Article Text

Abstract
Background Severe bacterial keratitis (BK) typically requires intensive antimicrobial therapy. Empiric therapy is usually with a topical fluoroquinolone or fortified aminoglycoside–cephalosporin combination. Trials to date have not reached any consensus as to which antibiotic regimen most effectively treats BK.
Methods A systematic review and meta-analysis using Cochrane methodology was undertaken to evaluate the effectiveness of topical antibiotics in the management of BK. Outcomes included treatment success, time to cure, serious complications of infection and adverse effects.
Results A comprehensive search for trials resulted in 27 956 abstracts for review. This eventually resulted in 16 high quality trials involving 1823 participants included in the review. Treatment success, time to cure and serious complications of infection were comparable among all antibiotic treatments included in the review. Furthermore, there was no evidence of difference in the risk of corneal perforation with any included antibiotics or antibiotic classes. Fluoroquinolones significantly reduced risk of ocular discomfort and chemical conjunctivitis but increased the risk of white precipitate formation compared with aminoglycoside–cephalosporin. Fortified tobramycin–cefazolin was approximately three times more likely to cause ocular discomfort than other topical antibiotics.
Conclusions Results of this review suggest no evidence of difference in comparative effectiveness between fluoroquinolones and aminoglycoside–cephalosporin treatment options in the management of BK. There were differences in safety profile, however. Fluoroquinolones decreased the risk of ocular discomfort and chemical conjunctivitis while ciprofloxacin increased the risk of white corneal precipitate compared with aminoglycoside–cephalosporin.
- bacterial
- keratitis
- review
- antibiotics
Statistics from Altmetric.com
Introduction
Bacterial keratitis (BK) remains a leading cause of ocular morbidity worldwide.1 The effects of BK range from mild corneal irritation to visual loss, corneal perforation or blindness. Severe infection may require hospitalisation and is typically treated with an intensive empiric regimen consisting of 15 min to hourly instillation of topical fortified aminoglycoside–cephalosporin (combination therapy) or topical fluoroquinolone (monotherapy), following corneal scrape and cultures.2 ,3 Severe bacterial infection may result in significant stromal scarring, which may eventually require corneal transplantation to restore vision.
While empiric treatment of BK is necessary when awaiting the outcome of culture and sensitivity testing, or where culture facilities are unavailable, the antibiotic regimen chosen should be of a sufficiently broad spectrum to cover likely pathogens while considering bacterial prevalence, antibiotic sensitivities and geographically-specific epidemiological data. In this respect, a systematic review4 investigating geographic variations in microbial keratitis highlighted major differences. USA (Los Angeles)5 and Australia (Adelaide)6 reported the highest percentages of bacterial cases (95% in both countries); Paraguay7 had the highest percentage of Staphylococcal infection (79%). Thailand (Bangkok)8 reported the highest percentage of Pseudomonas infections (55%) while India (Tamil Nadu)9 reported the highest percentage of Streptococcal infections (47%).
Despite the publication of numerous clinical trials, there remains a lack of consensus as to which topical antibiotics and which regimen (ie, monotherapy or combination therapy) provide superior clinical outcomes. Therefore, the objective of this systematic review was to quantify the comparative effectiveness and safety of various topical antibiotics for BK.
Materials and methods
Eligibility criteria
A systematic review of randomised controlled trials was conducted comparing the effectiveness of different topical antibiotics in the management of patients with BK.
Types of participants
Participants were patients of any age or ethnicity diagnosed with bacterial infection of the cornea either by cultures or clinical judgment of diagnosing physician in either community-based or hospital-based settings.
Types of interventions
Trials were included that compared two or more topical ocular antibiotics administered for at least 7 days. Placebo controlled trials were excluded. While variability between dosing schedules was expected, all trials were expected to provide intensive topical ocular antibiotic cover (drops administered every 30–60 min) for the first 48 h followed by at least a 2–4-h regime by day, until day 5. Ocular antibiotics were then administered at the discretion of the treating physician. Permitted co-interventions included cycloplegics, glaucoma drugs, vitamins, oral analgesics, ocular lubricants, topical ocular corticosteroids and lid hygiene.
