ophthalmic specialties in other units. Exenterations are disfiguring procedures that may, therefore, be reduced in incidence by aggressive removal at the time of primary removal. Once performed, the cosmetic rehabilitation is long, with multiple postoperative visits, independent of the method used to close the orbital defect.
- BCC, basal cell carcinoma
- SCC, squamous cell carcinoma
- exenteration
- outcomes
- complications
- BCC, basal cell carcinoma
- SCC, squamous cell carcinoma
- exenteration
- outcomes
- complications
Statistics from Altmetric.com
Orbital exenteration, first described by George Bartisch in 1583,1 is a radical procedure consisting of removal of the orbital contents, including orbital fat, conjunctival sac, globe, and part or all of the eyelids. This psychologically and anatomically disfiguring procedure is reserved to treat potentially life threatening malignancies or relentlessly progressive conditions unresponsive to other treatments. Less often, orbital exenteration may aid in palliation of severe deformity, pain, or less often as treatment for non-malignant disease.2
Cosmetic reconstruction is a major dilemma in exenterated patients, especially in the younger age group. Eyelid sparing techniques,3 retention of conjunctiva,4 and preservation of the periorbita5 are methods that have been introduced as modifications of exenteration to aid in facial rehabilitation.
In its currently practised form, orbital exenteration is performed by only a few ophthalmic surgeons in the United Kingdom, mainly in large tertiary referral units. This reflects the rarity of such surgery and the reluctance to perform orbital exenteration, especially as specialised reconstructive surgery may also be needed to mask the disfigurement. Mohr and Esser6 reported their experience of 77 cases over a 20 year period; Naquin7 described 48 cases over 25 years; Rathbun et al8 detailed 48 cases over a 30 year period; likewise, Levin and Dutton presented their experience of 99 cases over 20 years.9 The largest series in the western literature is described by Bartley et al10 of 102 patients from the Mayo Clinic over a 20 year period.
We report our experience and analyses of 69 cases of orbital exenteration over a 13 year period from 1 January 1991 to 1 April 2004.
METHODS AND SUBJECTS
This retrospective study reviewed operating department records via a computerised database to identify all patients who had undergone exenteration of the orbit from 1 January 1991 to 1 April 2004, inclusive, at the Manchester Royal Eye Hospital. All surgical records were examined to determine indications for exenteration, referral methods, diagnosis and surgical treatment elsewhere, location and extension of pathological lesions, and histological diagnosis. In the case of orbital and periorbital malignancies the histological reports were examined to determine whether or not clear histological margins had been obtained. Surgical technique, adjunctive postoperative treatments (further surgery, radiotherapy, chemotherapy), intraoperative and postoperative complications, recurrences, choice of aesthetic camouflage (occlusive patch, opaque spectacle lens, orbitofacial prosthesis), and time from exenteration to rehabilitation of the facial disfigurement with a formal prosthesis were also noted. Recurrence of any malignant disease was also noted.
Where surgical notes were unavailable, data were compiled from correspondence letters from the department of ocular prosthetics, general practitioners, and the referring hospital records.
