Article Text

Abstract
Aims To describe the conjunctival epithelial features seen with in vivo confocal microscopy (IVCM) after gold micro shunt (GMS) implantation in the suprachoroidal space, in patients with uncontrolled glaucoma.
Methods This was an observational case series study. Fourteen eyes of 14 consecutive glaucomatous patients with a history of multiple failed incisional surgeries followed by GMS implantation were evaluated with a digital confocal laser-scanning microscope (HRT II Rostock Cornea Module). Patients were divided into two groups: successful implantations (Group 1: eight patients, eight eyes), defined as a one-third reduction in preoperative intraocular pressure (IOP) with or without antiglaucoma medications and failed implantations (Group 2: six patients, six eyes) as a less than one-third reduction in preoperative IOP with maximal tolerated medical therapy. The examination was performed from 3 to 20 months (mean 15.4±5.4) postoperatively. Conjunctival mean microcyst density (MMD: cysts/mm2) and mean microcyst area (MMA: μm2) were the main outcome measurements.
Results The mean postoperative IOP was statistically different between the two groups (p<0.05), with the values of 14.3±2.77 and 32.3±8.01 mm Hg in Groups 1 and 2, respectively. When comparing successful with failed implantation, the IVCM analysis showed a greater MMD (p<0.01) and MMA (p<0.01). Clinical evidence of filtering bleb was not found in any of the patients.
Conclusions Successful GMS implantation significantly increased conjunctival microcysts density and surface at the site of the device insertion. These findings suggest that the enhancement of the aqueous filtration across the sclera may be one of the possible outflow pathways exploited by the shunt.
- Conjunctiva
- trans-scleral outflow
- suprachoroidal space
- gold micro shunt
- in vivo confocal microscopy
- primary open-angle glaucoma
- aqueous humour
- intraocular pressure
- imaging
- treatment surgery
Statistics from Altmetric.com
- Conjunctiva
- trans-scleral outflow
- suprachoroidal space
- gold micro shunt
- in vivo confocal microscopy
- primary open-angle glaucoma
- aqueous humour
- intraocular pressure
- imaging
- treatment surgery
Introduction
To date, filtration surgery and drainage device implantation are the most reliable procedures for lowering the intraocular pressure (IOP) in patients with medically uncontrolled glaucoma.1–4 The basic mechanism of these procedures is the creation of a new drainage route which allows aqueous humour to drain from the anterior chamber, thereby circumventing the pathological outflow obstruction. The aqueous then flows directly or indirectly into subconjunctival spaces leading to an elevation of the conjunctiva at the surgical site, which is commonly referred to as a filtering bleb.5 6
In a variable percentage of patients, either filtration procedures or drainage device implantation can lead to significant postoperative complications such as bleb leaks, hypotony, blebitis, endophthalmitis and bleb encapsulation, the latter being widely recognised as the main cause of surgical failure.7 8 Intense clinical and instrumental analysis of the bleb with frequent postoperative management still represents the main challenge in the maintenance of long-term surgical success of all available filtration surgical procedures.
In the last years, bleb-less surgical approaches which exploit and enhance alternative aqueous outflow pathways have been evaluated in order to avoid these complications.
One such procedure involves the use of gold micro shunt (GMS) devices which are 24-carat gold, biocompatible flat plates containing micro-tubular channels that create a bridge between the anterior chamber (AC) and suprachoroidal space, thus, forcing aqueous flow through the two compartments, taking advantage of the natural gradient of hydrostatic pressure (from 1 to 5 mm Hg) between the AC and suprachoroidal space, respectively.9 Hence, aqueous humour is removed via the choroidal vascular system or by gradually flowing through the scleral layers and then the conjunctiva, without the creation of a bleb. Recently, Melamed et al10 evaluated the efficacy and safety of GMS implantation in the supraciliay space in failed incisional glaucoma surgery, reporting a 79% surgical success, without relevant postoperative complications and without the formation of filtering bleb in any of the patients. However, to the best of our knowledge, no reports have specifically focused on the possible aqueous outflow pathways exploited by the GMS device.
The aim of the present study was to describe the bulbar conjunctival features in glaucomatous patients who underwent GMS implantation by using in vivo confocal microscopy (IVCM), in order to elucidate modifications induced by this device.
