Article Text

Abstract
Background and aims In Scotland, uveal melanomas are primarily treated with eye-preserving modalities with a low primary enucleation rate. Proton beam therapy (PBT) is reserved for those not suitable for brachytherapy. The authors' aim was to review the outcome of Scottish patients undergoing treatment for uveal melanoma with PBT.
Method All ciliary body or choroidal melanomas treated initially with PBT between 1 January 1993 and 30 March 2008 were identified. Data were gathered from retrospective review of case notes, database information, PBT planning data, ultrasound and pathology reports.
Results 147 patients were identified. The mean age was 62.3 years, 94.6% were choroidal melanomas. 97.8% of all treated melanomas were of medium or large size. Enucleation during follow-up occurred in 22.4%. Mean time to this was 23.8 months and main reasons were suspected recurrence (48%) and neovascular glaucoma (42%). Metastatic death occurred in 9.5%, the mean time to this was 28.9 months. The actuarial 5-year eye retention rate was 71.3% and disease-specific survival rate was 87.7%.
Conclusion PBT is reserved for the treatment of mainly medium-sized and large-sized uveal melanomas in Scotland. The eye retention and disease-specific survival rates confirm its suitability as an eye-preserving primary treatment in these patients. It is evident that PBT is a conservative treatment option for uveal melanoma, including those of larger size.
- Uveal melanoma
- proton beam therapy
- eye conservation
- survival rate
- neoplasia
Statistics from Altmetric.com
Introduction
Uveal melanoma is the most common primary ocular malignancy.1 2 It is rare with an incidence of 6–7 per million per year.1 2 Treatment occurs in specialist centres.1 The Scottish Ophthalmic Oncology Service (SOOS) is based at The Tennent Institute of Ophthalmology in Glasgow.
Uveal melanoma can lead to visual disruption, loss of the eye, metastatic disease and death.3 The choroid is the most common site; it may also involve the iris or ciliary body.4–6 It can spread locally or disseminate haematogenously to cause metastatic disease.7 8 The prognosis for metastatic disease is poor.8 Traditionally, enucleation was the treatment for uveal melanoma but eye-preserving modalities have now been available for decades.2 Options include radiotherapy, local resection, transpupillary thermotherapy, laser photocoagulation and enucleation.1 4 The primary aims of management are local tumour control and prevention of metastatic disease and death.6 A secondary aim is eye retention for function and cosmesis.6
The selected treatment depends on those available at that centre and the patient and tumour characteristics.1 Common radiotherapy modalities are brachytherapy (with ruthenium or iodine plaques) or proton beam therapy (PBT).1 8 Radiotherapy is more desirable than enucleation as it permits eye retention, potentially with vision. The Collaborative Ocular Melanoma Study (COMS)9 demonstrated that metastatic disease rate and overall survival was not significantly different between those treated with enucleation and radiotherapy (brachytherapy). Brachytherapy and PBT have proven efficacy in uveal melanoma treatment and are now widely used.10 PBT delivers a homogenous dose of radiation within the tumour volume, whereas in brachytherapy the tumour base receives several times the dose of the tumour apex.6 PBT avoids any risk of radiation exposure to the surgeons' hands.6 In some centres, it is selected for all uveal melanomas undergoing radiotherapy treatment.6 It is, however, more expensive and time-consuming in comparison to brachytherapy and can cause significant side effects in ocular and extra-ocular structures.3 Therefore, in many centres it is reserved for a select group of patients.1 3 It permits radiotherapy in larger tumours not suitable for brachytherapy and may be preferred for tumours located close to the optic disc or macula.6
The SOOS receives oncology referrals from the whole of Scotland. Diagnosis of uveal melanoma is made after clinical examination, colour photography and ultrasound. The treatment selected is based on the size and location of the lesion, taking into consideration the patient and their wishes. PBT is selected as a conservative treatment for larger tumours (height >5.5 mm) or those otherwise not suitable for brachytherapy, usually due to location. The patient has four tantalum markers inserted at The Tennent Institute followed by PBT at the Clatterbridge Centre for Oncology. Treatment is with 53.1 proton Grey in four daily fractions. Follow-up is then performed in Glasgow.
Aim
To determine the patient demographics, tumour characteristics, eye retention rate and disease-specific survival rate of Scottish patients undergoing treatment for choroidal and ciliary body melanoma with PBT.