RESULTS
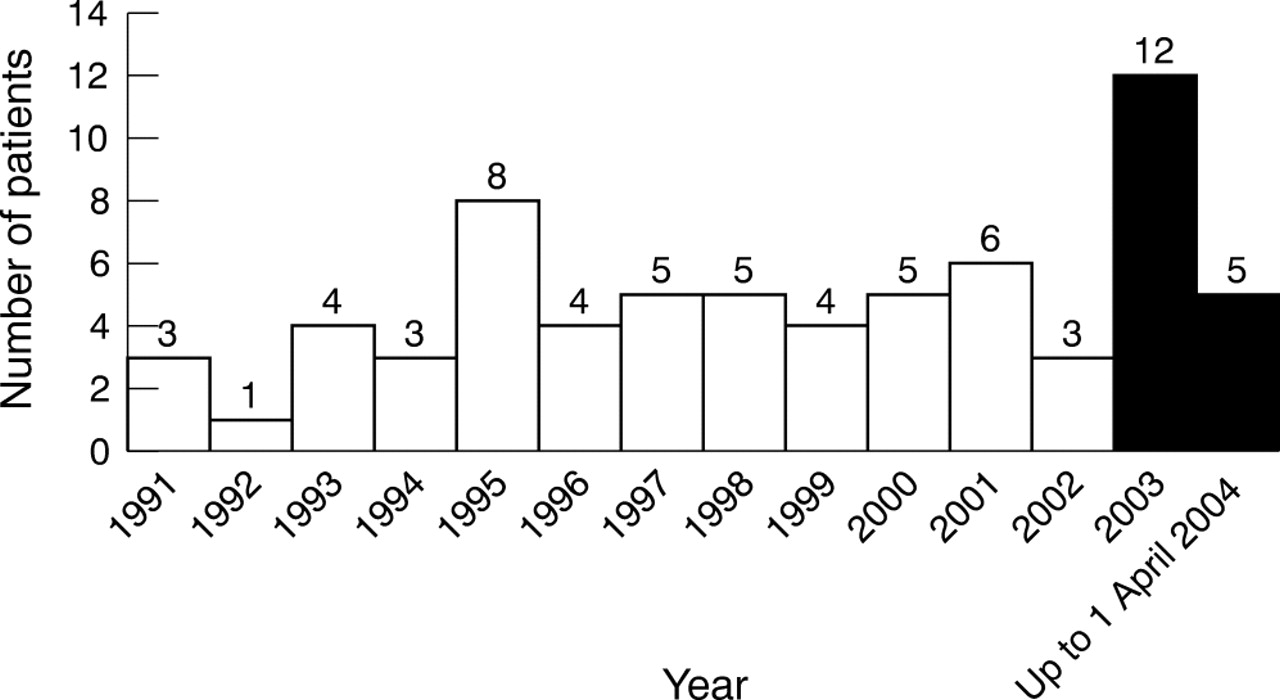
Between 1 January 1991 to 1 April 2004, 69 orbits of 68 patients were identified (one patient having bilateral exenterations for severe contracted sockets secondary to Stevens-Johnsons syndrome) from the theatre database as having undergone orbital exenteration (fig 1). Case notes for 57 patients were available for review. Histological data, letters from general practitioners, and clinic letters were used to collate the data for the remaining 12 patients. A total of 35 females and 33 males made up the study group, with 35 right orbits and 34 left orbits being affected. The mean age of the cohort was 68.2 years (median of 72, range 4–91 years), at the time of exenteration.
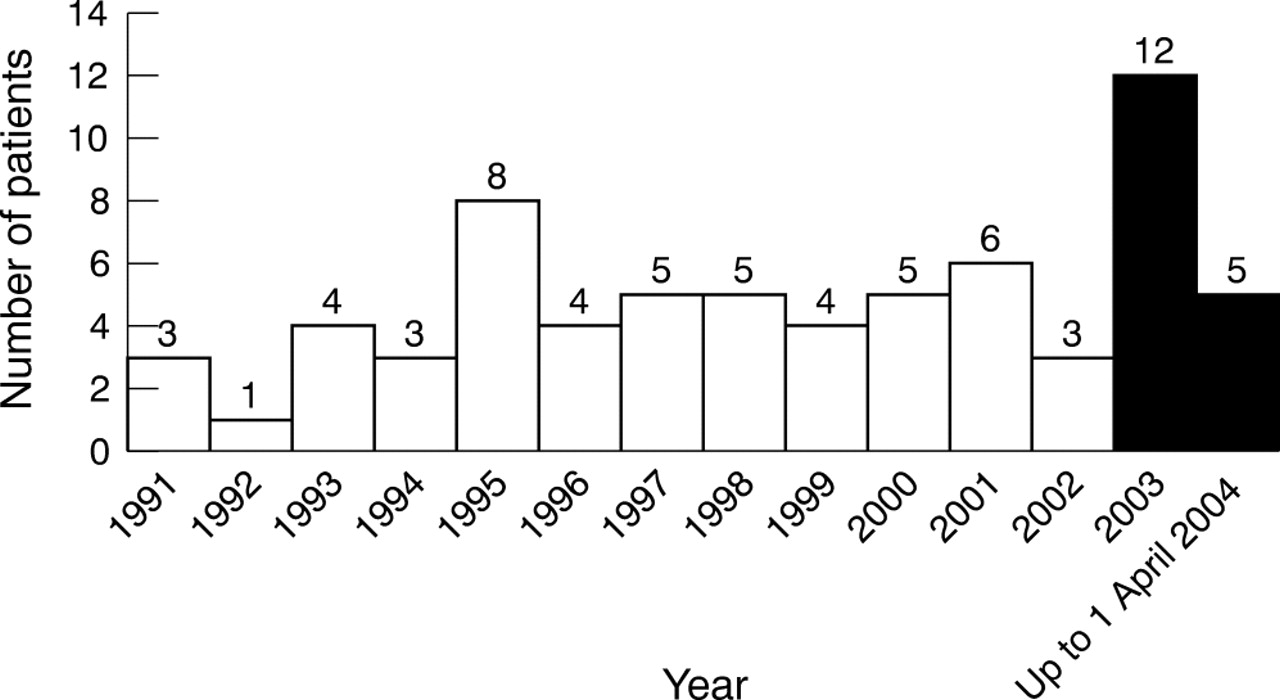
Distribution of exenteration patients over 13 year period.
Preoperative visual acuity was unavailable in 18 patients; 21 of the remaining 51 patients (41%) had a Snellen visual acuity of 6/12 or better. In the eye not exenterated, Snellen visual acuity of 6/12 or better was observed in 41 out of 53 eyes (77%), in whom visual acuity measurements were available preoperatively.
Five orbits of four patients underwent exenteration for non-malignant disease. One patient had a chronic discharging socket, another a contracted socket, and the third (two eyes) had severe Stevens-Johnson syndrome. The last patient had severe chemical injury necessitating facial cosmetic rehabilitation. This report deals chiefly with those patients with neoplastic indications for exenteration, and these five patients with non-neoplastic conditions are not considered further, except where surgical technique and complications are concerned. An overview of indications for exenteration is presented in table 1.
Indications for orbital exenteration
Although the surgery was carried out by a senior ophthalmic surgeon in all cases, referrals were made from varying specialties including dermatology, plastic surgery, neurosurgery, ENT, oncology, and from general practitioners. In total, nine patients had previous treatment in Manchester and a further 31 patients had