Types of outcomes
The primary outcome was treatment success, defined as complete re-epithelialisation of the cornea. Overall treatment success was reported at the conclusion of each trial in order to account for all participants. Secondary outcomes included time to cure (number of days treatment was instilled before physician's judgment designated BK as cured), adverse effects defined as any effects related to application of trial medication such as ocular discomfort (eg, pain, pruritus, burning, stinging, irritation), chemical conjunctivitis (eg, ocular/conjunctival toxicity or bulbar ulceration) or white precipitate, and serious complications of infection defined as complications requiring surgical intervention typically related to ocular bacterial infection rather than trial medication (eg, corneal perforation, therapeutic keratoplasty or enucleation).
Literature search
The following databases were searched for potential trials without language restriction: Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, MEDLINE, EMBASE, Scopus, BioMed Central, Trials Central, Clinical Trials, Controlled Clinical Trials, Web of Science, Latin American and Caribbean Health Sciences Literature (LILIACS) and relevant online medical journal websites. All databases were searched from the date of inception until the end of March 2013, and the reference lists of articles were also searched to identify potential trials of interest. The search strategy is available online as supplementary appendix 1. Authors of identified trials and pharmaceutical companies producing topical antibiotics were contacted for additional published, unpublished or ongoing trials. Authors of identified trials were also contacted if there were insufficient or missing data. This review was conducted following methodology guidance outlined in the Cochrane Handbook for Systematic Review.10 Review Manager 5.1 was used for meta-analysis.11
Data extraction and management
One reviewer conducted the electronic searchers. Two reviewers (EM and FR) independently selected trials for inclusion and assessed those that appeared potentially relevant. Full text articles were retrieved and translated where necessary. A third reviewer (CNJM) was available to arbitrate if there was failure in resolving disagreement between the first two reviewers. Random sequence generation, allocation concealment, masking of participants and personnel, masking of outcome assessment, incomplete outcome data and other identified bias of included trials were scored using the Cochrane Risk of Bias tool12 (see online supplementary figure S1).
Statistical analysis
Treatment differences were calculated using Mantel–Haenszel fixed-effect analysis,13 ,14 and random-effects analysis was to be used if there was evidence of statistical heterogeneity.12 Continuous outcomes were analysed using mean difference (MD) and reported with 95% CIs. Relative risk (RR) with 95% CI was reported for dichotomous outcomes. Where appropriate, the number needed to treat to benefit (NNTB) or harm (NNTH) and 95% CI were calculated.15 The NNT is the inverse of the absolute risk reduction. The NNTB gives a measure of the number of patients that need to be treated in order to provide the benefit outcome for one patient. Likewise, NNTH provides the same measure in order to prevent the harmful outcome to one patient.
Results
Trial selection and quality
Electronic searching yielded 27 957 abstracts, with 27 924 excluded as not relevant. The remaining 33 full text articles were obtained and independently reviewed by two authors, resulting in a further 17 trials being excluded. The remaining 16 trials,16–31 involving 1823 participants, were included as described in our Preferred Reporting of Systematic Reviews and Meta-Analysis (PRISMA) statement (figure 1). Two reviewers (EM and FR) were in full agreement regarding trial selection. Characteristics of included trials are reported in online supplementary table S1.

Summary of the trial flow and the meta-analysis profile as outlined in the Preferred Reporting of Systematic Reviews and Meta-Analysis statement.45 RCT: randomised controlled trial.
Assessment of risk of bias in included trials
Risk of bias summary of included trials is reported in online supplementary figure S1.
Random sequence generation and allocation concealment
Method of randomisation was clearly described and adequate in 12 trials.16 ,17 ,19–21 ,23 ,25–29 ,31 Four trials did not provide sufficient information with two described as randomised, double-masked, controlled trials,18 ,24 and two as randomised controlled trials.22 ,30 The overall risk of selection bias was low. Eight trials adequately described methods of allocation concealment.16 ,19 ,20 ,23 ,24 ,27 ,28 ,31
Masking
Nine trials were described as double-masked and provided methods for masking.16 ,19–21 23–27 Three of the trials were single-masked.17 ,28 ,31 Overall, the risk of detection bias was low.
Incomplete outcome data
All trials accounted for all participants. The risk of attrition bias was deemed to be low.