Method
A search of the SOOS database identified all those with a choroidal or ciliary body melanoma treated initially with PBT between 1 January 1993 and 30 March 2008. Information regarding the patients, their treatment and outcome was gathered from database information, retrospective review of patient case notes, PBT planning data, ultrasound and pathology reports.
The results were entered and analysed using Microsoft Excel. Statistical analysis was performed using Minitab. Tumour height and transverse diameter are from the measurements prior to PBT. The grouping of tumour size described in COMS9 (table 1) was used to summarise the range of treated lesions. The follow-up time, enucleation and metastatic rates were calculated from the last clinic visit or other available information (eg, a letter informing of enucleation or death). Patients who died or were lost during follow-up were censored from analysis at the date of death. Data were incomplete in 15 patients. These patients were excluded from analysis of the missing information but included where data were available. All-cause and disease-specific mortality rates were cross-referenced with the death statistics held by the Information Services Division Scotland (ISDS). Kaplan–Meier estimates were used to predict 3-year and 5-year eye retention and metastatic death rates with the value and 95% CI expressed.
Size defined in COMS9 of treated ciliary body and choroidal melanoma at presentation
Results
The search of the SOOS database identified 585 patients diagnosed with uveal melanoma between 1 January 1993 and 30 March 2008. A total of 147 of these patients had received PBT as their first treatment for a ciliary body or choroidal melanoma, representing 25.1%.
All patients treated with PBT
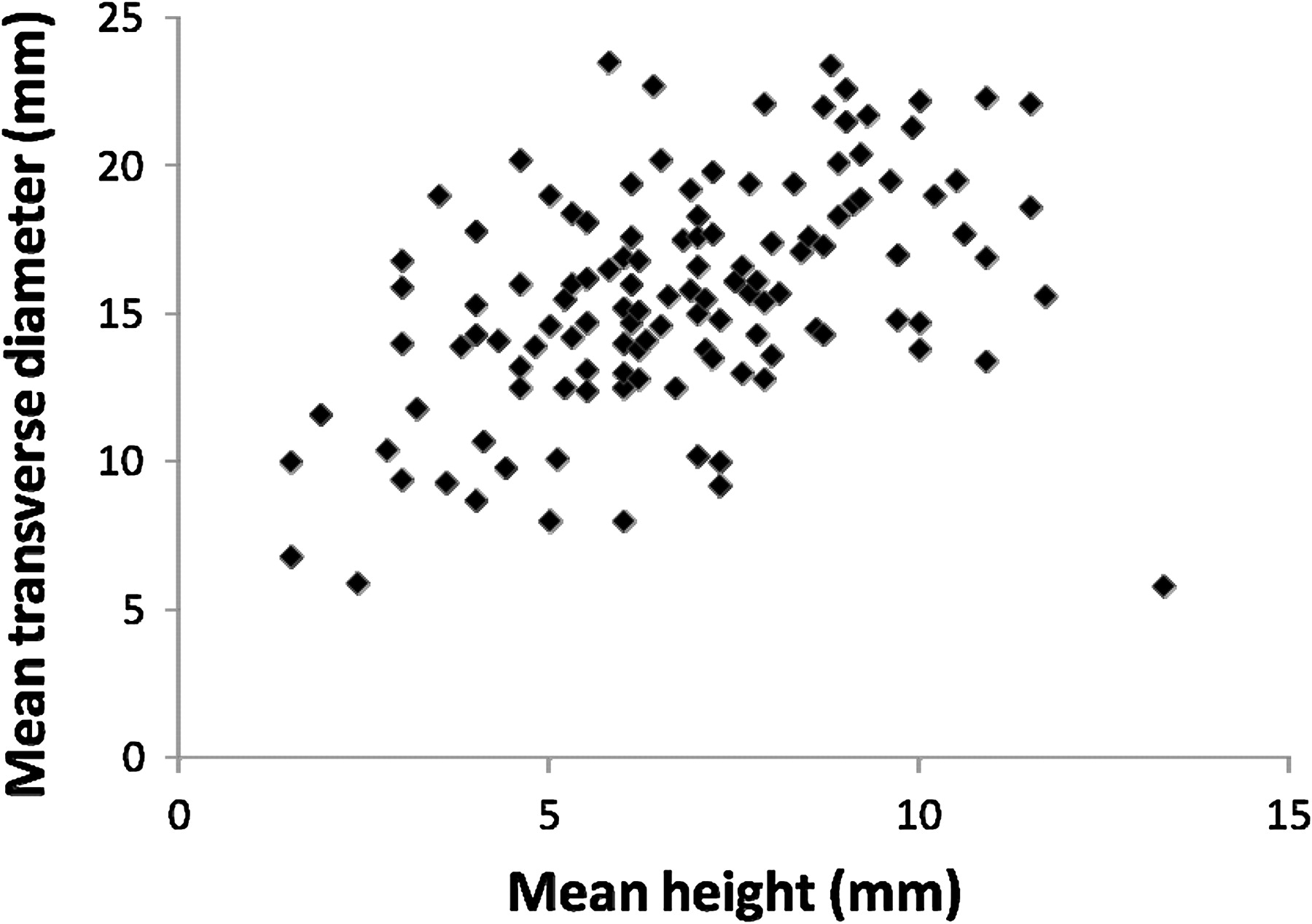