previously undergone treatments undertaken by the referring specialty. Sixteen had had a local tumour excision, one had undergone orbital radiotherapy, and a further 10 had had a combination of surgery and orbital radiotherapy. Two patients proceeded to orbital exenteration following failed attempts at Mohs’ micrographic surgical excision of extensive periocular malignancies. Of the final two patients, one underwent enucleation and the other multiple incisions with curettage. The mean time from the primary procedure to exenteration was 115 months (range 1–600 months). Treatment modalities undertaken before exenteration are outlined in table 2.
Previous therapy
Table 3 shows the histological diagnosis of the tumour. Fourteen different tumours were encountered, of which basal cell carcinoma (BCC) (28), melanoma (10), sebaceous cell carcinoma (nine) and squamous cell carcinoma (SCC) (six) were the most common. The remaining 10 tumour types accounted for the other 11 cases.
Histological diagnosis of patients undergoing exenteration
Seventeen exenterations have been performed over a 15 month period since the beginning of 2003. Of these, 11 (65%) had orbitally invasive BCC. In the previous 12 years a total of 47 exenterations were performed, 17 (36%) of which had orbital invasion by BCCs. It, therefore, appears that invasive BCC as an indication for orbital exenteration has increased. It is also interesting that 39% in the group with exenterations over 12 years compared to an increased 69% in the group in the most recent 15 months had at least one previous attempt at cure of the lesion. This may imply a trend towards less destructive surgical techniques, resulting in inadequate surgical clearance of the tumour or inappropriate follow up before exenteration is undertaken.
The anatomical location of these lesions is outlined in table 4. The eyelids were the most common sites of tumour, occurring in 38 of the 64 exenterated patients. Malignant disease originating in the orbit and lacrimal gland accounted for a further 18 cases, with the globe and conjunctiva accounting for a further five cases.