Material and methods
This was an observational case series study. The study adhered to the tenets of the Declaration of Helsinki, and informed consent was obtained from all patients prior to their enrolment. Our local Ethics Boards were notified, which determined that their approval was not necessary. We examined 14 eyes (eight right and six left eyes) of 14 consecutive Caucasian patients affected with primary open-angle glaucoma (POAG) who had been referred to the Ophthalmic Clinics of the Universities of Chieti-Pescara and Pisa, Italy (eight males and six females, with an age range from 43 to 77 years, mean 64.6±11.8). All patients had a history of multiple failed incisional procedures, followed by GMS implantation (SOLX, Boston, Massachusetts) from 10 to 14 months after the last failed surgery.
The number of failed procedures prior to GMS implantation ranged from 1 to 2 (mean 1.4±0.5) and corresponded to MM-C augmented trabeculectomy (14 procedures) or deep sclerectomy with T-Flux implant (six procedures).
The GMS was inserted in the superior-temporal (nine eyes) or superior-nasal (five eyes) region, as indicated on a patient-to-patient basis in order to avoid inadvertent intraoperative manipulations of the sites used in previous procedures. To comply with this intention, the conjunctiva overlying the site of the previous failed filtration procedure close to the planned site for GMS insertion was preoperatively marked (Methylene Blue) 2–3 mm outwardly to the limits of the presumed scleral flap. Therefore, the conjunctival flap and the scleral dissection for the GMS implantation were created at least 2 mm from the delimited area.
A detailed description of the shunt and surgical technique has been previously reported.10
The time range of postoperative examinations was 3 to 20 months (mean: 15.4±5.4 months) after GMS implantation.
Each patient, after a complete ophthalmological assessment including visual acuity, applanation tonometry, anterior segment slit-lamp evaluation with particular attention at the conjunctiva overlying the site of implantation (a set of reference photographs was obtained in all cases) and funduscopy, was carefully examined with a digital confocal laser-scanning microscope (LSM) (HRT II Rostock Cornea Module, Heidelberg Engineering, Germany). Additionally, in order to verify the correct position of the proximal and distal end of the GMS implant, each patient underwent gonioscopy and anterior segment optical coherence tomography (AS-OCT) (Carl Zeiss Meditec, Dublin, California).
According to the achievement of satisfactory postoperative IOP control and on evidence of surgery success,11 GMS implantations were classified in two groups: successful implantations (qualified and complete success) (Group 1; defined as a third reduction in preoperative IOP with or without antiglaucoma treatment12) and failed implantations (Group 2; as a reduction lower than a third in preoperative IOP in maximal tolerated medical therapy).
All the patients had been on preserved topical antiglaucoma medications; the mean duration of topical therapy and the drug regimen before GMS implantation in each group are reported in table 1.
Patient demographic and clinical characteristics
During the 3 months before IVCM examination, none of the patients received systemic or topical therapy (steroids) which could modify ocular hydrodynamics.
In vivo confocal microscopy
The technical characteristics of the instrument and the details of conjunctival examination were previously described.13 In this case series, we investigated the microscopic epithelial features of the bulbar conjunctiva overlying the location of the GMS implantation.
In order to avoid in the field of analysis the site of the previous surgery close to the device location, we marked (using Methylene Blue) the margins of the conjunctiva overlying the site of the GMS implantation (delineating a 4×5 mm area (20 mm2), at least 2–3 mm from site of the previous surgery) and performed the IVCM at the centre of the selected area (2×3 mm (6 mm2)).
IVCM analysis of each eye was performed by a single operator (VF) who selected six images (from about 40 images) which were evaluated, and the results averaged by a second IVCM operator (LA). Both operators were masked for patient surgical history and status.
The patient was seated in front of the microscope, with their head steadied by a headrest and the eye properly aligned using a dedicated target mobile bright red light provided with the instrument that the patient had to fix with the fellow eye, in order to obtain a tangential optical section of the superior bulbar conjunctiva. A digital camera was used to obtain am image of the lateral view of the eye and objective lens in order to check the position of the latter on the surface of the eye for each scan. The LSM objective was gently positioned in contact with the ocular surface separated by a PMMA (polymethyl methacrylate) contact cap, and a drop of 0.2% polyacrylic gel (Viscotirs Gel, CIBA Vision Ophthalmics, Marcon, Venice, Italy) served as coupling medium. Sequential images 300×300 μm in size derived from automatic scans and manual frames were acquired at the intermediate layer of the bulbar conjunctival epithelium (10 to 20 μm), 2 mm from the limbus at the centre of the corresponding site of the GMS implantation, with the eye in opposite gaze with respect to the site of the implant.
