Article Text

Abstract
Aim: To compare the diagnostic performance of accredited glaucoma optometrists (AGO) for both the diagnosis of glaucoma and the decision to treat with that of routine hospital eye care, against a reference standard of expert opinion (a consultant ophthalmologist with a special interest in glaucoma).
Methods: A directly comparative, masked, performance study was undertaken in Grampian, Scotland. Of 165 people invited to participate, 100 (61%) were examined. People suspected of having glaucoma underwent, within one month, a full ophthalmic assessment in both a newly established community optometry led glaucoma management scheme and a consultant led hospital eye service.
Results: Agreement between the AGO and the consultant ophthalmologist in diagnosing glaucoma was substantial (89%; κ = 0.703, SE = 0.083). Agreement over the need for treatment was also substantial (88%; κ = 0.716, SE = 0.076). The agreement between the trainee ophthalmologists and the consultant ophthalmologist in the diagnosis of glaucoma and treatment recommendation was moderate (83%, κ = 0.541, SE = 0.098, SE = 0.98; and 81%, κ = 0.553, SE = 0.90, respectively). The diagnostic accuracy of the optometrists in detecting glaucoma in this population was high for specificity (0.93 (95% confidence interval, 0.85 to 0.97)) but lower for sensitivity (0.76 (0.57 to 0.89)). Performance was similar when accuracy was assessed for treatment recommendation (sensitivity 0.73 (0.57 to 0.85); specificity 0.96 (0.88 to 0.99)). The differences in sensitivity and specificity between AGO and junior ophthalmologist were not statistically significant.
Conclusions: Community optometrists trained in glaucoma provided satisfactory decisions regarding diagnosis and initiation of treatment for glaucoma. With such additional training in glaucoma, optometrists are at least as accurate as junior ophthalmologists but some cases of glaucoma are missed.
- glaucoma
- optometry
- ophthalmology
- diagnosis
Statistics from Altmetric.com
Glaucoma describes a group of eye diseases in which there is progressive damage of the optic nerve characterised by a specific pattern of optic nerve head and visual field loss. It can lead to blindness if untreated. Open angle glaucoma (OAG) is the most common form of glaucoma in the United Kingdom, accounting for 75 to 95 per cent of primary glaucomas.1 The prevalence of OAG in the UK population aged over 40 is estimated to be 2.0%, with 542 000 people with glaucoma and an estimated 65% of cases currently undetected. Prevalence rises steeply with age from 0.3% at 40 to 3.2% at 70. The most important risk factors for developing OAG, identified from population studies, are raised intraocular pressure (IOP), increasing age, black race, and a family history of glaucoma.1 2 Many people have raised IOP (ocular hypertension) but do not necessarily develop glaucoma.. Ocular hypertension affects 4–5% of the adult population.1 2
In the United Kingdom, the majority of people suspected of having glaucoma are referred to the hospital eye service (HES) from the community optometrist via their GP. Cases are detected among people attending for a “sight” test, usually to obtain glasses. Between 20% and 65% of optometry referrals are false positives, placing a burden on the already overstretched outpatient services in any eye department.3–7 Definite cases of OAG or suspect OAG require continuing lifetime care.
With an aging population and an increased prevalence glaucoma and ocular hypertension with age the number of people requiring monitoring for glaucoma will probably outstrip the current capacity within existing hospital based glaucoma clinics.8–10 The concept of shared care for glaucoma, with optometrists and nurses either diagnosing or monitoring glaucoma, or both, is under development in the United Kingdom.11–14 Optometrists have suitable skills and equipment in their community practices for diagnostic testing for glaucoma. Late presentation with advanced disease is a risk factor for blindness from glaucoma.15 Late detection may be due to no contact with health services, or to a failure of the involved health professionals to detect glaucoma at an early stage.
In Grampian a new optometric glaucoma service was initiated in June 2004. This service was developed with three aims: first, to improve the diagnostic accuracy of glaucoma testing and reduce unnecessary referrals to the hospital glaucoma clinic; second, to initiate anti-glaucoma treatment promptly (instructing the GP to provide a prescription of a topical prostaglandin), avoiding the delays associated with referral to hospital; and third, to monitor people at risk of developing glaucoma in the community. Three local optometrists were enrolled in the scheme and underwent clinical training and accreditation by a consultant ophthalmologist and a glaucoma specialist (AAB). Training consisted of several practical sessions, attendance to glaucoma clinics, and teaching on various diagnostic interventions including applanation tonometry, measurement of central corneal thickness, gonioscopy, optic disc examination, and interpretation of visual field testing. A new patient pathway was introduced in which all patients with a possible diagnosis of glaucoma were referred first to an accredited glaucoma optometrist (AGO) who would determine the need for further referral and treatment.