Location of lesion
In the overall total of 68 patients (69 orbits) undergoing orbital exenteration, including those for non-malignant disease, 25 required a subtotal exenteration and a further 35 a total orbital exenteration. In nine cases the procedure was not clearly documented or the information was not retrievable. Surgery was performed under local anaesthesia with intravenous sedation in seven cases and under general anaesthesia in the remaining 62 cases. Patients were selected for local anaesthetic with sedation on the basis of co-existing medical problems, in whom general anaesthesia was deemed unsafe following advice from a consultant anaesthetist.
In three of the 64 cases requiring exenteration for malignant disease, it was deemed necessary to remove part of the bony orbit to ensure tumour clearance at the time of surgery. Overall, 29 patients demonstrated tumour to be present in excision margins on histological examination following exenteration. Nineteen of these 29 underwent further postoperative adjunctive treatment; 16 underwent orbital radiotherapy, one patient required a combination of radiotherapy and chemotherapy, one patient needed radiotherapy and further surgery, and one patient required further removal of tissue to achieve histologically clear margins.
The orbit was allowed to granulate in a total of 43 of the 64 patients. In a further 21 a split skin graft was applied. Postoperatively the most common complication was sino-orbital fistulas occurring in 15 patients. These occurred in 12 patients in whom the orbit was allowed to granulate and in only three patients in whom a split skin graft was placed. Fistula, therefore, developed more commonly with sockets left to granulate (80%) than with the concomitant use of skin grafts (20%). Seven further patients had graft failure, four of whom required regrafting and three others were allowed to granulate. A cerebrospinal fluid leak was observed intraoperatively in one patient who had previously undergone a craniotomy, but this was managed at the time of the exenteration with a local pericranial flap with no further adverse sequelae. Another patient had chronic socket discharge in the absence of a fistula. These complications and co-morbidity are detailed in table 5.
Complications and co-morbidity experienced in the 64 patients undergoing exenteration for neoplasm
There were eight cases of local or regional recurrence of tumours, outlined in table 6. This group included two SCCs, one liposarcoma, one SCC, one BCC, one melanoma, one adenocarcinoma from a gastrointestinal tumour, and one adenocarcinoma occurring in a lacrimal gland pleomorphic adenoma. Of these eight cases, six patients had tumour present on histological examination. Two had clear resection margins. Seven of the eight patients underwent adjunctive radiotherapy postoperatively.
Characteristics of patients with local or regional recurrence
In total, 31 patients had facial prostheses fitted at an average of 10 months (range 2–38 months) postoperatively (fig 2). Of these, four patients underwent successful 2 stage osseointegration before prosthesis fitting. There was no difference in the mean time to prosthesis fitting whether or not a split skin graft was applied (11 months for orbits allowed to granulate compared to 10 months using a skin graft). However, 25 patients were satisfied with the cosmetic outcome without a facial prosthesis and opted for a “pirate” patch to cover the exenterated defect. A further eight patients had not completed prosthesis fitting at the time of writing.

{kind=link}
{kind=link}
(A) Patient before facial prosthesis. (B) Patient with facial prosthesis. (Pictures reproduced with permission of patient and her parents.)
Of the five orbits exenterated for non-malignant disease, four were satisfied with the cosmetic outcome without facial prosthesis. One further orbit had prosthesis fitting 3 months after exenteration with the application of a skin graft.
A complete review of morbidity and mortality is beyond the scope of this paper and will be presented in a follow up study.
DISCUSSION
Orbital exenteration is a disfiguring procedure requiring preoperative and postoperative counselling by a multidisciplinary team consisting of an ocularist, orbital surgeon, specialist wound care nurse, and a clinical psychologist. Preoperative counselling with an ocularist is pivotal in deciding on the timing and best surgical approach—for example, whether osseointegration at the time of exenteration and before radiotherapy will save the patient later need for hyperbaric oxygen. Tumour eradication, however, should take precedence over cosmetic concerns. Often, removal of part of the bony orbit is necessary adding to the postoperative facial rehabilitation management plan. Recently, we have adapted the successful use of intravenous sedation with local anaesthetic (seven cases) as a means of exenterating the older patient with systemic co-morbidity.