For the IVCM assessment, we evaluated the microcysts in the bulbar conjunctival epithelium, as first reported in the conjunctival wall of functioning filtering blebs.14–17 The main parameters considered were the mean microcyst density (MMD) (cysts/mm2) and the mean microcyst area (MMA) (μm2). The total surface area of epithelial microcysts was calculated in each of the six selected confocal images by means of ImageJ, an open source software (http://rsb.info.nih.gov/ij), using previous described methods.15
Statistical analysis
Statistical analysis was performed using SPSS Advanced Statistical 13.0 Software (2005; SPSS, Chicago, Illinois). Differences in age and gender in successful and failed groups at baseline were evaluated using Student t test and χ2, respectively. An unpaired t test was used to analyse pre- and postoperative IOP, pre- and postoperative number of medications, duration of preoperative therapy and time of IVCM assessment after surgery between the two groups.
A paired t test was used to analyse the changes of postoperative of IOP or the number of medications in each group. The U Mann–Whitney test was used to assess differences on conjunctival microcysts density and surface between the two groups.
For the given effect size, the power of the study was 0.81 and 0.82 for microcyst density and area, respectively (Sample Power; SPSS Advanced Statistical 13.0 Software (2005)).
Results
The demographic and clinical data of each group are shown in table 1. No significant differences were found in age, sex, preoperative IOP, follow-up period and time range of postoperative examinations (months) between the two groups. All reported data corresponded to the last follow-up visit (15.4±5.4 months), which matched with the IVCM examination.
The mean overall (Groups 1 and 2) postoperative IOP percentage reduction was 22.6%, from 28.8±3.9 mm Hg to 22.1±10.6 mm Hg (p<0.05).
The mean postoperative IOP was statistically different between the two groups (p=0.002), with values of 14.3±2.8 and 32.3±8.0 mm Hg in Groups 1 and 2, respectively.
In Group 1, the mean IOP decreased from 28.1±5.0 to 14.3±2.8 mm Hg (percentage reduction of 50.6%) (p<0.001), while we did not observe any statistically significant modifications in Group 2.
The drug dose regimen and the duration of preoperative therapy were not statistically different between groups. The mean number of antiglaucoma medications at baseline and at the last follow-up was not statistically different between groups; these values were not significantly modified in the postoperative period in either group: from 2.7±0.9 to 2.2±1.0 in Group 1 and from 3.0±0.6 to 2.8±0.4 in Group 2.
In both groups, the clinical assessment (according to MBGS criteria),18 the evaluation of the set of the reference photographs and the AS-OCT images did not show any evidence of filtering bleb at the current surgical site in any case (figures 1 and 2A,B). In all eyes, as confirmed by gonioscopy and AS-OCT examination, the device was correctly positioned in both the AC and the suprachoroidal space with an appearance of spongy or tight overlying sclera (figures 1 and 2B). Additionally, AS-OCT showed an hypoechoic space posteriorly to the shunt in several successful implantations (figure 1B).
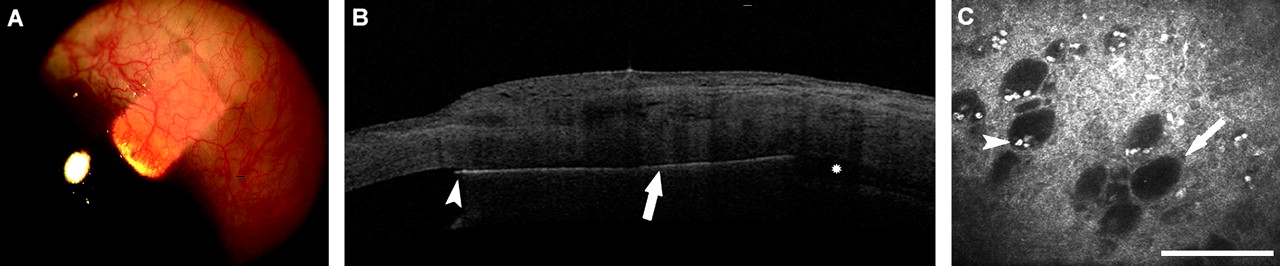
Functioning implantation. (A) Biomicroscopic aspect of a functioning gold micro shunt implant correctly positioned in the anterior chamber (proximal end) and in the suprachoroidal space (distal end). No signs of conjunctival filtering bleb are detectable. (B) Anterior segment optical coherence tomography showing the gold micro shunt in the anterior chamber (arrowhead) and in the suprachoroidal space (arrow), with a spongiform appearance of the overlying sclera and with the hypoechoic space posteriorly to the device (asterisk). (C) In vivo features of conjunctival epithelium at the corresponding area of the device insertion, characterised by intraepithelial microcysts (arrows) partially filled and surrounded by what appear to be inflammatory cells (arrowhead). The bar represents 100 μm.
