Article Text

Abstract
Purpose Ocular burns can damage the corneal epithelial stem cells located at the limbus. This study evaluated the efficacy of xeno-free autologous cell-based treatment of limbal stem cell deficiency.
Methods This retrospective study included 200 patients, above 8 years of age, with clinically diagnosed unilateral total limbal stem cell deficiency due to ocular surface burns treated between 2001 and 2010. A small limbal biopsy was obtained from the unaffected eye. The limbal epithelial cells were expanded ex vivo on human amniotic membrane for 10–14 days using a xeno-free explant culture system. The resulting cultured epithelial monolayer and amniotic membrane substrate were transplanted on to the patient's affected eye. Postoperative corneal surface stability, visual improvement and complications were objectively analysed.
Results A completely epithelised, avascular and clinically stable corneal surface was seen in 142 of 200 (71%) eyes at a mean follow-up of 3±1.6 (range: 1–7.6) years. A two-line improvement in visual acuity, without further surgical intervention, was seen in 60.5% of eyes. All donor eyes remained healthy.
Conclusions Autologous cultivated limbal epithelial transplantation using a xeno-free explant culture technique was effective in long-term restoration of corneal epithelial stability and improvement of vision in eyes with ocular surface burns.
- Limbal stem cell deficiency
- xeno-free
- autologous
- cultivated limbal epithelial transplantation
- ocular surface burns
- iris
- sclera and episclera
- ocular surface
- cornea
- immunology
- imaging
- ocular surface
- stem cells
- epidemiology
- angiogenesis
Statistics from Altmetric.com
- Limbal stem cell deficiency
- xeno-free
- autologous
- cultivated limbal epithelial transplantation
- ocular surface burns
- iris
- sclera and episclera
- ocular surface
- cornea
- immunology
- imaging
- ocular surface
- stem cells
- epidemiology
- angiogenesis
Introduction
The corneal epithelium is continuously renewed by a steady supply of cells from the palisades of Vogt, located at the limbus.1 There is now enough scientific evidence to support that adult corneal epithelial stem cells reside at this location.2 3 Damage to the limbus by injury or disease, most commonly due to ocular surface burns, leads to limbal stem cell deficiency (LSCD) and consequently corneal epithelial breakdown.4 This clinically manifests as recurrent or persistent epithelial defects, progressive corneal vascularisation and eventually loss of corneal clarity.4
LSCD can be treated by transplanting healthy limbal cells from the unaffected fellow eye (autologous) or from donors (allogeneic) depending on whether the injury is unilateral or bilateral.5 Over the last two decades, the surgical technique has evolved from direct limbal transplantation6 7 to transplantation of ex vivo cultivated limbal epithelial cells,8 which requires less donor tissue and hence is thought to be safer for the donor eye. Despite this advantage, limbal cultivation may involve use of xenogenic tissue, associated with the risk of transmission of known or unknown infections to the transplant recipient.9–11 Xenogenic constituents of a limbal culture system may be in the form of murine feeder cells,8 12 13 fetal bovine serum (FBS)8 12–15 or animal-derived growth factors.16
Although an effective xeno-free technique of limbal cultivation is desirable, only six groups have reported the use of such a technique, but in few eyes and with variable follow-up.17–22 Currently, there are no large studies on the long-term outcomes of xeno-free autologous cultivated limbal epithelial transplantation.9 10 To fill this gap in existing literature, we report the long-term survival, visual benefit and complications of transplantation of autologous limbal epithelial cells, cultivated using a completely xeno-free explant culture technique, in 200 eyes with LSCD following ocular surface burns.
Methods
Study design and subjects
The study was approved by the Institutional Review Board of L V Prasad Eye Institute, Hyderabad, India, and was conducted in strict adherence to the tenets of the Declaration of Helsinki. Prior written informed consent was obtained from all patients or guardians, as appropriate. A retrospective chart review of all patients who underwent cultivated limbal epithelial transplantation for the treatment of LSCD between 1 April 2001 and 1 April 2010 was carried out.