When redesigning services, and in particular the move towards diagnosis and management in a primary care setting,16–18 the safety, cost, effectiveness, efficiency, and patient satisfaction of the new service needs to be defined. One aspect of this evaluation is to determine the reliability and diagnostic accuracy of the primary care provider in decisions regarding diagnosis and the need to treat.
Avoiding unnecessary referrals (false positives) is important, but it is equally important to assess referral accuracy in terms of cases missed (false negatives). The purpose of this study was to evaluate the reliability (interobserver agreement) and diagnostic accuracy of the decision making process of glaucoma optometrists compared with that of junior ophthalmologists (n = 9) against expert diagnosis—a consultant ophthalmologist with a special interest in glaucoma (the reference standard).
METHODS
Participant selection
Participants were identified from referrals made by community optometrists in Grampian from June 2004 to September 2005 to the glaucoma coordinator for the Grampian optometry scheme, based at Aberdeen Royal Infirmary. All patients aged over 18 who had been referred by the community optometrist to the AGO were eligible to take part.
All patients referred by the community optometrist were sent a leaflet informing them about the service and that they might be asked whether they would like to take part in a study which would involve them visiting the eye clinic at the hospital for assessment similar to those that their AGO would undertake. Participant selection was by remote allocation by an independent researcher based in the Health Services Research Unit, masked to patient details, using a computer generated random number table. Each month 15 patient study numbers were randomly selected from the list using a statistical package (SPSS). Patient lists varied each month, ranging from 25 to 71 patients.
Patients who were randomly selected to participate received a further information leaflet giving details of the study and invited to participate.
Optometrist selection and training
All Grampian optometrists were invited to participate. The selection process consisted of a written assessment of their overall glaucoma knowledge with presentation of cases, visual field abnormalities, and optic discs. A consultant evaluated and marked the answers, and the three optometrists with the highest scores were invited to participate in the scheme. Training consisted of practical sessions in which the optometrist attended two or three glaucoma clinics, until both the optometrist and consultant were comfortable with the skills acquired. During the clinics the optometrist was supervised by the consultant on applanation tonometry, gonioscopy, visual field interpretation, and optic disc examination. Written referral criteria were provided, including actions to be taken according to IOP, central corneal thickness, gonioscopy, visual field test, and optic disc data.
Clinical assessment
All participants had the following assessments for glaucoma made by the AGO in their practice: visual acuity (Snellen chart); visual fields using a threshold related strategy; corneal thickness using ultrasound pachymetry; slit lamp biomicroscopy to assess the anterior segment and optic disc; tonometry (Goldmann) to measure the IOP; and gonioscopy. Refraction and the presence of risk factors for glaucoma were also recorded.
Additionally, participants attended the eye outpatient clinic at Aberdeen Royal Infirmary and during a single visit the same clinical assessments described above were made by the glaucoma expert and a junior ophthalmologist (in any order), masked to the decisions made by other assessors with the exception of IOP measurement. Visual field testing was done with Humphrey SITA 24-2 perimetry. IOP measurements were not assessed at this visit to the eye outpatient clinic as differences in IOP level that would influence the management decision could be found. IOP data obtained by the AGO were copied on to the assessment forms by the trial coordinator and used by the doctors for their patient assessment. Trainees were aware of the study. However, the AGO was unaware of which patients would be included. Participants were specifically asked by the glaucoma coordinator not to provide information about the outcomes of previous consultations.
Statistical analysis
The primary outcome of this study was the agreement of management decision as categorised below by the AGO, junior doctor, and glaucoma ophthalmologist.
Five possible management decisions were considered (table 1):
normal and discharged;
glaucoma suspect or ocular hypertension (OHT) not requiring treatment but needing a review visit;
glaucoma suspect, or OHT, requiring treatment (which included patients with narrow anterior chamber angle and primary angle closure);
glaucoma (defined as the presence of glaucomatous damage in optic disc and/or visual field examination);
glaucoma requiring urgent treatment and referral.
