Article Text

Abstract
Aim: To study time trends in the incidence of conjunctival melanoma in Sweden.
Methods: All patients with conjunctival melanoma from 1960 to 2005 in Sweden were identified through the Swedish Cancer Registry, cross-checked against hospital files, and validated by histopathological review (97.5%) or detailed hospital records (2.5%). The crude and age-standardised incidences were estimated separately for each sex and the annual change in incidence over time was estimated using a regression model with logarithmic incidence numbers. Time trends for the largest diameter, thickness and location of the tumour when diagnosed were analysed.
Results: The age-standardised incidence of conjunctival melanoma increased significantly in men (n = 89) from 0.10 cases/million to 0.74 cases/million (p = 0.001) and in women (n = 81) from 0.06 cases/million to 0.45 cases/million (p = 0.007). The annual relative change in age-standardised incidence was 16.9% (95% confidence interval (CI) 12.2 to 21.6) in men and 19.5% (95% CI 9.3 to 29.7) in women. The age-specific incidence was higher in men and women ⩾65 years (1.48 and 1.39 cases/million, respectively) than in younger men and women (0.3 and 0.2 cases/million, respectively). During the period of study, tumours became smaller (p = 0.005) and thinner (p = 0.002) at the time of diagnosis and increasingly arose from parts of the conjunctiva exposed to ultraviolet radiation (p = 0.001).
Conclusion: The incidence of conjunctival melanoma increased in Sweden during the period 1960 to 2005.
Statistics from Altmetric.com
Conjunctival melanoma arises from melanocytes lodged in the basilar layer of the conjunctival epithelium and causes death in 30% or more of the patients.1 Conjunctival melanoma is distinctly uncommon and though 95% of all melanoma cases are cutaneous and 3–4% of tumours occur in the eye, only about 5% of melanoma arising in the ocular region has a conjunctival origin.2 Population-based studies indicate that the incidence of conjunctival melanoma is probably within the range 0.024–0.08 per 100 000.123456
Given recent advances in the epidemiology and molecular biology of conjunctival melanoma, it now seems likely that the molecular mechanisms driving conjunctival melanoma tumourigenesis are more akin to those of cutaneous and mucous membrane melanoma than those of melanoma arising in the uveal tract.13478 Specifically, the incidence of cutaneous melanoma is increasing by 4–5% annually in the Western world; this rise is being attributed largely to increased exposure to ultraviolet radiation (UVR).69 The uvea is largely protected from UVR exposure, and uveal melanoma incidence rates appear to be stable or even declining.10 Interestingly, large parts of the conjunctiva are exposed to UVR and recent studies suggest that conjunctival melanoma incidence rates may be rising and parallel those of cutaneous melanoma.34
Materials and methods
The criteria for inclusion were patients with primary conjunctival melanoma, diagnosed in Sweden 1960 through 2005, with the diagnosis validated by histopathological review by a trained ophthalmic pathologist or by detailed hospital records including clinical photographs or drawings. The Swedish National Cancer Registry, founded in 1958, receives reports when a malignant disease is diagnosed. Compulsory dual registration from a clinician and a histopathologist or cytopathologist ensures a high inclusion rate. Each patient is identified through a unique national registration number, and the registry is estimated to include more than 95% of all cases of cancer in the country.11 These data were combined with those of the Swedish Ocular Oncology Service and Eye Pathology Laboratory based at Karolinska University Hospital until 1990, and thereafter at St Eriks Eye Hospital in Stockholm. This tertiary referral centre manages nearly all cases of conjunctival and uveal melanoma in Sweden.
Files from the Swedish National Cancer Registry during the period 1960 to 200512 were searched for patients with conjunctival melanoma, using both the International Classifications of Diseases, and the Seventh, Eight, Ninth and Tenth Revision (ICD-7, ICD-8, ICD-9 and ICD-10) code and the Systematized Nomenclature of Medicine (SNOMED) code. All the patients reported from Cancer Registry were cross-checked against the files of the Ocular Oncology Service and Eye Pathology Laboratory based in Stockholm. Data on the Swedish population were collected from the Statistics Sweden.13
During the study period, 170 cases of conjunctival melanoma were registered with the Swedish National Cancer Registry. A histopathological review of archival tissue indicated that 21 cases were erroneously classified as conjunctival melanoma, as follows: ten cases were choroidal melanoma, five iris melanoma, three ciliary body melanoma, two cutaneous melanoma and one case was a breast cancer. In addition, 14 patients were classified as conjunctival melanoma with the Swedish National Cancer Registry but as there no hospital records or histopathological samples to validate this, all 35 cases were excluded from this study, leaving 135 patients with conjunctival melanoma filed with the Swedish National Cancer Registry 1960–2005.