The inclusion criteria for this study were as follows: (A) patients with a documented history of chemical or thermal burns; (B) patients with age at injury of more than 8 years; (C) patients who underwent autologous limbal transplantation for unilateral (defined as no clinical signs of ocular surface disease in the other eye) and total LSCD (defined as 360° superficial corneal vascularisation, diffuse fluorescein staining of the corneal surface with or without persistent epithelial defects, conjunctivalisation of the corneal surface and absence of limbal palisades of Vogt, figure 1); (D) patients with a postoperative follow-up time ≥12 months. The following exclusion criteria were applied: (A) patients who had bilateral LSCD or had allogeneic limbal transplantation; (B) patients who had limbal transplantation for partial LSCD or LSCD due to causes other than ocular surface burns; (C) cases treated prior to October 2002 when FBS was used for limbal culture if autologous serum (AS) was not obtained during limbal biopsy; (D) patients with stable corneal epithelium, but with <1-year follow-up; (E) patients with total LSCD, but with dry eye disease (Schirmer's test without anaesthesia of <10 mm in 5 min), were not considered for surgery; (F) patients with no visual potential as determined by clinical examination and electrophysiological testing (flash visual evoked potential and flash electroretinogram); (G) patients with untreated concurrent problems, such as glaucoma and infection, were not considered for surgery.
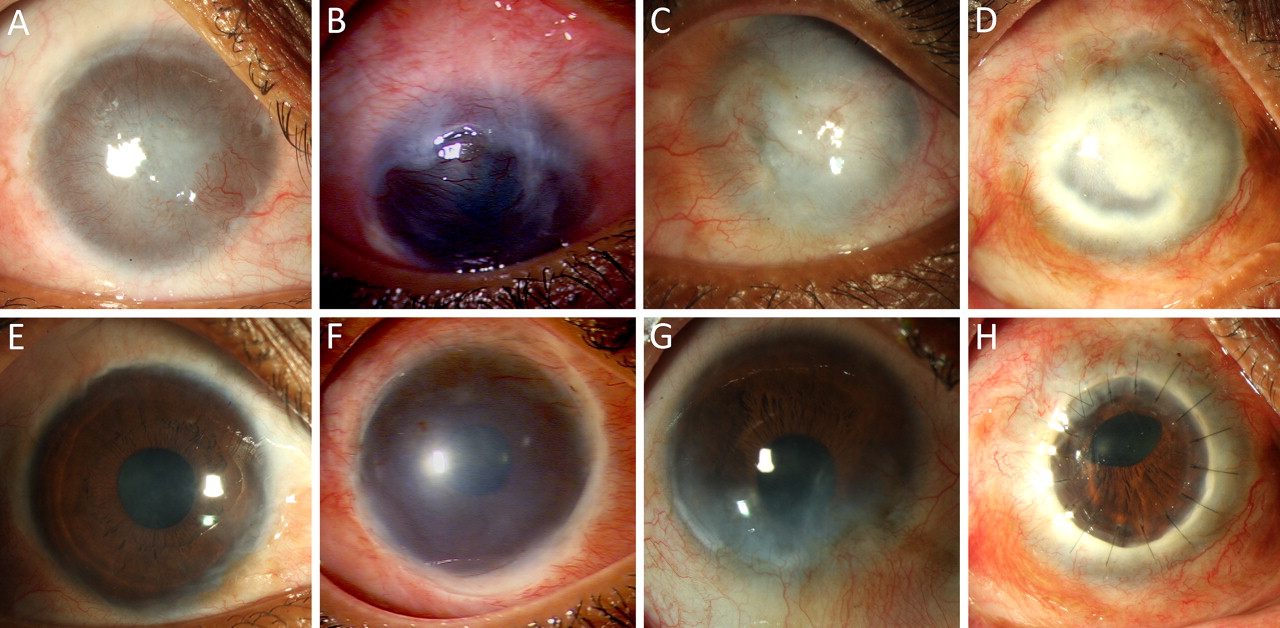
Clinical photographs of eyes before and after autologous cultivated limbal epithelial transplantation. Eyes of four different patients with total limbal stem cell deficiency and variable amounts of corneal stromal scarring (A to D); same eyes 1 year after limbal transplantation (E to H). Right eye of a 26-year-old female patient with a history of alkali injury showing a stable corneal surface, minimal stromal scarring and a best-corrected visual acuity (BCVA) of 20/30 (E). Right eye of a 19-year-old male patient with a history of acid injury showing a stable corneal surface with residual stromal scarring with a BCVA of 20/100 (F). Right eye of a 45-year-old male patient with a history of alkali injury showing recurrence of conjunctivalisation inferiorly (failure) between 4 and 7 o'clock at the limbus, with a BCVA of 20/40 (G). Right eye of a 37-year-old female patient with a history of acid injury showing a stable corneal surface and a clear corneal graft with a BCVA of 20/20 (H).