The proportion of disagreements and the precision of the estimates were calculated, along with the 95% confidence interval (CI) for each outcome. Two different comparisons were made: the presence of glaucoma (decision 4 or 5) vs the absence of glaucoma (decisions 1, 2, or 3); and treatment required (decisions 3, 4, or 5) vs no treatment required (decision 1 or 2) (table 1). Weighted κ statistics (with SE) were estimated, assigning similar weight to disagreements of the above scale (1–5, table 1).
The sample size calculation was based on an estimate of 20% disagreement in management between the AGO and glaucoma ophthalmologist. Based on the results of a previous randomised trial comparing optometric decisions vs hospital decision for established glaucoma monitoring,20 a sample size of 100 participants gives the opportunity to detect a precision of disagreement of 15% with a 95% confidence interval. In addition, sensitivity and specificity, with corresponding 95% confidence intervals, were estimated for the AGO and the junior ophthalmologists, and the differences and associated 95% confidence intervals in sensitivity and specificity for the two groups of health professional were estimated.
The study was approved by the Grampian research ethics committee and the Research and Development Board of NHS Grampian. The research was conducted according to the tenets of the Declaration of Helsinki
RESULTS
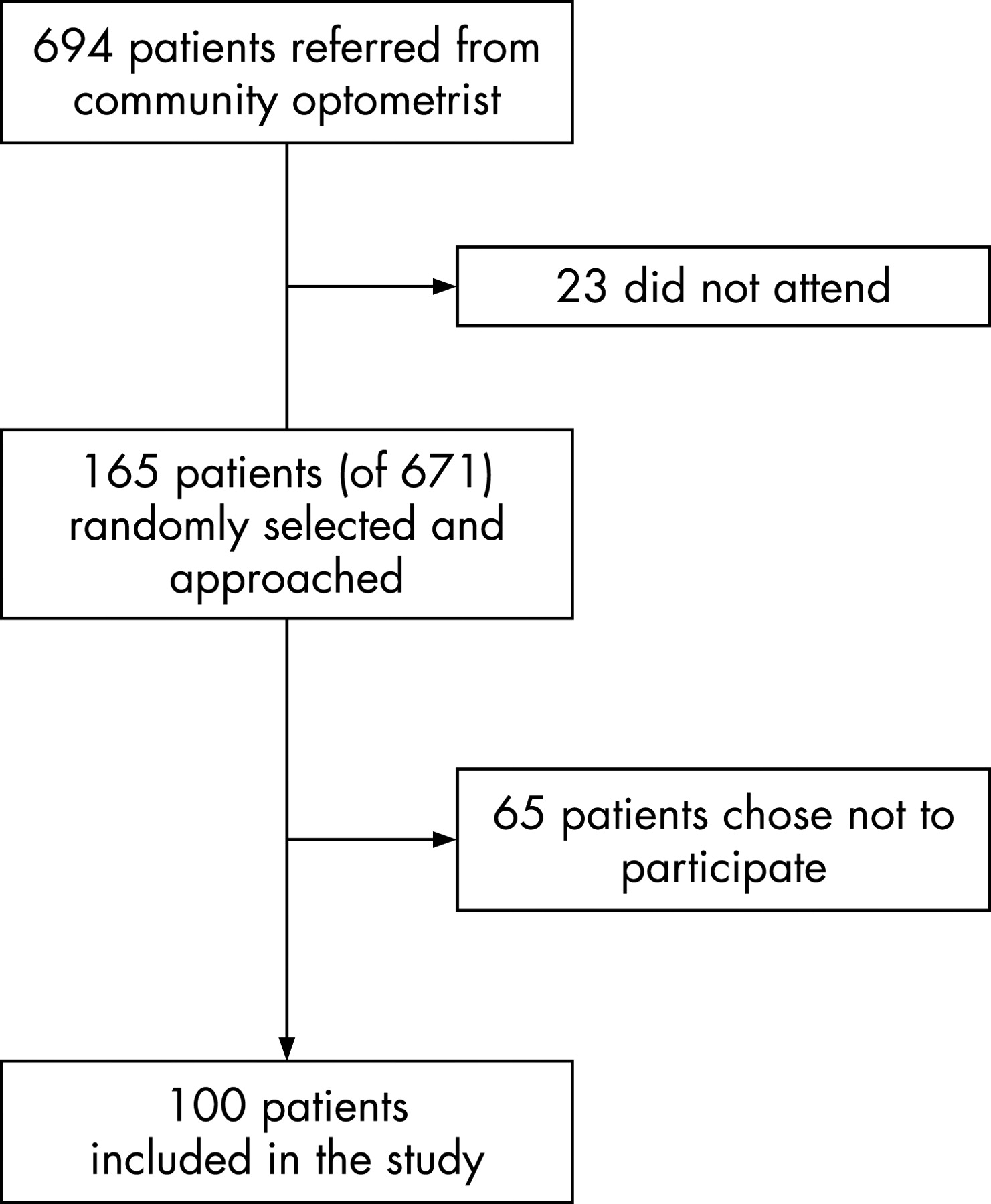
Between June 2004 and September 2005 the glaucoma trained optometrists examined 671 of 694 patients referred to the scheme (fig 1). Among these patients, 165 were randomly selected. Sixty five patients did not wish to participate in the study or in the shared care scheme. In all, 100 people (61% of those approached) were enrolled and examined by the consultant ophthalmologist and the junior ophthalmologist at the hospital eye outpatients department. The diagnosis by the consultant ophthalmologist, demographic characteristics, the highest IOP, and the family history of glaucoma are given in table 2. All patients but one (black) were white.
