Article Text

Abstract
Aim: To describe an alternative and novel technique using cyanoacrylate glue to achieve successful limbal tissue dissection, from an organ culture media stored corneoscleral button, without an artificial anterior chamber.
Methods: A donor corneoscleral button (leftover from penetrating keratoplasty) was divided into two equal semicircular halves. A thick layer of tissue adhesive (N-butyl-2-cyanoacrylate) was spread on a sterile rubber block (the under surface of the donor punch). One half of the donor corneoscleral rim was placed epithelial side up on the adhesive and allowed to attach firmly to the block. This composite provided stability to the donor rim allowing lamellar dissection of the limbal tissue to be performed without damaging the limbal epithelium.
Results: Regular, partial-thickness limbal tissue was obtained. There was no histological evidence of glue or cellular toxicity of the harvested limbal stem cells. This harvested tissue had been grafted successfully in patients with limbal stem cell deficiency also undergoing keratoplasty.
Conclusions: Tissue adhesive can be a simple, effective and useful tool in the dissection and harvesting of corneal limbal stem cell allografts from corneoscleral buttons stored in organ culture media.
Statistics from Altmetric.com
Allo-grafting corneal limbal stem cells requires a whole globe for dissection of donor limbal tissue inclusive of stem cells. Dissecting the limbal tissue from a corneoscleral button is technically difficult without an artificial anterior chamber. Here we describe an alternative and novel technique using cyanoacrylate glue to achieve successful limbal tissue dissection without an artificial anterior chamber.
AIM
The aim here is to describe an alternative and novel technique using cyanoacrylate glue to achieve successful limbal tissue dissection, from an organ culture media stored corneoscleral button, without an artificial anterior chamber.
DESIGN
This is a prospective innovation of surgical technique to harvest coneal limbal stem cells effectively and with ease to treat patients with limbal stem cells deficiency.
METHODS
Surgical technique
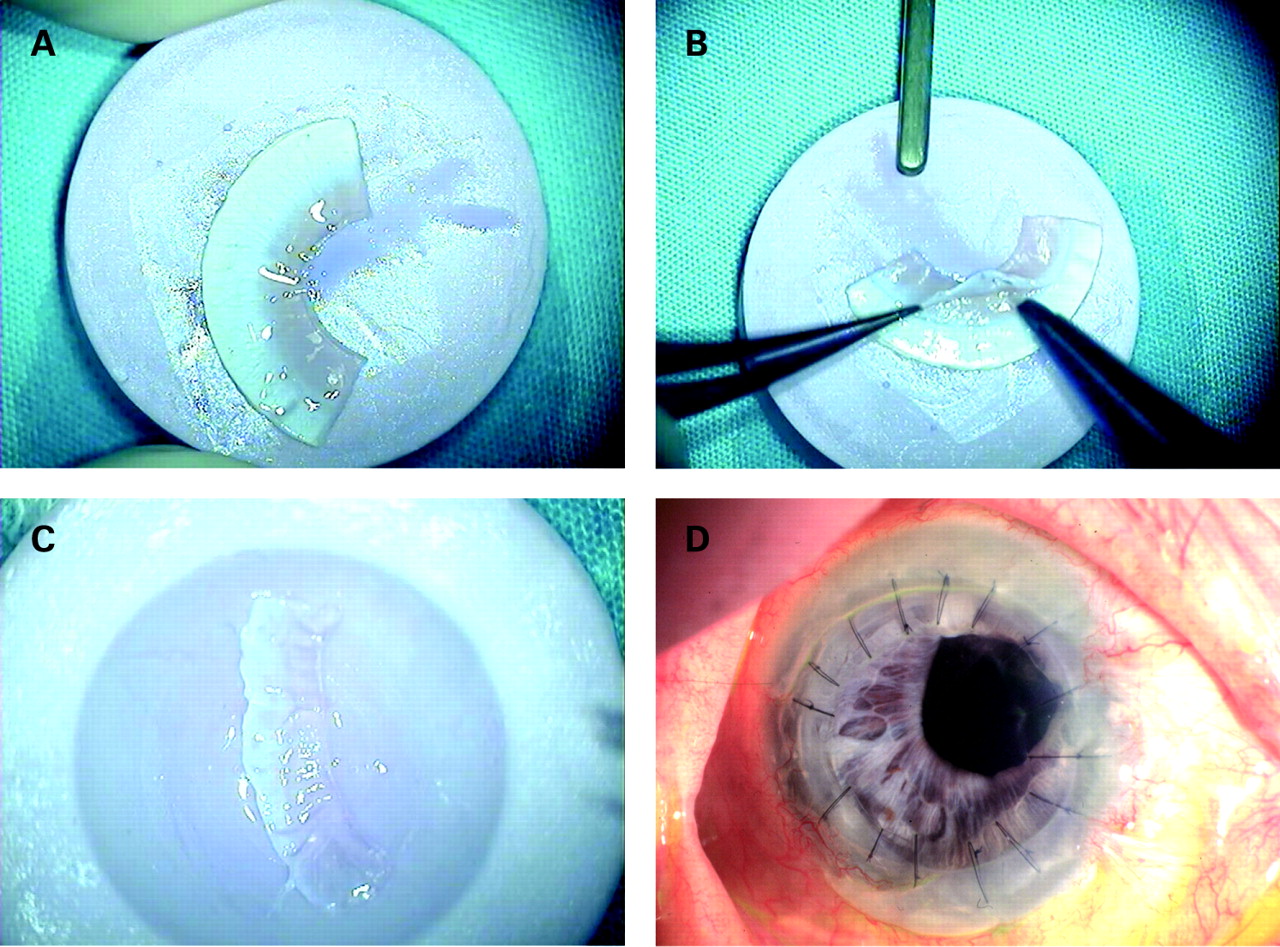
The central cornea from a donor corneoscleral button is initially removed, and the residual tissue is divided into two equal semicircular halves. A thin layer of tissue adhesive (N-butyl-2-cyanoacrylate) is spread on a sterile rubber block (the under surface of the donor punch). One half of the donor corneoscleral rim is placed epithelial side up on the adhesive and allowed to attach firmly to the block (fig 1A). This composite provides stability to the donor rim allowing lamellar dissection of the limbal tissue up to 80% of full thickness depth, to be performed without damaging the limbal epithelium (fig 1B) (technique by KR).