Data collection
The data retrieved from the medical records included age and sex of the patient, type and date of injury, details of prior ocular procedures, Snellen's best spectacle-corrected visual acuity (BCVA) and intraocular pressure at presentation and at each follow-up visit, presence or absence of lid abnormalities, dry eye disease, symblepharon, degree of limbal involvement, intraoperative surgical details, postoperative complications, duration of follow-up and status of ocular surface at each visit (slit-lamp findings including fluorescein staining).
Outcome measures
The primary outcome measure was success of transplantation, defined clinically as a completely epithelised, avascular and clinically stable corneal surface. Failure was defined as the occurrence of superficial corneal vascularisation or persistent epithelial defects. Survival time was calculated in months from the date of limbal transplantation to the date of failure or the date of last follow-up depending on the clinical outcome. The secondary outcome measure was the proportion of eyes that had a two-line improvement in BCVA at last follow-up or before undergoing penetrating keratoplasty (PK) as compared to baseline.
Technique of limbal biopsy
A biopsy was taken from a healthy part of the limbus. A 2×2 mm piece of conjunctival epithelium with 1 mm into clear corneal stromal tissue at the limbus was dissected. Conjunctiva was excised just behind the pigmented line (palisades of Vogt), and the limbal tissue that contained epithelial cells and a part of the corneal stroma was obtained.23
Technique of limbal culture
The tissue was transported to the laboratory in human corneal epithelium (HCE) medium.23 HCE is composed of modified Eagle's medium/F12 medium (1:1) solution containing 10% (vol/vol) AS, 2 mM l-glutamine, 100 U/ml penicillin, 100 μg/ml streptomycin, 2.5 μg/ml amphotericin B, 10 ng/ml human recombinant epidermal growth factor and 5 μg/ml human recombinant insulin.23 Under strict aseptic conditions, the donor limbal tissue was shredded into small pieces. Human amniotic membrane (hAM), prepared and preserved by our eye bank, was used as a carrier. A 3×4 cm hAM sheet was de-epithelised using 0.25% recombinant trypsin23 and EDTA solution for 15 min. The shredded bits of limbal tissue were explanted over the centre of de-epithelised hAM with the basement membrane side up. A similar parallel culture was also prepared as a backup. A submerged explant culture system without a feeder cell layer was used. We used the HCE medium to nurture the culture. The culture was incubated at 37°C with 5% CO2 and 95% air. The growth was monitored daily under an inverted phase contrast microscope, and the medium was changed every other day. The culture was completed when a monolayer of the cells growing from the explants became confluent, typically in 10 to 14 days.
Technique of limbal transplantation
Any symblepharon which prevented adequate separation of the lids was released to permit the insertion of a wire speculum (no additional surgery to treat the symblepharon was performed).15 A peritomy was performed, and the corneal fibrovascular pannus was excised. If excessive corneal thinning or perforation was noted at this stage, a lamellar or penetrating keratoplasty was performed.24 The hAM and monolayer of cultivated limbal epithelial cells were spread over the cornea, epithelial side up. The graft was then secured to the peripheral cornea by interrupted, circumferential 10-0 nylon sutures and to the surrounding conjunctival edge by interrupted 8-0 polyglactin sutures.15 Alternately, using a sutureless technique, the graft was secured to underlying ocular surface with fibrin glue (TISSEEL Kit from Baxter AG, Austria), and the margins of the graft were tucked under the surrounding conjunctival edge.15 Bandage contact lenses were not applied at the end of surgery.
Postoperative management
All patients were treated with 1% prednisolone acetate eye drops eight times a day tapered to once a day in 35–42 days and 0.3% ciprofloxacin hydrochloride eye drops four times a day for 1 week. The latter were continued, as needed, if an epithelial defect was present. No systemic antibiotics or steroids were administered to any patients. Patients were examined on postoperative days 1, 7 and 42 and at an interval of 90–180 days thereafter, as customised by the clinical appearance of the transplant. Each examination included a complete history, visual acuity assessment with Snellen's charts, intraocular pressure measurement and detailed ocular examination with slit-lamp biomicroscopy.
Statistical analysis
MedCalc (V.11.4.3.0) statistical software was used for data analysis. The outcome of transplantation was analysed using Kaplan–Meier survival curves, and survival probability/rate at 1 year was reported as percentage (±SE). Multiple logistic regression analysis was performed to test the association between graft failure and clinical variables. A two-tailed p value of <0.05 was considered statistically significant.