Although non-malignant disease may occasionally be the indication for orbital exenteration, the vast majority of exenterations are undertaken to treat malignant disease. Bartley et al10 reported that 100 of their 102 exenterated cases resulted from malignant disease. This is similar to Levin et al (93 of 99 cases)9 and Mohr and Esser (74 of 77 cases).6 We found a similar ratio in our series of 64 of 69 cases requiring exenteration for malignant disease.
Healing of the orbital defect is dependent on the method used for reconstruction. Options include temporalis muscle transposition,11 midline forehead flaps,12 dermal graft,13 dermis fat graft,14 split skin graft,15 globe sparing exenteration,16 eyelid sparing techniques17 and spontaneous granulation.18 Allowing granulation of the defect may delay healing by up to 2–3 months. The need for regular dressing changes must be weighed against the potential benefits of healing by secondary intention—namely, an easier, quicker procedure that allows recurrences to be detected early. This provides a comparable colour match to the surrounding skin when granulation is complete.10 In our practice, postoperative dressing changes are undertaken by experienced nurse practitioners using a moist wound bed healing technique. The orbit is packed with Aquacel (Convatec Ltd, Deeside, UK), and dressings changed on a weekly basis until complete healing of the orbit.
Significant numbers of patients may develop sino-orbital fistulas from perforated sinuses occurring intraoperatively. In our series, 12 of the 43 (28%) orbits allowed to granulate developed permanent fistula formation following granulation of the orbit. This is a lower rate when compared to other large studies, 17/25 (68%) cases6 and 17/49 (35%) cases.10 Other disadvantages of secondary healing of an exenterated orbit include delayed healing, prolonged postoperative socket care, and delayed facial rehabilitation. The method employed to close the orbital defect must take into account several important issues: local and systemic tumour control and the likely survival of the patient. For instance, in cases where recurrence is unlikely and survival good, granulation may be beneficial to allow local detection of tumour. Conversely, in cases where exenteration is preformed for palliation of the neoplasm, a split skin graft will give rapid rehabilitation of the socket, and minimise hospital attendance. The use of such a graft, however, lengthens the duration of surgery and can have morbidity in older patients. Furthermore, in our study, there was no significant difference in the time to facial rehabilitation with prosthesis for those orbits allowed to granulate (11 months) compared to those orbits in which a split skin graft was applied (10 months).
In our series, BCC was the most common neoplasm (44%), followed by melanoma of the eyelids, sinuses, and globe with extrascleral spread, and then SCC. Combined, these three tumours accounted for 73% of cases requiring exenteration. Other large studies have reported varying rates of BCC. However, our rate of 44% is significantly higher. Rathbun et al8 reported 14 cases of BCC in their series of 48 (29%) exenterations, Bartley et al10 21 of 100 (21%) cases, Mohr and Esser6 six of 74 (8%) exenterations, and eight of 99 (8%) cases reported in the series by Levin and Dutton.9 Two cases of orbital exenteration in our BCC group had Gorlin-Goltz syndrome,19 one of which underwent exenteration for palliative reasons.
It is interesting to note that 23/28 (82%) cases of those orbits exenterated for orbital invasion of a BCC had previously experienced failed treatments (surgery/radiotherapy) elsewhere. This was similar to the overall figure documented by Bartley et al of 80%.10 More recently, there has been a significant increase in the number of exenterations being undertaken at our institution for orbital invasion by a BCC. Since 1 January 2003, 11/17 cases of orbital invasive BCC have undergone exenteration compared to 17/47 cases in the previous 12 years. Further, in the most recent 15 months 69% of patients have had treatment of neoplastic lesions before exenteration. In comparison, in those with exenteration over a 12 year period, 39% received previous attempts at tumour removal before referral for exenteration. There has been a trend towards a greater number of patients being treated before exenteration over the past 15 months (69%) compared to the previous 12 years (39%).