Other potential sources of bias
Six trials were funded by drug companies producing at least one of the trial drugs.17 ,20 ,21 ,23 ,25 ,26 Three trials reported no financial/conflict of interest,17 ,21 ,23 while two others did not provide sufficient information to ascertain level of drug company involvement.20 ,25 One trial stated their statistical analysis was funded by a drug company.26
Additional considerations
In all, 10 of the 14 trials16 ,19 ,21–25 27–,29 reporting treatment success had a study duration between 21 and 37 days with two trials allowing up to 90 days for follow-up.17 ,31 One trial20 reported treatment success by 14 days, while another did not specify study duration but measured treatment success at days 7 and 14.26 The study duration of one trial written in Portuguese was not stated in translation.30
Details for outcome comparisons are summarised in tables 1⇓⇓–4. There was no evidence of heterogeneity within any of the comparisons.
RR of treatment success with various topical antibiotics compared with fluoroquinolone or aminoglycoside–cephalosporin
MD in time to cure (days) with various topical antibiotics compared with fluoroquinolone or aminoglycoside–cephalosporin
RR of serious complications with various topical antibiotics compared with fluoroquinolone or aminoglycoside–cephalosporin
RR of adverse effects with various topical antibiotics compared with fluoroquinolone or aminoglycoside–cephalosporin
Treatment success
Treatment success was reported in each of the included trials as a dichotomous outcome at trial conclusion, although a few trials reported treatment success at specific time-points. There was no evidence of difference in RR of treatment success when moxifloxacin was compared with tobramycin–cefazolin28 ,31 (RR 1.02: 95% CI 0.91 to 1.14), when ciprofloxacin was compared with gentamicin–cefazolin22 ,30 (RR 1.11: 95% CI 0.84 to 1.45) or when moxifloxacin,17 ,28 ofloxacin17 ,23 ,24 ,26 or ciprofloxacin20 ,22 ,30 was compared with aminoglycoside–cephalosporin (RR 0.93: 95% CI 0.64 to 1.36; RR 0.94: 95% CI 0.68 to 1.30; and RR 1.02: 95% CI 0.83 to 1.25, respectively). There was also no evidence of difference in risk of treatment success when moxifloxacin,17 ,28 ofloxacin,17 ,27 ,29 ciprofloxacin,16 ,25 ,27 gatifloxacin25 ,28 or tobramycin–cefazolin17 ,20 ,23 ,24 ,28 were compared with fluoroquinolones (RR 1.02: 95% CI 0.58 to 1.80; RR 0.82: 95% CI 0.57 to 1.16; RR 1.44: 95%: 0.94 to 2.21; RR 0.76: 95% CI 0.40 to 1.44; and RR 1.03: 95% CI 0.85 to 1.24, respectively).
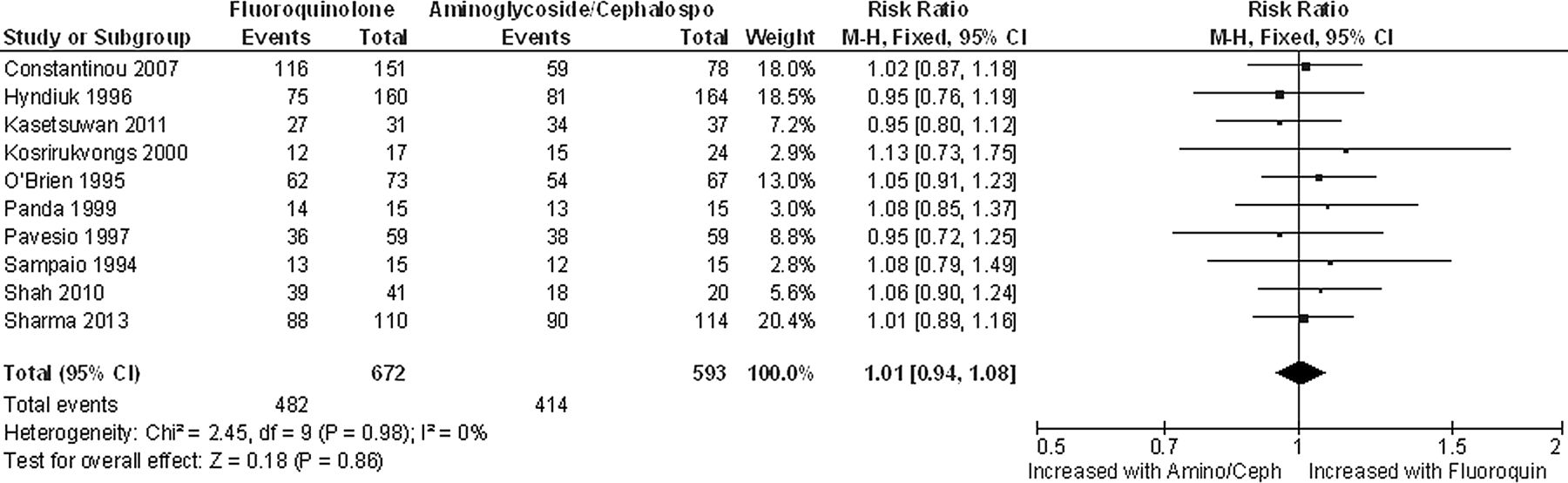