{kind=link}
RESULTS
Regular, partial thickness limbal tissue was obtained (fig 1C). There was no histological evidence of glue or cellular toxicity of the harvested limbal stem cells. This harvested tissue had been grafted successfully in four patients with limbal stem cell deficiency who also had penetrating keratoplasty. Two of these patients had ocular cicatricial pemphigoid, one had ocular chemical burns, and the other one had Stevenson–Johnson Syndrome. All these patients maintained clear corneal grafts beyond 6 months postoperatively, up to 18 months’ follow-up (fig 1D).
Histology studies on sections of the corneal limbal stem cells harvested using the method mentioned showed that on all four occasions, there was no evidence of cyanoacrylate glue on any of the harvested sections and that the limbal stem cells were intact. This implies that this method is safe.
DISCUSSION
Limbal stem cell deficiency requires repopulation of the debilitated limbus with a viable stem cell population. This can be achieved through limbal tissue transplantation or transplantation of limbal stem cells expanded in vitro. It is relatively easy to dissect limbal tissue from a whole globe. However, the current practice of harvesting and distributing corneas from eye banks has its limitations, and a whole globe is seldom available for limbal tissue transplantation. We may therefore have to rely on corneal limbal tissue to harvest limbal tissue with its stem cell population.1–3 Dissecting limbal tissue from an unstable corneoscleral button is technically demanding.4 5 Alternative techniques have been described to stabilise the corneoscleral button. Mannis et al described a method using a standard silicone orbital sizing sphere and three 25-gauge needles to fix the corneoscleral button.4 Another method described used an acrylic sphere mounted on a polyvinylchloride cylinder with a hexagonal shaped footing with holes at each corner through which a needle and suture could be threaded and the donor cornea fixed. The donor cornea was then trephined to leave behind a 1 mm rim surrounding the limbus, cyanoacrylate tissue adhesive placed on the posterior side of the corneoscleral rim and the sphere to stabilise it, and the keratolimbal stem cell was then harvested using a Number 65 Beaver blade.6
Our novel technique described is safe and easy to perform. Cyanoacrylate tissue adhesive appears to be a useful, practical, cost-effective tool in the dissection of corneal limbal stem cell allografts from corneoscleral buttons stored in organ culture media. It can facilitate harvesting of corneal limbal stem cells in any standard operating theatre.
Footnotes
Competing interests: None.