Since 2001, almost 50% of cases with orbitally invasive BCCs have been treated and referred by allied specialties—that is, plastic surgery, dermatology, and oncology, and the remaining 50% or so by regional ophthalmologists. Preceding this period, however, the majority (70%) had been treated and referred by ophthalmologists. This may reflect the more diverse interest of eyelid tumour surgery among allied specialties, often using non-Mohs’ micrographic techniques, resulting in recurrence of tumours.
A high rate of recurrence is observed in medial canthal tumours and was confirmed in our series where 12 of 23 cases of recurrence were from medial canthal lesions, necessitating exenteration.20 Only one case of BCC had recurrence after Mohs’ micrographic surgery. This may reflect the medial canthal area as an area where BCCs are common or a site where recurrence and invasion may be prominent. Many of these cases may have avoided exenteration if treated early; factors that are likely to have influenced their outcome include inappropriate surgery, inappropriate observation and/or follow up, and neglect of the lesion by the patient until a late stage in the disease.
Management of uveal tumours remains controversial, but it is now generally agreed that primary exenteration does not increase survival rates and may even hasten progress of the disease process.21–26 In our series, there was a 100% survival after 1 year. The 3 year survival fell to 33%, although only six patients have been followed up for this length of time. Furthermore, three patients had an exenteration for palliation of symptoms.
Two schools of thought exist when deciding on exenteration for these highly malignant uveal tumours with extrascleral spread. Those opposing exenteration think that the highly metastatic nature of these tumours necessarily involve micro-metastases when extrascleral extension is identified and, thus, carry a poor prognosis with or without treatment. Those advocating exenteration believe that removing the tumour as early as possible may increase survival by limiting the time for systemic spread to occur. Shammas and Blodi23 reported an overall 73% mortality of patients when extrascleral extension of the tumour was observed, compared to 22% when extrascleral extension was not observed. Kersten et al27 found a similar tumour related mortality of 81% in patients undergoing extrascleral extension. Furthermore, there was no clinically significant difference in overall survival probabilities of patients undergoing early exenteration (21%) compared to enucleation (17%) alone on extended follow up, and a 100% incidence of metastasis related to orbital recurrences needing only palliation. Thus, the preferred treatment for extrascleral extension of uveal melanomas appears to be local resection of the tumour, including enucleation and tenonectomy.
Sebaceous gland carcinoma of the eyelid is a slow growing lesion, often mimicking benign conditions, such as a chalazion.28 Of the eight cases in our series, only one had had previous surgery on the assumption that the lesion was a chalazion. After several recurrences over a 24 month period before referral, a biopsy confirmed sebaceous cell carcinoma. However, the remaining seven patients had biopsy confirmation without previous surgery elsewhere. All had confirmed pagetoid conjunctival spread. A mortality rate of 3–40% has been reported.29–34 Early diagnosis can, however, prevent mutilating exenteration and may be amenable to less destructive surgery. We found a mortality rate of 25% (two patients) in this subgroup from metastatic disease and a further one patient with metastatic disease, but having palliative treatment. All three of these patients did not achieve clear surgical margins at the time of exenteration.
CONCLUSION
Exenteration is a procedure performed with increasing frequency in our unit over the past 15 months, the majority because of BCCs. The incidence of 44% of exenterations at our unit being performed for orbitally invasive BCC is significantly higher than other large studies; 39% of these were performed in the past 15 months. A large number of patients with these exenterations had undergone previous treatments under a variety of non-ophthalmic specialties in other units, using non-Mohs’ micrographic techniques. Coupled with possible inappropriate observation and/or follow up, or neglect of the lesion by the patient, eyelid tumours are presenting at an advanced stage.
Exenterations are disfiguring procedures that may, therefore, be reduced in incidence by primary removal of tumours by those most skilled at tumour removal. Once performed, the cosmetic rehabilitation is long, with multiple postoperative visits, independent of the method used to close the orbital defect. Our rate of fistula formation is significantly lower than other reports, which may reflect surgical technique. Further, we have found the use of local anaesthetic with sedation to be very effect in specific patients with medical co-morbidity without difficulties during exenteration.
REFERENCES
Footnotes
-
Competing interests: none declared