There was no evidence of difference in risk of treatment success when fluoroquinolones as a class were compared with aminoglycoside–cephalosporin in 10 trials17 ,20–24 ,26 ,28 ,30 ,31 with 1265 participants (RR 1.01: 95% CI 0.94 to 1.08). No evidence of significant heterogeneity was detected in trials comparing treatment success (table 1 and figure 2). Random-effects analysis did not provide results that differed from using fixed-effect analysis for treatment success.
{kind=link}
{kind=link}
Forrest plot for topical fluoroquinolone compared with topical fortified aminoglycoside–cephalosporin indicating no difference in chance of treatment success.
Time to cure
In order to provide context for the MD, the range of days to cure has also been provided for each treatment arm in table 2. There was no evidence of difference in mean time to cure when moxifloxacin17 ,28 or ofloxacin17 ,24 was compared with aminoglycoside–cephalosporin (MD −1.24: 95% CI −7.40 to 4.92 and MD 3.57: 95% CI −4.23 to 11.37, respectively), or when moxifloxacin,17 ,28 ofloxacin,17 ,27 ,28 ciprofloxacin,16 ,25 ,27 gatifloxacin,25 ,28 gentamicin–cefazolin19 ,22 or tobramycin–cefazolin17 ,24 ,28 were compared with fluoroquinolones (MD -4.30: 95% CI −10.86 to 2.25; MD 1.05: 95% CI −0.15 to 2.25; MD 1.14: 95% CI −0.51 to 2.79; MD −0.92: 95% CI −0.60 to 2.36; MD −1.97: −5.35 to 1.41; and MD 0.08: 95% CI −2.47 to 2.62, respectively).
There was no evidence of difference in mean time to cure when fluoroquinolones as a class were compared with aminoglycoside–cephalosporin in four trials17 ,19 ,24 ,28 with 259 participants (MD 2.09: 95% CI −1.26 to 5.44). There was no evidence of significant heterogeneity in this outcome measure (table 2).
Serious complications of infection
There was no evidence of difference in risk of corneal perforation when moxifloxacin,17 ,28 ofloxacin17 ,26 or fluoroquinolones as a class17 ,22 ,26 ,28 was compared with aminoglycoside–cephalosporin. There were also no evidence of difference in risk of perforation when ofloxacin17 ,27 or tobramycin–cefazolin17 ,28 were compared with fluoroquinolones. There was also no evidence of difference in risk of therapeutic keratoplasty when moxifloxacin was compared with tobramycin–cefazolin17 ,31 or when ofloxacin17 ,24 and fluoroquinolones as a class17 ,22 ,24 ,31 were compared with aminoglycoside–cephalosporin. Likewise, when tobramycin–cefazolin17 ,24 ,31 were compared with fluoroquinolone, there was no evidence of difference (table 3). There was no evidence of difference in risk of enucleation when fluoroquinolones17 ,22 were compared with aminoglycoside–cephalosporin. None of the comparisons reported evidence of significant heterogeneity (table 3).