{kind=link}
Weighted κ values were 0.534 between optometrist and consultant, 0.452 between consultant and junior physician, and 0.450 between optometrist and junior physician (table 3). The agreement between the AGO and the consultant ophthalmologist in the diagnosis of glaucoma was substantial (89%, κ = 0.703, SE = 0.083). Agreement about the need for treatment was also substantial (88%, κ = 0.716, SE = 0.076). Patients needing urgent referral (n = 2) were correctly identified.
The agreement between the trainee ophthalmologists and the consultant ophthalmologist in the diagnosis of glaucoma was moderate (83%, κ = 0.541, SE = 0.098), and the agreement in recommending treatment was also moderate (81%, κ = 0.553, SE = 0.90).
The agreement between the AGO and the junior physician in detecting glaucoma was fair (66%, κ = 0.222, SE = 0.101), while the agreement to treat was substantial (85%, κ = 0.624, SE = 0.088) (table 3).
The diagnostic accuracy of the AGO in detecting glaucoma in this population was high for specificity (0.93 (95% CI, 0.85 to 0.97)) but lower for sensitivity at 0.76 (0.57 to 0.89) (table 4). The performance was similar when accuracy was assessed against a decision that treatment was required (sensitivity = 0.73 (95% CI, 0.57 to 0.85); specificity = 0.96 (0.88 to 0.99)). Differences in performance between AGO and the junior ophthalmologist were not statistically significant (table 4).
DISCUSSION
In the United Kingdom, community optometrists are responsible for detecting eye diseases in patients visiting their practices. After using a variety of tests and completing an ocular examination the optometrists refer to the hospital eye service those patients who have some abnormal findings. Owing to the aging population, the increasing prevalence of glaucoma and ocular hypertension, the limited resources of the hospital eye services, and the convenience of health care delivery at the local level, part of glaucoma care is likely to be transferred to optometrists.
The quality of referrals of patients with glaucoma from community optometrists to hospital eye services has been reported in several studies. A substantial proportion of possible glaucoma patients were false positives. In the largest study reported to date, that of Bowling et al,21 nearly half (45.8%) of all patients referred to a glaucoma clinic were discharged at the first visit. Similar outcomes were observed in other studies.3–6 False positive referrals add an unnecessary workload to busy outpatient departments, incur financial costs, and affect the patients’ wellbeing. None of the reported evaluations of the performance of optometrists estimated the rate of false negatives, which was assumed to be low. In this study the specificity of the glaucoma trained optometrist is high, reducing the false positive referrals to a minimum. The performance of the glaucoma trained optometrist was at least comparable to that of a junior ophthalmologist in assessing new referrals for glaucoma in a general ophthalmology clinic. Data reporting the diagnostic accuracy of community optometrists for glaucoma detection are not available, despite a systematic search of published reports,2 but sensitivity has been estimated at 32% and specificity at 99%.2 These estimates are based on a survey conducted on behalf of the International Glaucoma Association involving 241 optometrists in England and Wales who carried out 275 600 sight tests (equivalent to 5% of the national total) over a six month period in the late 1980s.5
Interventions to improve glaucoma detection rates in the community have been tried with variable success. Vernon and Ghosh found little effect after providing specific referral guidelines to local optometrists.22 However, Patel et al9 proved that ongoing training of optometrists resulted in an increased rate of detection of glaucoma in the community. A community based scheme to improve the referral accuracy of suspect glaucoma cases was also successful.12 Standard glaucoma referrals were passed to trained optometrists for repeat diagnostic testing, with suspect cases then referred on to the HES. The number of suspect glaucoma cases referred to the Manchester Royal Eye Hospital was reduced by 40% and the scheme produced a small financial cost saving to the NHS of approximately £17 per patient. The percentage of false negatives was not known. In Bristol a randomised controlled trial examining community optometric care for monitoring glaucoma patients versus standard hospital care found no difference in terms of health outcome at two years.11 The latter study involved a population of known glaucoma patients already attending the hospital eye service. A costs analysis found the community service, including costs of referral back to hospital for cases of uncertainty, was more expensive than standard hospital care.