Results
Demographics
This study included 200 eyes of 200 patients with LSCD due to ocular burns. The mean age of the patients was 24.1±9.9 years, and the male to female ratio was 159:41. Table 1 summarises the baseline demographic features of all 200 eyes. Although 56 (23.5%) fellow eyes had history of simultaneous injury, none had clinical features of ocular surface disease at presentation. The mean follow-up was 3±1.6 (range 1–7.6) years. All 200 patients had follow-up of 1 year; 117, 73, 61, 39, 18 and 4 patients had follow-up of 2, 3, 4, 5, 6 and 7 years, respectively.
Demographic features of 200 eyes treated with xeno-free autologous cultivated limbal epithelial transplantation
Primary outcome
At final follow-up visit, 142 of the 200 (71%) eyes maintained a completely epithelised, avascular and clinically stable corneal surface. The Kaplan–Meier survival rate was 76.4%±3% at 1 year and 68.1%±4% at 2 years and thereafter (figure 2). Multiple logistic regression showed that eyes with prior amniotic membrane grafts (OR 3, 95% CI: 1.3 to 6.7, p=0.007) or prior keratoplasty (OR 4.7, 95% CI:1.9 to 11.3, p=0.0006) or keratoplasty along with limbal transplantation (OR 9.8, 95% CI: 1.9 to 50.1, p=0.006) had greater risk of failure, but there was no association seen with age, gender, duration between injury and surgery, aetiology of injury, presence of lid abnormalities, prior lid surgeries, presenting vision and presence or absence of symblepharon (p>0.5).

Kaplan–Meier survival analysis of 200 eyes treated with autologous cultivated limbal epithelial transplantation from April 2001 to April 2010. The survival was 76.5%±3% at 1 year postoperatively and 68.1%±4% at 2 years and thereafter.
Secondary outcome
Of the 200 eyes, a two-line improvement in BCVA was seen in 121 (60.5%) eyes. At last follow-up visit or before undergoing keratoplasty, 80 (40%) eyes had BCVA of 20/60 or better, 54 (27%) had BCVA of 20/70 to 20/200 and 66 (33%) eyes had BCVA worse than 20/200. Of the 66 eyes with BCVA of less than 20/200, 58 (29%) eyes had poor vision due to recurrence of LSCD, and 8 (4%) eyes had corneal scarring for which PK was done subsequently.
Treatment failures and adverse events
Failures occurred between 1 month and 20.6 months of limbal transplantation, and 47 (81%) of the 58 failures occurred within 1 year. Haemorrhage under the amniotic membrane was seen postoperatively in 56 (23%) eyes, all of which resolved spontaneously. Among the 58 eyes with treatment failure, persistent epithelial defects developed in 13 (22.4%) eyes; five (2.5%) eyes developed sterile corneal melts which were managed with tissue adhesive application. Three (1.5%) eyes developed bacterial keratitis, of which two eyes resolved with intensive medical treatment and one eye needed an emergency PK. Successful ex vivo expansion of the limbal epithelial cells was seen in all cases, and none of the patients had to undergo a repeat biopsy. None of the donor eyes developed any clinical signs or symptoms of ocular surface disease, and the donor site healed without scarring in 10–14 days (figure 3).

{kind=link}
{kind=link}
{kind=link}
Serial clinical photographs of donor eyes of two different patients after limbal biopsy showing different morphological patterns of epithelisation. Right eye of a 23-year-old male patient shows a large epithelial defect involving the bulbar conjunctiva and limbus 1 day after limbal biopsy. (A) Three days later, the limbus had re-epithelised, and the conjunctival defect had reduced. (B) A small v-shaped defect on the bulbar conjunctiva was noted 7 days after biopsy, (C) and complete epithelisation was seen 2 weeks after biopsy (D). Left eye of a 19-year-old female patient shows a similar large epithelial defect involving the bulbar conjunctiva and limbus 1 day after limbal biopsy (A); within 3 days, the limbus had re-epithelised with reduction in the size of the conjunctival defect (B). A small oval defect remained on the bulbar conjunctiva 7 days after biopsy (C), and complete epithelisation was noted 14 days after biopsy, on the day of limbal transplantation in the contralateral eye (D).