Adverse effects of treatment
Ocular discomfort
When compared with aminoglycoside–cephalosporin in two trials,17 ,23 ofloxacin significantly reduced risk of ocular discomfort by 78% (292 participants, RR 0.22: 95% CI 0.13 to 0.39) with an NNTB of 4 (table 4). RR of ocular discomfort increased more than threefold when tobramycin–cefazolin were compared with fluoroquinolones in three trials17 ,20 ,23 that included 693 participants (RR 3.13: 95% CI 2.13 to 4.60) with an NNTH of 6. Fluoroquinolones reduced risk of ocular discomfort by 68% compared with aminoglycoside–cephalosporin in three trials17 ,20 ,23 (693 participants, RR 0.32: 95% CI 0.22 to 0.47) with an NNTB of 6.
Chemical conjunctivitis
When ofloxacin was compared with aminoglycoside–cephalosporin in three trials17 ,23 ,26 risk of chemical conjunctivitis was reduced by 80% (410 participants, RR 0.20: 95% CI 0.10 to 0.41) with an NNTB of 7. There was no evidence of difference in risk of chemical conjunctivitis when tobramycin–cefazolin were compared with fluoroquinolones in two trials.17 ,23
White precipitate
The risk of white precipitate formation increased 24-fold with ciprofloxacin compared with aminoglycoside–cephalosporin in three trials20 ,22 ,30 (395 participants, RR 24.37: 95% CI 4.68 to 126.89) with an NNTH of 6. There was no evidence of heterogeneity in trials comparing ocular discomfort, chemical conjunctivitis or white precipitate.
Discussion
This review found no evidence of difference in comparative effectiveness of topical ocular antibiotics. However, combination therapy, particularly with tobramycin–cefazolin, provided evidence of increased risk of ocular discomfort up to 78%, compared with fluoroquinolones. Moreover, there was evidence that combination therapy increased the risk of chemical conjunctivitis 80% compared with ofloxacin while ciprofloxacin increased the risk of white precipitate 24-fold compared with combination therapy.
Standard treatment for BK, particularly in severe infections, often consists of intensive aminoglycoside–cephalosporin combinations. This particular combination covers a broad range of Gram negative and positive pathogens while awaiting culture results and clinical response. Although the results of this review report no evidence of difference between combination therapy and fluoroquinolones, variability has been described in pathogen susceptibility among topical ocular antibiotics with increased resistance of Pseudomonas aeruginosa and Staphylococcus aureus to fluoroquinolones in various geographical areas, particularly the Indian subcontinent.32 A possible reason for increased resistance in this region may be attributable to widespread systemic use for infections and prophylaxis, and availability of over-the-counter antibiotics,33 although there was no evidence of this in any of the included trials conducted in India.
An important component of treatment success is patient compliance. Clinical trials are conducted under ideal conditions where eye-drop storage, administration and regime are monitored closely and documented. In reality, patients may be more compliant with fluoroquinolones than combination therapy due to storage at room temperature, one drop required per dose and minimal ocular discomfort or chemical conjunctivitis.
This meta-analysis did not find evidence of difference in risk of corneal perforation with fluoroquinolones compared with combination therapy in 449 patients.17 ,22 ,26 ,28 The fluoroquinolones included in this outcome were ofloxacin, ciprofloxacin, gatifloxacin and moxifloxacin. Perforations were not reported in trials comparing either lomefloxacin or levofloxacin with combination therapy. That said, in vitro studies have observed cytotoxic effects on corneal keratocytes under the influence of fluoroquinolones, with ciprofloxacin cited as most cytotoxic.34 It is therefore possible that changes in corneal keratocytes resulting from stromal inflammation35 and exposure to fluoroquinolones34 could contribute to corneal perforation.
The current review found no evidence of difference in the risk of therapeutic keratoplasty in BK when moxifloxacin or ofloxacin was compared with combination therapy or when fortified tobramycin–cefazolin were compared with fluoroquinolones. As a class, fluoroquinolones did not increase risk of therapeutic keratoplasty compared with combination therapy. There was also no evidence of difference in risk of enucleation with fluoroquinolones compared with combination therapy. This may indicate a comparable degree of ulceration and severity of infection in the study groups compared. Only one trial17 exclusively recruited patients with severe infection, although the definition of severe was not outlined in their protocol.