In the present study two different aspects of the performance of accredited glaucoma optometrists have been assessed: diagnosis and indications for treatment. The gold standard was the judgment of an experienced consultant ophthalmologist. Overall, the agreement between optometrists and the consultant ophthalmologist was high, supporting the current role of trained glaucoma optometrists in the detection of glaucoma and the initiation of treatment. Most disagreements occurred at the lower end of the severity scale (normal and suspect/OHT requiring review). These disagreements may not have clinical relevance for patients, although unnecessary review of suspect cases would increase the cost of the service. Two patients requiring urgent referral were correctly identified. Among patients with glaucoma requiring non-urgent referral (n = 23), two were missed by the optometrists and three by junior doctors. The effect of further training, increased clinical experience, or more detailed guidelines to avoid such disagreements is unknown but it is likely that the agreement would improve. From the clinical point of view, accredited glaucoma optometrists could potentially manage and treat patients with ocular hypertension in the community without their needing to attend the hospital eye service. Another advantage of this scheme is that patients diagnosed with glaucoma would start treatment immediately while waiting to be seen at the hospital eye service. The quality of care would be at least as good as that provided by junior doctors in the outpatient department. However, it is possible that specialist training in glaucoma would also improve the performance of trainees.
To our knowledge, this is the only study that has evaluated the performance of trained glaucoma optometrists and included the rate of false negatives in a community setting. Banes et al14 have recently reported good agreement on clinical management decisions between optometrists and consultant ophthalmologists in a hospital based setting. Our study has the strengths of having used a clinical examination of each patient carried out by a consultant rather than relying on the medical records, and having evaluated the actual practice of accredited glaucoma optometrists working in the community. Although the AGOs knew that the study was in progress they were unaware of which patients would be involved. The study design was strong in that all participants were assessed by all three categories of health professionals and as such provide a direct comparative estimated of the reliability of the management decisions. Additionally, the study also provides comparative diagnostic accuracy estimates of the performance of optometrists compared with junior ophthalmologists. There are limitations in that a true reference standard for glaucoma would be best provided by a longitudinal follow up. However, such a cohort study would need many years of follow up. Under the circumstances, expert opinion was the most feasible and best reference standard available.
Community optometrists trained in the glaucoma are potentially a very valuable resource for the detection and management of glaucoma, and indeed of other significant eye diseases.23 24 Access to community optometrists is easy and they help to reduce the demand on stretched hospital eye services. In this study not only was the detection of glaucoma satisfactory overall but so were decisions regarding management and the initiation of treatment. With additional training in glaucoma, optometrists are at least as accurate as junior ophthalmologists, but some cases of glaucoma are missed. It is possible that with further clinical experience the performance of the optometrists would improve.
There are potential disadvantages of an optometrist based scheme such as the possible increased cost of health care (for example, in a fee-per-service contract), or the cost of purchasing spectacles, which could deter some people from attending for testing. Given limited health care resources the cost-effectiveness of establishing such a service across the United Kingdom needs to be compared with alternative strategies and current hospital based care.
Acknowledgments
The Health Services Research Unit is supported by a core grant from the Chief Scientist Office of the Scottish Executive Health Department. The views expressed are those of the authors and are not necessarily shared by the funders. We thank Mrs Pat Peacock, glaucoma co-ordinator, for her assistance in this project.
REFERENCES
Footnotes
Competing interests: None declared.
- Abbreviations:
- AGO
accredited glaucoma optometrist
- HES
hospital eye service
- IOP
intraocular pressure
- OAG
open angle glaucoma