When searching our local pathology and hospital files, 151 patients with conjunctival melanoma were found; 116 of these matched the files of the Swedish National Cancer Registry but 35 cases not previously registered were disclosed and formally notified. Hence, the Swedish National Cancer Registry’s non-inclusion rate of conjunctival melanoma was 20.6%. The 35 cases not previously registered were added to the 135 validated cases from the Swedish Cancer Registry leaving 170 patients with conjunctival melanoma to be included in this study; 166 (97.5%) of these were confirmed by histopathological examination and four (2.5%) by detailed hospital records only. The size of each tumour was assessed from clinical photographs by two independent observers. The pathological grading and histological grade were assessed (tables 1 and 2). Most tumours were bulbar and multifocal (table 3).
Pathological staging of primary tumour according to AJCC cancer staging manual, seventh edition (2009)19
Histological grade of primary tumour according to the AJCC cancer staging manual, seventh edition (2009)19
Location of conjunctival melanoma
Each sex was analysed separately and the patients were divided into eight age groups, each spanning 10 years, except the youngest (0–24 years) and the oldest (>85 years) age groups. The analysis over time was performed for 5-year periods from 1960 except the period 2000 to 2005.
An overall crude and age-standardised incidence rate in the total Swedish population was calculated, and the sexes were further analysed separately. Age-standardisation of incidence numbers over the study period was performed by a direct method, with the Swedish population during the period 1970 to 1974 taken as a standard according to the stratum weights shown in table 4. The relative change in incidence over the 46-year period was calculated by linear regression after logarithmic transformation of incidence data. The annual change was expressed as a percentage with 95% confidence intervals (CI). A similar regression model was used to estimate time trends in the largest diameter, thickness and location of the tumour when diagnosed. Tumour location was coded as conjunctiva chronically exposed to ambient solar radiation and hence UVR (most of the bulbar and limbal and all caruncular conjunctiva) or as conjunctiva with minimal UVR exposure (tarsal and forniceal conjunctiva). The level for statistical significance was a set at p<0.01. Data were processed with statistical analysis software (SPSS, ver. 15.0; SPSS Inc., Chicago, Illinois, USA).
Stratum weights of the Swedish population during the period 1970 to 1974
Results
A total of 170 patients were found to have conjunctival melanoma in Sweden during the period 1960 to 2005 after searching the Swedish National Cancer Registry and the files of the Swedish Ocular Oncology Service and Eye Pathology Laboratory. These patients included 89 men and 81 women (male to female ratio: 1.09). The men were 20 to 99 years of age (mean 62 years; median 63 years) and the women were 22 to 91 years of age (mean 67 years; median 75 years) at the time of diagnosis. Notably, all patients were ⩾35 years of age at the time of diagnosis with the exception of two patients (fig 1).

The age distribution of conjunctival melanoma in the Swedish population during the period 1960 to 2005.
The age-specific incidence for men and women increased gradually from the 35–44-year-old group (0.49 and 0.19 cases/million, respectively) to a peak for the group >85 years of age at the time of diagnosis (3.27 and 2.95 cases/million, respectively). The age-specific incidence was higher in men and women ⩾65 years (1.48 and 1.39 cases/million, respectively) than in men and women younger than 65 years of age (0.3 and 0.2 cases/million, respectively) at the time of diagnosis (fig 2).

Age-specific incidence rates of conjunctival melanoma in the population of Sweden during the period 1960 to 2005.
During the period 1960 to 2005, the overall age-standardised incidence of conjunctival melanoma in the Swedish population increased sevenfold, from 0.08 cases/million to 0.56 cases/million (p = 0.001). In the male population, the age-standardised incidence increased from 0.10 to 0.74 cases/million (p<0.001) and this was paralleled by a similar increase among women from 0.06 to 0.45 cases/million (p = 0.007) during the period of study (fig 3). By applying a log-regression model, we determined the annual change in incidence rate. The male incidence increased by 16.9% (95% CI 12.2 to 21.6) per year and the female incidence increased by 19.5% (95% CI 9.3 to 29.7) per year from 1960 to 2005. The total annual change in incidence for both sexes combined was 17.1% (95% CI 11.2 to 23.0).

Annual age-standardised incidence compared with the observed incidence in the Swedish population for (A) men, (B) women and (C) both sexes combined during the period 1960 to 2005. Solid line, observed incidence; grey line, age-standardised rates when standardised against the Swedish population of 1970 to 1974.