The location, age and tumour size are summarised in table 2 and figure 1. The mean follow-up time was 4.4 years (range: 3 months–15 years, median 3.1 years). Eighty-three (56.5%) of the 147 patients had been followed for 3 years or more post-PBT at the time of data collection and 58 (39.5%) patients for 5 years or more post-PBT. Thirty-six (24.5%) patients died from all-cause mortality during follow-up. Based on the COMS classification, 51.9% of all treated ciliary body and choroidal melanomas were of medium size and 45.9% were large.
Comparison of the location, age and tumour size of all uveal melanoma patients treated with PBT compared with those enucleated and dying from metastases

Tumour size. Scatter plot of the mean height and the mean diameter of the ciliary body and choroidal melanomas treated with PBT.
Patients requiring subsequent enucleation
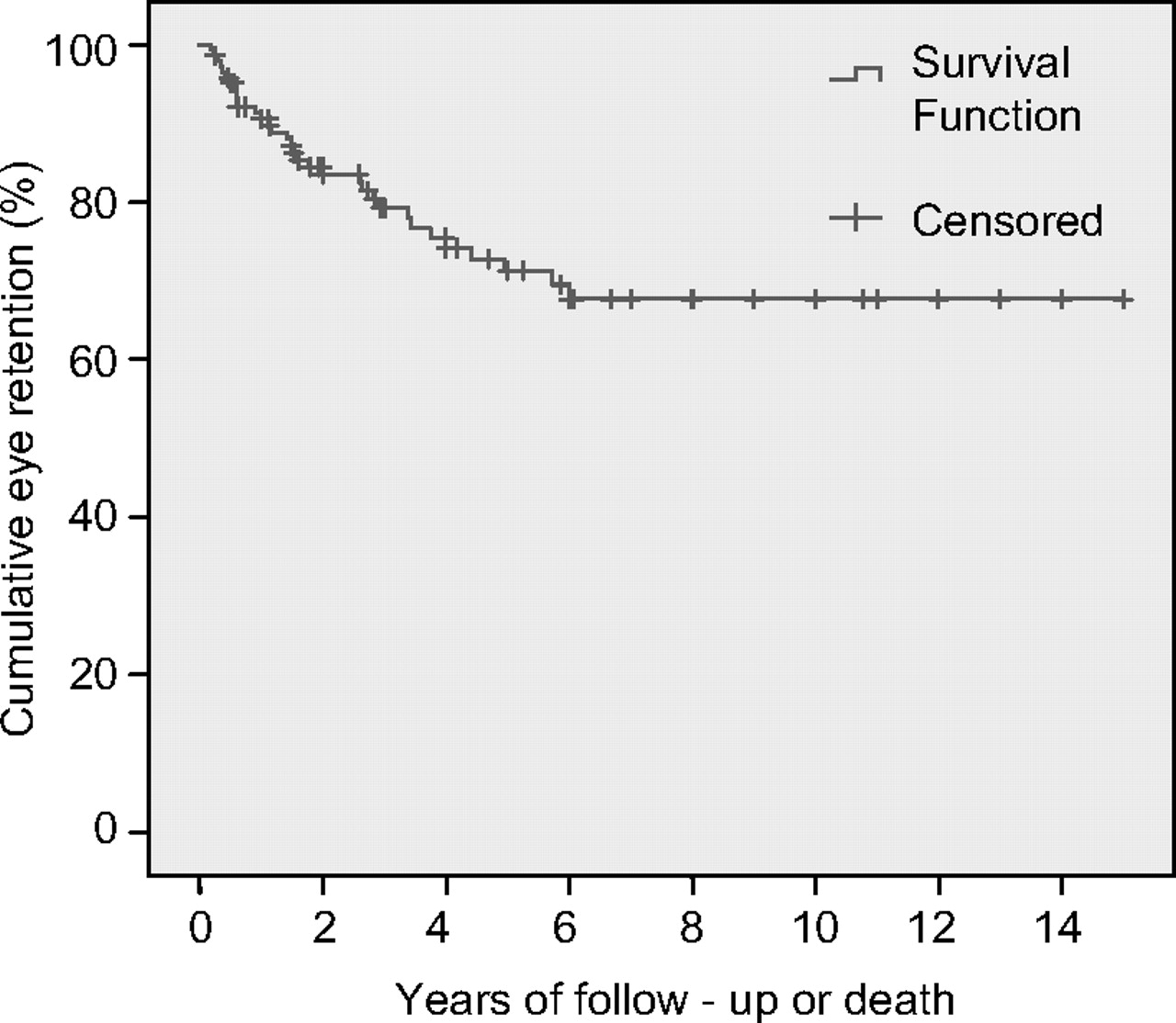
The location, age and tumour size are summarised in table 2. Enucleation during follow-up was necessary in 22.4%. The time between PBT and enucleation ranged from 2.1 to 68.6 months. The mean value was 23.8 months (median 17.4 months); 78.8% of enucleations were performed within the first 3 years. The reason for enucleation was suspected recurrence in 48%, neovascular glaucoma in 42% or another complication of PBT treatment in 10%. Histological analysis of enucleated specimens was available in 30 of the 33 cases. Fourteen of the 16 eyes enucleated for suspected recurrence had histological data available. In these, eyes histology revealed mitotic activity in 10 cases and intrascleral, extrascleral or vortex vein invasion with tumour in 4 cases. According to COMS, 67.7% of our enucleated tumours were large-sized pre-PBT and 25.8% were medium-sized pre-PBT. The mean height and mean diameter of the group of tumours requiring subsequent enucleation were larger than the mean height and mean diameter of all the treated melanomas. The Kaplan–Meier predicted 3-year eye retention rate was 79.2% (95% CI 71.8% to 86.6%) and 5-year eye retention rate was 71.3% (95% CI 62.3% to 80.3%) (figure 2).