{kind=link}
{kind=link}
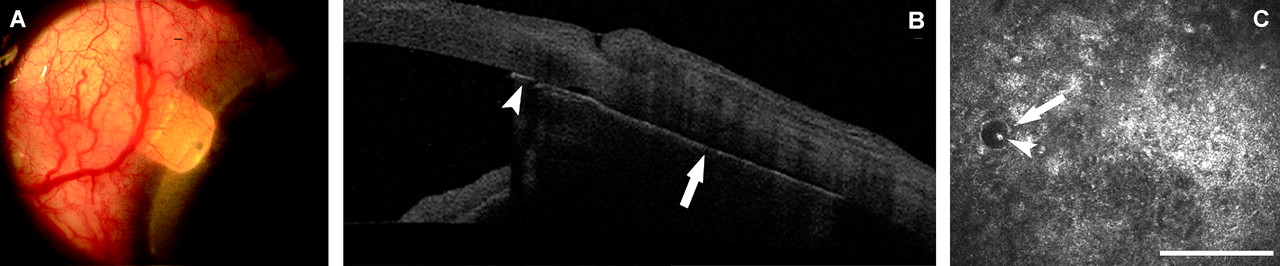
Non-functioning implantation. (A) Biomicroscopic aspect of a non-functioning gold micro shunt implant correctly positioned in the anterior chamber (proximal end) and in the suprachoroidal space (distal end). No signs of conjunctival filtering bleb are detectable. (B) Anterior segment optical coherence tomography showing the gold micro shunt in the anterior chamber (arrowhead) and in the suprachoroidal space (arrow), with a tight appearance of the sclera overlying the device. (C) In vivo aspect of conjunctival epithelium at the corresponding area of the device insertion, showing a diffuse hyper-reflectivity of the layer with one intraepithelial microcyst (arrow) containing what appears to be an inflammatory cell (arrowhead). The bar represents 100 μm.
When analysing the considered IVCM parameters, we found a statistically significant difference between the two groups, either for the microcysts density (cysts/mm2) or for area (μm2) (table 2) (p<0.01). In particular, we did find values of 103.1±22.6 and 29 489.3±12 954.9 and 22.4±11.9 and 4696.0±3608.1 for MMD and MMA in functioning and failed implantations, respectively (figures 1 and 2C).
In vivo confocal microscopy parameters
Discussion
The scarring of conjunctival filtering bleb is the main challenge and limiting factor for long-term IOP control in glaucoma surgery. The bulk of the scientific evidence strongly supports the fact that all antiglaucoma procedures which create a fistula and route aqueous humour from AC to subconjunctival spaces are exposed to a significant risk of bleb scarring and failure over time.8 19 The pathophysiological basis of the bleb scarring appears to be related to the action of a variety of factors present in the aqueous humour of glaucomatous eyes, which are capable of stimulating a fibrotic response after contact with the vascular Tenon tissue.20 Additionally, fibrosis may be mechanically activated by the immediate postsurgical aqueous filtration into the subconjunctival space, as demonstrated after the implantation of Ahmed devices.21
GMS (now commercially available only as the Plus version) is one of the developing surgical procedures which works by shunting fluids from AC to suprachoroidal space, thus avoiding direct and immediate postoperative aqueous outflow into subconjunctiva and the creation of a bleb. In the present study, we analysed the microscopic features of the bulbar conjunctiva at a surgical site with particular attention to intraepithelial microcysts, in patients who underwent uncomplicated GMS implantation after the failure of previous filtration surgeries.
Concerning the postoperative IOP, an average global IOP reduction of 22.6% from baseline was found at the last follow-up (15.4±5.42 months), and all successful patients were classified in qualified success.
These results are quite different with respect to those reported by Melamed et al,10 who found a postoperative IOP decrease and complete success of 32.6% and 13.2%, respectively. Such inconsistency could result from the surgical history of the patients: Melamed et al included in their series patients who had previous glaucoma surgery, a glaucoma drainage device (53%) or patients who did not, while in our series all patients underwent at least one previous filtration surgery and were to be considered refractory glaucoma.