Ofloxacin reduced the risk of ocular discomfort by 78% compared with combination therapy. However, compared with fluoroquinolones, no evidence of difference in risk was noted. Tobramycin–cefazolin increased the risk of ocular discomfort threefold compared with fluoroquinolones. The three trials comprising this outcome identified predominant Gram positive infection, most commonly Staphylococci. Two of the trials used comparable drug concentrations for both fluoroquinolones and combination therapy. However, O'Brien and colleagues23 used an increased concentration of tobramycin (1.5% compared with 1.3%) and cefazolin (10% compared with 5%), and increased dosing frequency (every 30 min compared with hourly) for the first 48 h, which could have influenced this result. However, when this study was removed from analysis, the increased risk of ocular discomfort with combination therapy remained. Ocular discomfort may also exist with other aminoglycoside–cephalosporin combinations but cannot be substantiated due to paucity of randomised controlled trials. As a class, fluoroquinolones reduced the risk of ocular discomfort by 66% compared with combination therapy. These results are in agreement with current literature as fortified combination therapy has been documented to cause increased corneal irritation and possible delay in corneal epithelialisation.36–38 However, one of the trials included in the review21 found faster corneal re-epithelialisation with cefazolin–amikacin compared with levofloxacin. This may be due to the absence of either gentamicin or tobramycin, both of which have been identified to cause delay in corneal re-epithelialisation.36 ,39
Ofloxacin reduced the risk of chemical conjunctivitis by 80% compared with combination therapy.17 ,23 ,26 It is possible that the inclusion of a study26 using fortified gentamicin 1.5% and cefuroxime 5% contributed significantly to this result as this effect disappeared when the study was removed. Moreover, the risk of chemical conjunctivitis did not increase with tobramycin–cefazolin compared with fluoroquinolones.17 ,23 It is interesting to note that while tobramycin–cefazolin had a threefold increased risk of ocular discomfort compared with fluoroquinolones, this did not equate to an increased risk of chemical conjunctivitis and did not impact on treatment success, time to cure or serious complications of infection. As noted in previous trials,16 ,40–44 the current meta-analysis confirms an increased risk of white precipitate formation with ciprofloxacin, which resolves following treatment discontinuation.
While included trials did not provide cost analysis, it is important to consider accessibility and time to treatment. Fluoroquinolones are generally dispensed from hospital and community pharmacies and can be kept at room temperature. Fortified aminoglycoside–cephalosporins are prepared in compounding pharmacies and must remain refrigerated as they have a shelf life of approximately 4 days. A drop of each medication needs to be given at least 5 min apart hourly, which has resource implications. The time involved preparing fortified antibiotics is also a consideration when patients present with severe bacterial infection such as P aeruginosa requiring immediate intervention. The current review also reported fortified aminoglycoside–cephalosporin to cause more ocular discomfort than fluoroquinolones which can decrease patient compliance with recommended dosing schedules—leading to ineffective bacterial inhibition.
Implications for further research
There is a paucity of trials comparing differing combinations of aminoglycoside–cephalosporin other than tobramycin–cefazolin. Of interest is a possible increased risk of chemical conjunctivitis with gentamicin–cefuroxime compared with ofloxacin, and a faster time to cure with amikacin–cefazolin and levofloxacin compared with ofloxacin. However, single trials have reported these outcomes.
Clinical recommendations
This extensive study of high quality randomised controlled trials evaluating the effectiveness of topical antibiotics in the management of BK reports no evidence of difference in risk of treatment success, time to cure or serious complications of infection when fluoroquinolones were compared with fortified aminoglycoside–cephalosporin in intensive topical regimens.
While fluoroquinolones reduced the risk of ocular discomfort and ofloxacin reduced the risk of chemical conjunctivitis, this did not impact on other important clinical outcomes. Therefore, we report no evidence of difference in comparative effectiveness between fluoroquinolone and aminoglycoside–cephalosporin intensive regimens in the management of patients presenting with BK.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online figure
- Data supplement 3 - Online table
Footnotes
-
Contributors EMM, FSFR, DVP, CNJM: conception and design of study. EMM, FSFR: literature search for included studies. EMM, FSFR: analysis and interpretation of data. EMM, FSFR, CNJM, DVP: drafting the article. EMM, FSFR, CNJM, DVP: revising manuscript critically for important intellectual content. EMM, FSFR, CNJM, DVP: final approval of the version to be published. The corresponding author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.