Actuarial eye retention following PBT for uveal melanoma in Scotland.
Patients subsequently dying from metastases
The location, age and tumour size are summarised in table 2. Metastatic death occurred in 9.5% of all treated patients. The time between PBT and death from metastases ranged from 7.9 to 70.4 months. The mean value was 28.9 months (median 21.3 months). Twelve occurred within 3 years post-PBT. According to COMS, all of tumours associated with subsequent metastatic death were of large size pre-PBT. The mean height and mean diameter of the group of tumours subsequently leading to death from metastases were larger than the mean height and mean diameter of all the treated melanomas. The site of metastases was the liver in 10 patients, the lung in 1, the lung and bone in 1 and unknown in 2. All patients underwent palliative treatment only for the metastatic disease. Seven of the patients who died from metastatic disease had undergone prior enucleation, in six cases this had been for recurrence. The Kaplan–Meier predicted 3-year disease-specific survival rate was 89.1% (95% CI 83.2% to 95.0%) and 5-year disease-specific survival rate was 87.7% (95% CI 81.2% to 94.2%) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Actuarial disease-specific survival following PBT for uveal melanoma in Scotland.
Discussion
PBT is reserved in Scotland for the treatment of mainly medium-sized and large-sized uveal melanomas. The actuarial 5-year eye retention rate for this patient group has been predicted at 71.3%, and the 5-year disease-specific survival rate at 87.7%, justifying its use as an eye-preserving primary treatment.
The majority of treated tumours were choroidal melanomas, similar to previous reports of uveal melanoma (94.6%).4–6 The mean patient age, 62.3 years, is broadly comparable with other studies.2–4 6 10 The mean follow-up after PBT was 4.4 years, 56.5% had at least 3 years follow-up and 39.5% had at least 5 years follow-up. Follow-up time varies between studies with some shorter and others longer than this.2–4 6 10 The follow-up period in this study reflects the 24.5% all-cause mortality rate. A longer period increases long-term result accuracy, if the number of patients lost from review is small. Although our follow-up was shorter than some other studies, there were few patients in which follow-up data were incomplete. Based on the COMS classification, 51.9% of all treated ciliary body and choroidal melanomas were of medium size and 45.9% were large. The mean height of all treated tumours was 6.7 mm, and the mean diameter was 15.4 mm. In comparison with other studies, the tumours selected for PBT treatment were towards the upper end of the range in terms of height and diameter.2–4 6 7 10–12
Comparison of outcome data from different centres is difficult as no reporting standards exist and there is no universally adopted treatment protocol for uveal melanoma.6 Some centres will use PBT to treat the vast majority of uveal melanomas. Others will reserve it for a select group of tumours, utilising other modalities, such as brachytherapy for smaller tumours and primary enucleation for larger ones. Therefore the size, location and other tumour characteristic vary, as may the administered treatment protocol. Most centres treat tumours in patients from a specific geographical location and populations may differ in risk factors influencing outcome.
In this study, subsequent enucleation was required in 22.4%. The mean time to this post-PBT was 23.8 months, 78.8% were enucleated within 3 years. This is similar to previous data suggesting the majority are performed in the first 3 years, but may occur later.2 6 10 11 The main reasons for enucleation were suspected recurrence and neovascular glaucoma similar to other reports.2 3 6 10 The Kaplan–Meier 5-year eye retention rate was 71.3%. Others have reported a 5-year eye retention rate of 71.1–100%.3 6 10–12 Some describe outcome by presentation size and show a higher enucleation rate in larger tumours. The results suggest that our eye retention rate lies towards the lower end of reported ranges. Factors reported to increase enucleation rate include an anterior location or ciliary body tumour, proximity to the optic disc or fovea, the size (tumour diameter and height), the total radiation dose, irradiation of the anterior segment and intra-ocular or extra-ocular extension.3 4 6 10 11 13 These were not all assessed in our study. The dose given was towards the lower end of that reported and the treatment was administered at the same centre as the study by Damato.3 4 6 10 11 13 A differing dose or treatment regime does not explain our enucleation rate. Not all studies included ciliary body tumours, which may have increased our enucleation rate.3 10 11
According to COMS, 93.5% of our enucleated tumours were large-sized or medium-sized pre-PBT. The mean height of all enucleated tumours was 7.7 mm, and the mean diameter was 17.2 mm. No study is directly comparable with our data. Fuss et al10 reported results for medium and large melanomas, with a 5-year eye retention rate of 75.3% also towards the lower end of reported rates. That study differed from ours, however, as it included only choroidal tumours and the overall mean diameter of treated melanomas was lower. In our study, the mean height and transverse diameter of the enucleated group were both greater than that of all the treated melanomas. It is likely that the tumour size at presentation was a contributing factor to their subsequent enucleation and influenced the 5-year eye retention rate.
Our 5-year eye retention rate may be a reflection of using PBT to treat mainly larger, higher risk tumours and a low primary enucleation rate, reserving this for a few unsalvageable eyes at presentation. Due to this many patients with large tumours are treated initially in our centre with PBT when others might undertake primary enucleation. Larger tumour size influences subsequent enucleation for two reasons; it increases the risk of local recurrence and the risk of PBT complications.3 The decision to enucleate post-PBT in our centre is taken after discussion with the patient. Of those carried out, 48% were for suspected recurrence, higher than in some previous reports. Local recurrence is diagnosed following evidence of growth (height and/or diameter) on serial ultrasounds and/or clinical suspicion from changes in the tumour appearance on photographs over sequential visits. An initial change in size post-PBT may represent a treatment reaction and is initially closely observed in our centre but continued growth over subsequent visits necessitates further treatment. In our centre this is almost always enucleation, with few other treatments undertake in patients at this stage. This may explain the higher rate of enucleations carried out for recurrence in our centre compared with others who may treat recurrence post-PBT with further eye-preserving modalities. There is no uniform, clearly defined indication for enucleation post-PBT, and thresholds for carrying it out may vary between studies.11 It is therefore not a directly comparable outcome statistic between studies, but does provide local information regarding the effectiveness of treatment in achieving tumour control without severe complications.11 The higher enucleation rate post-PBT in our centre compared with some other reflects the large size of tumour treated, the low primary enucleation rate (PBT is almost always tried first) and the low threshold for enucleation after PBT for tumour growth or complications. Eye retention is the reason for choosing PBT over primary enucleation and the risk of subsequent enucleation and characteristics of these patients facilitate future management of patients with larger tumours.
Metastatic death occurred in 9.5% of our patients, 7.9–70.4 months post-PBT. Twelve occurred within 3 years post-PBT. Previous data show annual mortality rises rapidly following treatment, peaking at 2–3 years before declining with extending follow-up.14 The Kaplan–Meier 5-year disease-specific survival rate was 87.7%. Based on COMS and meta-analysis of studies, the predicted 5-year disease-specific mortality rate was 31–35% for large tumours, 10% for medium tumours and 1% for small tumours.13 Other studies have reported varying 5-year disease-specific survival rates of 75.6–90.0%.2–4 6 7 10 Our patients' survival rate is comparable with other studies, lying towards the upper end of those reported.
Metastatic death rates have remained relatively static despite the success of conservative treatments in achieving local control.5 A change is unlikely without a better understanding of the pathophysiology, prevention and treatment of metastases.13 Presenting tumour size influences the risk of metastatic death.5 The majority of tumours likely to metastasis have probably done so by presentation in medium and large size tumours.5 The time to death varies with growth characteristics and may occur many years later.5 13 Actively growing tumour can also act as a reservoir.5 Local recurrence is associated with an increased risk of metastatic death.5 Other reported factors include an anterior or ciliary body location, proximity to the fovea, advanced patient age, the genotype and associated chromosomal abnormalities and the phenotype or histological features of the tumour.2 10 13 These were not all assessed in our patient group. Given the size of the tumours treated in this study, it is perhaps surprising that more of our patients did not die from metastases. It is however noticeable that the mean height and mean diameter of the tumours subsequently leading to metastatic death in our study were larger than all the treated melanomas included. It is likely that the size at presentation (all classed as large) in these patients was a contributing factor to their subsequent death. Their mean age at presentation was also higher than that for all patients. It has been suggested that older patients have a reduced defence against growth of metastases, which may have contributed to their death within a shorter period.14 Although not assessed, it is possible that the genotype or phenotype of our patients may vary from others, influencing the risk of or time to metastases. It is possible that we did not identify all patients with metastases, although we feel that this is unlikely to equate to a significant number. Those who lost to follow-up or died from other causes may have had unrecognised metastatic disease and not been included in the Kaplan–Meier analysis. The risk of this was minimised by using multiple sources of hospital information and correspondence with the patients' general practitioner to keep the database up to date. All patients included in the study were also cross-referenced with ISDS to check for deaths we were not aware of, the cause of deaths and any patients coded as having metastatic disease. We therefore feel that the vast majority of patients with known metastatic disease were included in our analysis, although we recognise that with almost one-quarter of our patients who died during follow-up some may have had unrecognised metastases or died before metastatic disease would have become clinically recognised.
Conclusion
This study confirms PBT as an effective treatment of uveal melanoma, with results in Scotland comparable with other centres. It suggests that the 5-year eye retention rate for uveal melanoma treated with PBT in Scotland was approximately 71.3%. This group of mainly medium and large tumours was at a higher risk of subsequent enucleation than all patients presenting with uveal melanoma, but our study supports the view that eye retention is still achievable in a high number. The 5-year disease-specific survival rate was predicted at 87.7%. It is reassuring that although the treated patients fell into a higher risk group for metastases than many other studies, the choice of a conservative treatment (ie, PBT rather than enucleation) did not adversely affect survival. It is evident that PBT is an effective eye-preserving treatment option for uveal melanoma, including those of larger size, which does not appear to adversely affect the mortality rate.
Acknowledgments
The authors thank Dr David Young, Department of Statistics and Modelling Science, University of Strathclyde, Glasgow.
References
Footnotes
The corresponding author confirms that she had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.