Epithelial microcysts are empty optically clear spaces originally described in the conjunctival bleb wall of successful trabeculectomies, as hallmarks of humour aqueous filtration through the conjunctiva.14 Recently, Amar and colleagues,22 using both impression cytology and IVCM, modified and improved the definition of the bleb wall microcysts, demonstrating that such structures correspond to goblet cells, mostly containing aqueous humour instead of highly hydrophilic gel-forming mucin. Based on these findings, the authors suggested that the transcellular pathway of the aqueous humour could occur at the level of goblet cells towards the ocular surface. More interestingly, in other studies23 24 the presence of intraepithelial microcysts was documented also in eyes affected with untreated ocular hypertension or medically treated POAG that had not undergone surgical procedures. These authors have speculated that these findings support the hypothesis of activation and/or enhancement of alternative hydrodynamic pathways and, specifically, the trans-scleral outflow, in conditions of increased IOP.
In the present study, when comparing functioning with non-functioning implantations, we did find a statistically significant difference for both mean microcysts density and surface, with values approximately fivefold and sixfold higher.
At the biomicroscopic examination, none of the implanted patients developed a postoperative filtering bleb, indicating the absence of a direct postoperative subconjunctival aqueous filtration just as the technique of implantation requires. Therefore, the evidence of conjunctival microcysts at the site of successful GMS implantation might be interpreted as a sign of aqueous percolation through the scleral layers and then the conjunctiva.
As the mean number of postoperative medications did not differ between groups,23 the effects of topical drugs on microcyst density and area were not investigated. Moreover, signs of inflammatory cells were not reported as significant features in the majority of cases, although this aspect was not methodically investigated.
To date, the main mechanisms involved in the IOP reduction after GMS implantation are yet to be determined. However, our results may validate the assumption of Melamed et al,10 who supposed that, once aqueous humour reaches the suprachoroidal space, it drains into the choroidal vascular system or permeates through the sclera. In support of this, the hypoechoic space sometimes observed posteriorly to the functioning implants may indicate the suprachoroidal outflow pathway. Conversely, both the evidence of epithelial microcysts and the spongy appearance of the sclera at IVCM and AS-OCT examinations may be interpreted as the microscopic and macroscopic signs of the supposed activation of the trans-scleral aqueous outflow in functioning GMS shunts.
The pathophysiological basis of this mechanism is most likely an effect of the GMS introduction into the AC. This action technically requires a scleral dissection and, therefore, the creation of a plane of 80–90% scleral thickness. The final result is a partial scleral thinning with a reduction of the trans-scleral fluid movement resistivity which permits aqueous humour to move easier and in larger amounts from suprachoroidal space to subconjunctiva.
In support of this, the importance and role of the scleral thinning in filtration surgery success have been recently demonstrated also in eyes that underwent MM-C augmented trabeculectomy.24
By considering such results, bleb-less surgical approaches which shunt aqueous humour to suprachoroidal space and/or thin the sclera, thus increasing the trans-scleral outflow, could be useful to improve the success of antiglaucoma surgical procedures and avoid the intensive postoperative management.
However, like Melamed et al, we did not calculate the exact contribution of the suprachoroidal aqueous resorption and trans-scleral outflow to the mechanism of IOP reduction.
In non-functioning cases, various mechanisms of failure may be hypothesised. The most relevant could be the formation of a fibrotic capsule around the device isolating the shunt from the choroidal vascular bed and the sclera. Alternatively, a connective invasion and/or an occlusion of the proximal end channels and the distal end holes or both mechanisms should be evoked. The effect is a proximal or a distal blockage of the aqueous outflow, and so reaching and permeating the sclera would be unfeasible. These aspects could justify the very low density of epithelial microcysts at IVMC and the tight feature of the sclera at AS-OCT in failed implantations. Nevertheless, to verify our hypothesis, histological studies aimed at the analysis of the removed shunts in non-functioning cases are mandatory.
The main limitation of our study is the lack of information regarding the status of conjunctival epithelium before GMS surgery, which may be useful to accurately calculate the trans-scleral aqueous flow enhancement achieved with the shunt, as recently verified for trabeculectomy.24 Furthermore, to avoid reading biases due to the effect of the previous filtration procedures on the overall trans-scleral outflow, the effects of GMS should be evaluated in glaucomatous patients naïve for glaucoma surgery.
In conclusion, the in vivo analysis of conjunctiva in glaucomatous patients implanted with GMS provided valuable information which may help to clarify pathophysiological aspects of the aqueous outflow pathways exploited by the shunt.
References
Footnotes
Linked articles 187906.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.