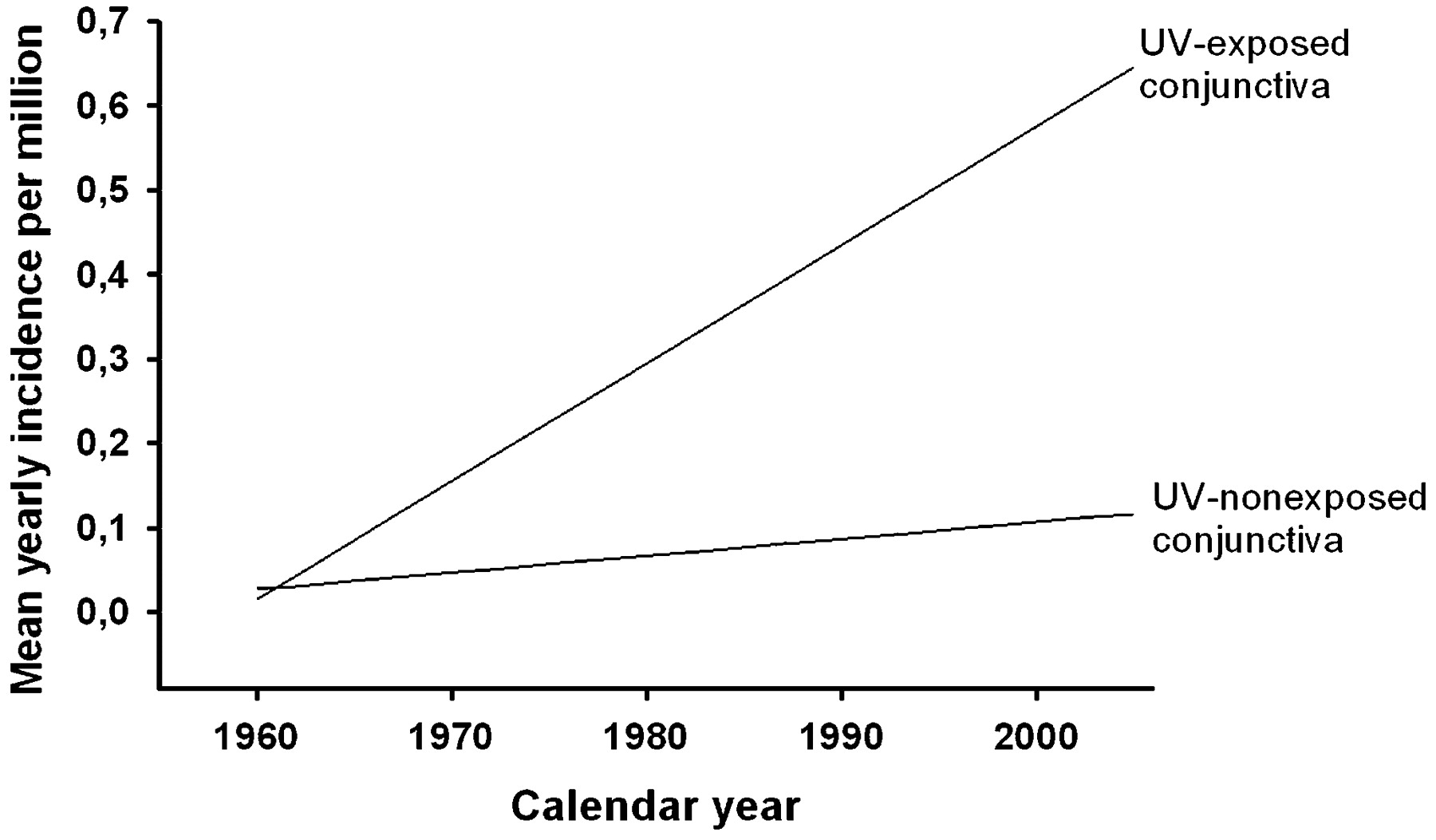
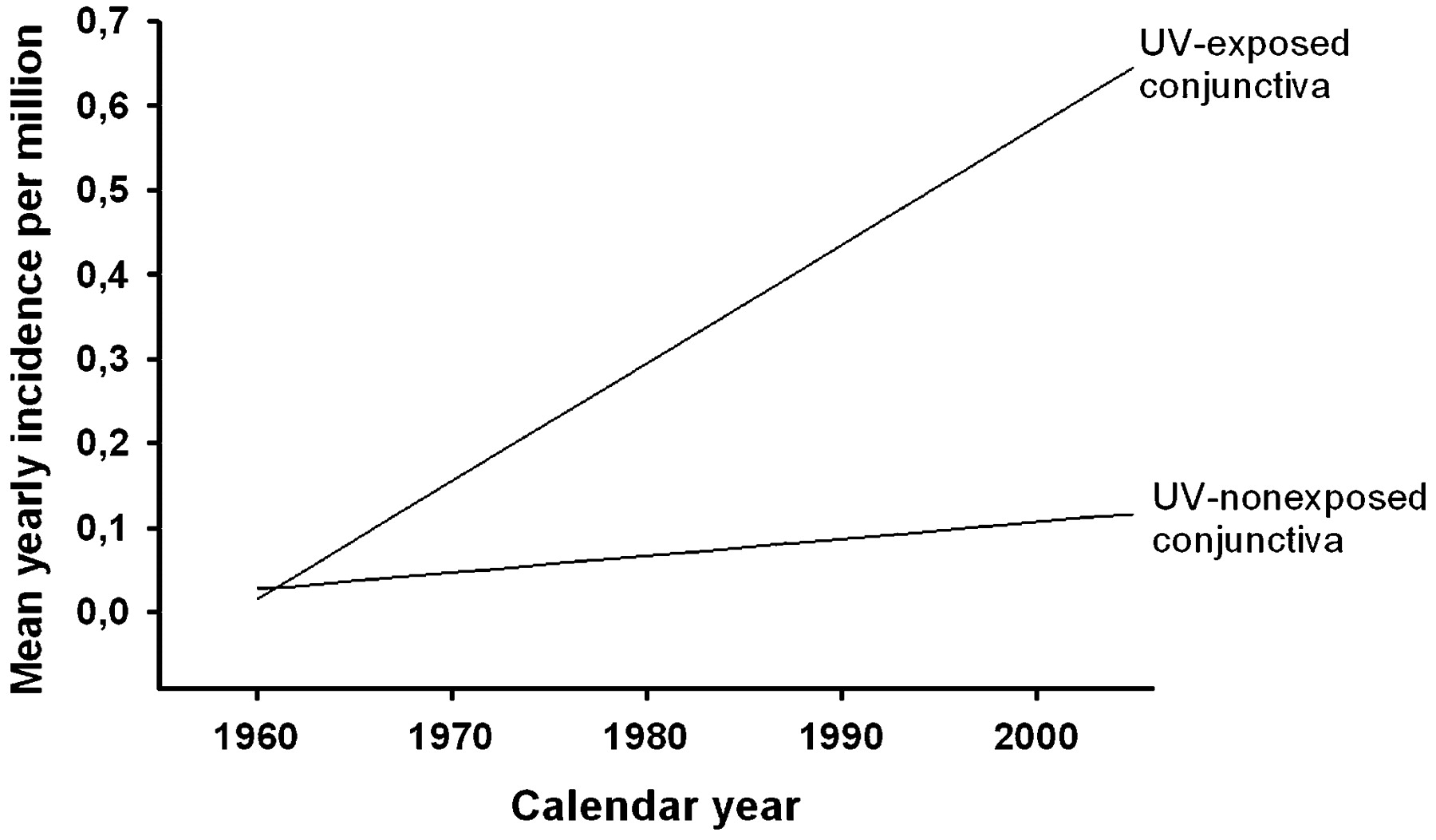
By logarithmic regression, the largest tumour diameter at the time of diagnosis decreased from 11 to 8 mm (p for slope = 0.005) and tumour thickness decreased from 2.5 to 1.0 mm (p for slope = 0.002) during the period of study. Most of the increase in conjunctival melanoma incidence could be attributed to melanoma becoming more frequent in bulbar parts of the conjunctiva exposed to ultraviolet radiation (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Model-based fitted values with linear regression shown no significant increase in conjunctival melanoma arising from conjunctiva protected from UVR (p for slope = 0.275), but tumours arising from conjunctiva exposed to UVR increased (p for slope <0.001) during the period of study. The difference between slopes was statistically significant (p = 0.001). The total number of cases of UVR-exposed conjunctival melanoma was 134. The number of UVR-non-exposed conjunctival melanoma was 33. In three cases it was not possible to identify completely the location of the tumour.
Discussion
This study demonstrates a dramatic and statistically significant increase in the incidence of conjunctival melanoma in Sweden 1960 to 2005. Are these results correct? There have been two recent studies on time trends in conjunctival melanoma incidence based on very similar but not identical datasets from the National Cancer Institute’s Surveillance Epidemiology and End Results (SEER) program. The SEER database covered approximately 14% of the population of the USA in 1992.9
One of the previous studies based on the SEER database detected 153 cases of conjunctival melanoma during the period 1974 to 1998;9 the other found 206 cases when including only two more years, from 1973 to 1999.3 Whilst the first study failed to detect a statistically significant increase in conjunctival melanoma incidence,9 the second study detected a biennial increase of 11.2% (95% CI 6.3 to 16.3) in White men.3 Remarkably this rise was not seen in women. In contrast, the study reported herein is the first to demonstrate a statistically significant increase in the incidence of conjunctival melanoma for both men and women with no apparent sex difference. Similarly, a previous study found no difference between sexes, suggesting that in Finland, the rise in conjunctival melanoma incidence largely parallels the increase seen in cutaneous melanoma incidence.4
A rise in cutaneous melanoma incidence is apparent in many Western countries and in Sweden a 5% annual increase has been reported during 1976 through 1994.14 Notably, the 17.1% (95% CI 11.2 to 23.0) annual increase of the incidence we report is more than three times the rise in cutaneous melanoma incidence in a near identical population.14 There are many potential flaws to consider before accepting this sharp rise in incidence. First, the registration may have been incomplete during the early years of the study, giving rise to ascertainment bias. However, the proportion of cases validated by histopathological examination remained high throughout the period of study reported herein. In addition, data derived from both types of sources (National Registry and Ocular Oncology Centre) included in this study showed a similar trend with incidence rising from 1970 and reaching a plateau after 1990. Interestingly, this plateau parallels the levelling off noticed for cutaneous melanoma incidence in northern Europe since the mid 1990s.15
Second, the incidence of conjunctival melanoma in Sweden during the first period of the study (from 1960 to the mid 1970s) was lower (0.08 to 0.20 cases/million) than the crude annual incidence reported from neighbouring countries such as Finland, with a mean of 0.4 cases/million,4 or Denmark, with 0.45 cases/million.6 The low incidence seen in Sweden until the mid 1970s would somewhat accentuate the rise in incidence seen in later years.
Third, because the incidence of conjunctival melanoma differs markedly between ethnically different populations,16 a rising incidence occurring through a long period of time could be (partially) explained by an ethnicity shift of that population. The SEER population includes 14% of the US population and is more much more ethnically heterogeneous (including higher proportions of Blacks and Hispanics with a lower incidence rate) than the Swedish population, which like the Finnish population is largely made up of Whites.16 Notably, there has been a small but growing immigration from both European and non-European countries to Sweden in the past few decades.14 However, the net immigration rate remains comparatively low: the Swedish rate is estimated at 0.86/1000 population compared with 3.5/1000 population for the USA during 2000.17 Data from the Swedish National Bureau of Statistics indicate that the proportion of the population of non-European origin in 1960 was 0.2% and in 1998 had increased to 4.0%.18
Fourth, diverse factors might explain the increase of reported cases to the Swedish National Cancer Registry during the recent decades as, for instance, health awareness of the population or a higher accessibility to ophthalmological examination through the expansion of cataract surgery and screening programmes for diabetic retinopathy that has been introduced in the last 25 years. However, only very small subsets of the Swedish population have annual ophthalmological follow-up. The statistically significant decrease of the largest tumour diameter and tumour thickness we noted is consistent with lesions being diagnosed at an earlier stage in recent years, but even so this is insufficient to fully account for the increase in overall incidence observed throughout the 46-year period of the study.
Increased intermittent UVR exposure through ambient sunlight has been directly implicated in the significant rise in cutaneous melanoma incidence apparent in fair-skinned societies.15 Not much evidence is available on the pathogenesis of conjunctival melanoma, but as most of the conjunctiva is UVR-exposed, it is conceivable that any rise in conjunctival melanoma incidence could be attributed to similar molecular mechanisms as in the pathogenesis of cutaneous melanoma.2 Interestingly, the rise in conjunctival melanoma incidence we have shown in this study could largely be attributed to conjunctival melanoma occurring more frequently in conjunctiva exposed to UVR. Similarly, there was no detectable increase in conjunctival melanoma arising from the tarsal conjunctiva (outlining the inner surface of the eyelids) with minimal sunlight exposure. Taken together with the time trend, this suggests that UVR exposure may play a major part in the pathogenesis of conjunctival melanoma.
REFERENCES
Footnotes
Funding Supported by grants from Karin Sandqvist’s Foundation for the Visually Impaired, St Eriks Eye Research Foundation and the Swedish Research Council.
Competing interests None declared.
Provenance and Peer review Not commissioned; externally peer reviewed.
Ethics approval The research protocol for the present study was approved by the Human Ethics Committee at the Karolinska Institute, in accordance with the statutes of the World Medical Association’s Declaration of Helsinki.
Linked Articles
- At a glance