Discussion
Previous studies have shown that cultivated limbal epithelial transplantation is as effective as direct limbal transplantation for the treatment of LSCD, while requiring less donor limbal tissue and hence being safer for the donor eye.6–10 However, limbal cultivation is not without its disadvantages, like additional laboratory costs and theoretical risks associated with using xenobiotic materials for culture.9–11 These two factors have restricted the popularity of cultivated limbal epithelial transplantation to a few advanced centres around the globe.9 10 Having used FBS prior to October 2002,15 we subsequently developed a feeder-free explant culture system using human AS and human recombinant growth factors.23 Over the course of the last decade, we have characterised the cultured cells,25 standardised our cultivation technique23 and shown how the transplanted monolayer of cells forms a normal stratified corneal phenotype in vivo.24 26 27 Our previous report summarised the clinical results in the initial 88 eyes with partial and total LSCD due to a variety of causes, treated with limbal cells cultivated using either FBS or AS, with a success rate of 73% and follow-up ranging from 3 to 41 months.15 In contrast to our previous report, this large series of 200 eyes focused on a more homogenous group with total LSCD due to ocular burns and a minimum follow-up of 1 year.
This study found that the transplantation of limbal epithelial cells cultivated using our xeno-free explant culture technique was successful in ocular surface restoration in 71% of the 200 recipient eyes. Previous studies by Nakamura et al,17 Shimakazi et al,18 Di Girolamo et al,19 Kolli et al20 and Zakaria et al22 also described xeno-free techniques for autologous limbal cultivation, but they were limited by the relatively smaller samples of two to eight eyes. In addition to being clinically effective and free of animal-derived products, this technique of cultivation was also extremely reliable, as ex vivo expansion was successful in every case. We have previously shown that inadequate growth or contamination is seen in <1.5% of the cultures in our system.28
The overall success rate of cultivated limbal epithelial transplantation, as reported in various studies, ranges between 50% and 100%.9 10 In comprehensive reviews of this procedure, Baylis et al and Shortt et al found no significant differences in the clinical outcomes based on source of donor tissue (autologous or allogeneic), culture technique (explant or suspension) or indication for surgery.9 10 Caution must be exercised before comparing our results with those of existing literature because the indications for surgery, sample size and follow-up duration are widely variable among different studies.8 9 It is noteworthy in this context that with similar indications for surgery, clinical criteria for success and follow-up, our success rate (71%, 200 eyes) compares well with that of Rama et al (68%, 107 eyes)12 and Di Iorio et al (80%, 166 eyes),13 who unlike us used a feeder-cell- and FBS-based suspension culture technique.
The actual mechanism by which limbal transplantation works is still debated. It is unclear whether this treatment replenishes the stem cell reserve12 or revives the surviving stem cells by improving the microenvironment.10 It is also widely accepted that the cause of failure of limbal transplantation is multifactorial and poorly understood.9 10 Surprisingly, we found that eyes having undergone prior amniotic membrane grafts or PK were more prone to failure of the limbal transplant. This finding needs to be interpreted carefully and should not be misconstrued as a contraindication for performing these procedures during acute stage of ocular burns. This association is simply indicative of the fact that eyes with more severe injury need multiple surgical interventions and are more difficult to treat.12 Additionally, we found that the timing of limbal transplantation did not affect the eventual outcome. In our opinion, this procedure can be performed as early as 3 months after the initial injury, but only if the ocular surface inflammation has been adequately controlled by that time.
The strengths of this study include the large, homogenous sample and long follow-up. The limitations include the retrospective design and subjective clinical criteria for diagnosis and success of treatment. The rarity of the disease makes a retrospective design a necessity, although a multicentric prospective study involving all the clinical centres around the world practicing this treatment is something worth considering. The alternative to clinical assessment is an objective scoring system based on impression cytology or a symptom-based questionnaire, both of which have inherent limitations.
In conclusion, our goal was to study the long-term clinical outcomes of transplanting autologous limbal epithelial cells, cultivated using a xeno-free explant culture system for eyes with LSCD due to ocular burns. We found that our technique was successful in long-term restoration of the ocular surface and vision with no adverse effect on the donor eyes. This report provides ample clinical evidence to support the use of simpler xeno-free limbal cultures, which will eliminate any real or perceived risks associated with the use of animal products and allow wider applicability of this effective technique.
References
Footnotes
Funding This work was funded by a competitive grant from the Department of Biotechnology, India (BT/01/COE/06/02/10), a partnership grant from the Champalimaud Foundation, Portugal, and support from Sudhakar and Sreekanth Ravi, California, USA (for equipment and laboratory infrastructure). None of these had any role in the design, collection, analysis and interpretation of the data.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics Committee, L V Prasad Eye Institute, Hyderabad, India.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance