Article Text

Abstract
Purpose To investigate the appearance of medium–large drusen and reticular pseudodrusen on adaptive optics (AO).
Methods In 14 consecutive patients, AO infrared (IR) images were overlaid with confocal scanning-laser-ophthalmoscope IR reflectance images and IR-referenced spectral-domain optical coherence tomography.
Results In eight eyes of six patients, a total of 19 images of medium–large drusen were investigated by AO imaging. En face AO revealed medium–large drusen as highly hyper-reflective round/oval lesions, always centred and/or surrounded by a continuous/discontinuous hyporeflectivity. Cone photoreceptors were detected overlying drusen, appearing either as continuous ‘bright’ hyper-reflective dots over a ‘dark’ hyporeflective background, or as continuous ‘dark’ hyporeflective dots over a ‘bright’ hyper-reflective background. In eight eyes from eight patients, a total of 14 images of pseudodrusen were investigated by AO imaging. En face AO revealed reticular pseudodrusen as isoreflective lesions, always surrounded by a continuous/discontinuous hyporeflectivity. Cone photoreceptors were detected overlying pseudodrusen as ‘bright’ hyper-reflective dots over either a hyporeflective or isoreflective background. No ‘dark’ hyporeflective dots were detected in eyes with reticular pseudodrusen only. Cone photoreceptors were counted on the border of the drusen and pseudodrusen, respectively, and in a visibly healthy zone in its absolute vicinity. A similar decrease in cone appearance was observed for drusen and pseudodrusen (15.7% vs 16.2%).
Conclusions AO allows differences in reflectivity between medium–large drusen and reticular pseudodrusen to be appreciated. The cone mosaics may be detected as continuous ‘bright’ hyper-reflective dots overlying/on the border of drusen and pseudodrusen deposits, and possibly as continuous ‘dark’ hyporeflective dots overlying drusen only.
- Imaging
- Retina
Statistics from Altmetric.com
Introduction
In age-related macular degeneration (AMD), material between the basal lamina of the retinal pigment epithelium (RPE) and the inner collagenous layer of Bruch's membrane is generally referred to as drusen.1 Our group initially characterised reticular pseudodrusen in 1990.2 This is a peculiar, yellow pattern visible in the macula of patients with AMD. Advances in integrated imaging technology recently permitted our group to better characterise the centre of the reticular yellowish pattern on spectral-domain optical coherence tomography (SD-OCT). This region is characterised by discrete agglomerations of hyper-reflective material located above the RPE (ie, the pseudodrusen deposits, also known as subretinal drusenoid deposits).3–9 Patients with AMD, however, typically exhibit agglomerations of hyper-reflective material under the RPE. Histopathological studies10 and integrated imaging approaches5–9 have led several groups to propose that pseudodrusen deposits are the result of fibrosis and atrophy of the choroid. These lead to RPE derangement and secondary accumulation of photoreceptor outer segments above the RPE. Of particular note, the peripheral features of pseudodrusen deposits are defined on SD-OCT by the loss of outer segment (OS)/RPE interface and inner segment (IS)/OS interface5 ,6 (also known as ellipsoid zone).11
However, on infrared (IR) reflectance, the pseudodrusen deposit peripheral features appear as hyper-reflective halos (target aspect). In a recent study, our group demonstrated significantly reduced retinal sensitivity in eyes with reticular pseudodrusen compared with eyes with typical drusen.12 Interestingly, reduced sensitivity seems to match with areas of apparent distribution of reticular pseudodrusen.12 ,13 This could be explained by a widespread disruption and loss of RPE and photoreceptors on the IS/OS interface associated with pseudodrusen deposits5–9 ,14 rather than a focal outer retina impairment overlying drusen.15–18
In conventional imaging systems, lateral resolution is limited by the numerical aperture of the system used and the optical aberrations of the human eye. Adaptive Optics (AO) imaging systems improve the transverse resolution of retinal imaging. They do this by measuring the ocular wavefront aberrations and compensating for them in real time with active optical elements.19 ,20 Because the lateral resolution of retinal images is improved to the order of 2 μm, detailed analysis of macular lesions and cone photoreceptor appearance can be performed in vivo.
In this study, we investigated the appearance of medium–large drusen and reticular pseudodrusen on AO, in non-neovascular AMD.
Methods
Study population
Fourteen consecutive patients with medium–large drusen only or reticular pseudodrusen only who presented at the Retinal Service of the University Eye Clinic of Creteil between June and July 2013 were sent for AO imaging. Medium–large drusen are defined by discrete mound-like accumulation of material between the basal lamina of the RPE and the inner collagenous layer of Bruch's membrane. They appear on funduscopic examination as yellow-white deposits within the macula. Confocal scanning laser ophthalmoscope (cSLO) IR reflectance shows a subtle variation in the greyscale tones in regions containing medium–large drusen, and SD-OCT reveals discrete mound-like, mildly reflective elevation of the RPE. Reticular pseudodrusen deposits are defined by discrete agglomerations of material above the RPE, appearing on fundus examination as a yellow pattern within the macula (the visibility of which is enhanced by cSLO IR reflectance). On SD-OCT, pseudodrusen deposits appear as well defined round or triangular hyper-reflective lesions above the RPE. There is apparent loss of OS/RPE interface and IS/OS interface on their borders (which is responsible for the hyper-reflective halos and thus the target aspect on cSLO IR reflectance).
Inclusion criteria were age >50 years; presence of medium–large drusen (≥63 μm) or reticular pseudodrusen as a manifestation of non-neovascular AMD in at least one eye (no evidence of choroidal neovascularisation (CNV) on fluorescein angiography and indocyanine green angiography; no intraretinal or subretinal fluid; and no sub-RPE/retinal haemorrhage). Exclusion criteria were: signs of any other retinal disease in the study eye, such as retinal vascular disease (ie, diabetic retinopathy and retinal vein occlusion) or vitreoretinal disease (ie, vitreomacular traction syndrome and epiretinal membrane); presence of geographic atrophy; presence of CNV; any prior treatment (eg, laser photocoagulation, photodynamic therapy, intravitreal injections of steroids, or anti-vascular endothelial growth factor); and high myopia (>6 dioptres). Our study was performed in agreement with French bioethical legislation and the Declaration of Helsinki for research involving human subjects. French Society of Ophthalmology Ethics Committee approval was obtained for this study.
Study protocol
All patients underwent a complete ophthalmologic examination that included best-corrected visual acuity (BCVA) using standard Early Treatment of Diabetic Retinopathy Study, fundus examination, cSLO IR reflectance, and tracked Spectralis SD-OCT (Spectralis real-time eye-tracking technology). The cSLO IR reflectance images were acquired with a 815 nm wavelength (Spectralis SD-OCT, Heidelberg Engineering, Heidelberg, Germany), and automatic real-time averaging was used to minimise noise. High-resolution SD-OCT images were acquired with Spectralis SD-OCT, a high-speed OCT system (up to 40 000 axial scans per second) using spectral/Fourier domain detection, with an optical axial image resolution of 7 μm. In Spectralis SD-OCT, cSLO with real-time eye tracking technology allows one to track the eye and guide OCT to the selected location, thus giving a real-time reference for locating the SD-OCT scan. The SD-OCT minimum acquisition protocol covered a 6×6 mm area composed of 19 horizontal lines (each with nine averaged OCT B scans, 1024 A scans per line, at 240 mm intervals). IR images of medium–large drusen and reticular pseudodrusen guided the acquisition of additional high-resolution 9 mm single B scans (each composed of up to 100 averaged enhanced depth imaging OCT B scans). All patients also underwent flood illumination AO IR fundus imaging using an AO retinal camera (rtx1; Imagine Eyes, Orsay, France). This instrument is the first commercially available compact AO fundus camera. It permits imaging of the retina at a cellular scale. The rtx1 is based on a flood illumination apparatus working at 850 nm in mydriatic condition if the pupil size of the patient is over 4 mm. The aberrations of the patients are measured by a Shack–Hartman Wavefront sensor (Haso32-Eye, Imagine Eyes, France) with a light source at 780 nm. A 52 actuator electromagnetic deformable mirror (mirao52e, Imagine Eyes) corrects the measured aberrations. An 850 nm LED lights the fundus of the eye and a low noise CCD camera captures the raw images of the retina at 10 Hz over a 4°×4° field of view. Adjustment in depth inside the retina is possible to choose the structures to image. Sets of 40 short exposure time images are recorded to obtain one improved final image. That final image is the result of an automatic registration performed by software provided by the manufacturer (CK V.0.1, Imagine Eyes).
AO imaging analysis
Photoshop (Photoshop CS4, Adobe System Inc, San Jose, California, USA) was used to manually overlay AO IR images with cSLO IR reflectance images using the retinal vessels as landmarks. The correlation feature of Spectralis (Heidelberg Eye Explorer software, V.1.7.0.0, Heidelberg Engineering) was used to establish the correspondence of en face AO features, including cone appearance, with medium–large drusen and pseudodrusen deposits, as visualised by cSLO IR-referenced SD-OCT scans (Spectralis real-time eye-tracking technology).
Qualitative description of AO features for SD-OCT-matched medium–large drusen and pseudodrusen deposits was performed by two senior retinal physicians (GQ and EHS). The position of the photoreceptors was computed by the manufacturer's software (AO Detect Mosaic V.0.1, Imagine Eyes, France). That software detects ‘bright’ hyper-reflective dots (small circular spots with a different brightness from the surrounding background level). The spatial distribution of the centres of these spots was analysed in terms of local cell numerical density (cells per square millimetre of retinal surface). Photoreceptors were counted on the border of medium–large drusen and pseudodrusen deposits, respectively, and in a visibly healthy zone in its absolute vicinity. This was performed to limit the causes impacting reflectivity and thus visualisation of cones in the AO images, including a change in orientation over medium–large drusen and pseudodrusen deposits.
Statistical analysis
Data were analysed with the Statistical Package for the Social Sciences V.20.0 for Mac (IBM, Chicago, Illinois, USA). The analysis included descriptive statistics for demographic data and a qualitative and quantitative description of the findings. Continuous variables were reported as means±SD. Student's t test for paired data was used for means comparison. Fisher exact test was used for categorical variables. A significant p value was <0.05.
Results
In eight eyes of six patients (one man and five women; mean age 65.3±14.9 years; BCVA range 20/20–20/40) a total of 19 images of medium–large drusen were investigated by AO imaging. All AO images were sized 4°×4°, and localised between 8.2°t and 8.2°n, and between 6.3°s and 5.6°i. En face AO revealed medium–large drusen as highly hyper-reflective round/oval lesions, always centred and/or surrounded by a continuous/discontinuous hyporeflectivity (figure 1A–D). Cone photoreceptors, appearing as continuous ‘bright’ hyper-reflective dots over a ‘dark’ hyporeflective background (ie, cone mosaics), were unambiguously detected overlying and on the border of medium–large drusen (figure 1A–D). Interestingly, continuous ‘dark’ hyporeflective dots over a ’bright’ hyper-reflective background were also detected in three eyes of three patients (in the same 11 images showing coincident ‘bright’ hyper-reflective dots) overlying medium–large drusen (figure 1B,D).
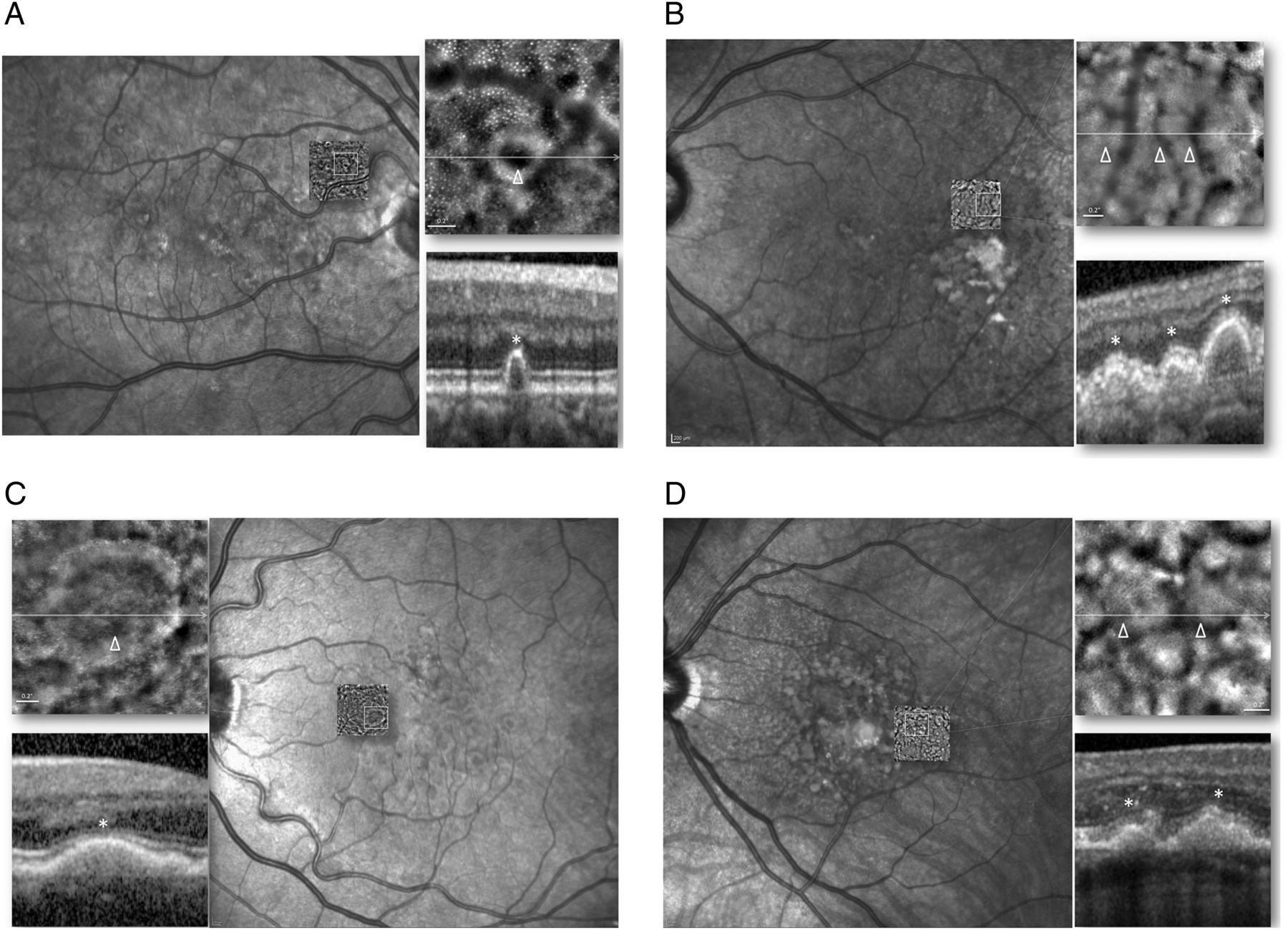
En face adaptive optics (AO) imaging overlaid with confocal scanning laser ophthalmoscope (cSLO) infrared (IR) reflectance, and cSLO IR-referenced spectral-domain optical coherence tomography (SD-OCT) scans in patients with medium–large drusen (patient 3, right eye (A); patient 1, left eye (B); patient 6, left eye (C); patient 4, left eye (D)). En face AO shows medium–large drusen as highly hyper-reflective round/oval lesions centred and surrounded by a discontinuous hyporeflectivity (A–D). Cone photoreceptors, appearing as continuous ‘bright’ hyper-reflective dots over a ‘dark’ hyporeflective background, may be unambiguously detected overlying and on the border of medium–large drusen (A–D, enlarged view). Continuous ‘dark’ hyporeflective dots over a ‘bright’ hyper-reflective background may also be detected overlying medium–large drusen (B and D, enlarged view). Irregularities within the cone mosaic and reduced cone reflectivity can be noted over medium–large drusen (A–D) on en face AO. The hyporeflective AO signal corresponds with hyporeflectivity of the inner segment/outer segment interface in SD-OCT images directly overlying medium–large drusen (A–D, enlarged view (arrowheads and asterisks)).
In eight eyes from eight patients (all women; mean age 79.3±6.6 years; BCVA range 20/20–20/50) a total of 14 images of pseudodrusen were investigated by AO imaging. All AO images were sized 4°×4°, and localised between 7.6°t and 5.9°n, and between 6.3°s and 8.1°i. En face AO revealed pseudodrusen deposits as isoreflective lesions, always surrounded by a continuous/discontinuous hyporeflectivity (ie, hyporeflective halo) (figure 2A–D). Cone photoreceptors, appearing as ‘bright’ hyper-reflective dots over either a hyporeflective or isoreflective background, were unambiguously detected overlying and on the border of pseudodrusen deposits (figure 2A–D). Unlike in medium–large drusen, no ‘dark’ hyporeflective dots were detected in eyes with reticular pseudodrusen only. In all eyes, the hyporeflective halo detected on en face AO corresponded with loss of the IS/OS interface in SD-OCT images (figure 2A–D).

{kind=link}
{kind=link}
En face adaptive optics (AO) imaging overlaid with confocal scanning laser ophthalmoscope (cSLO) infrared (IR) reflectance, and cSLO IR-referenced spectral-domain optical coherence tomography (SD-OCT) scans in patients with reticular pseudodrusen (patient 9, right eye (A); patient 7, right eye (B); patient 10, left eye (C); patient 12, right eye (D)). En face AO shows pseudodrusen deposits as isoreflective lesions, surrounded by a hyporeflective halo (A–D). Cone photoreceptors, appearing as ‘bright’ hyper-reflective dots over either a hyporeflective or isoreflective background may be unambiguously detected overlying and on the border of pseudodrusen deposits (A–D, enlarged view). Irregularities within the cone mosaic and reduced cone reflectivity can be noted over pseudodrusen deposits (A–D) on en face AO. The hyporeflective AO signal corresponds with hyporeflectivity of the inner segment/outer segment interface in SD-OCT images directly overlying pseudodrusen (A–D, enlarged view (arrowheads and asterisks)).
In all eyes, subtle irregularities within the cone mosaic and reduced cone reflectivity were noted over medium–large drusen and pseudodrusen deposits on en face AO. The hyporeflective AO signal corresponded with hyporeflectivity of the IS/OS interface in SD-OCT images directly overlying medium–large drusen and pseudodrusen (figures 1 and 2).
Cone photoreceptors were counted on the border of the medium–large drusen and pseudodrusen deposits, respectively, and in a visibly healthy zone in its absolute vicinity. A similar decrease in cone appearance was observed for medium–large drusen and pseudodrusen (15.7% vs 16.2%) (table 1).
Demographics and clinical features of patients with medium–large drusen and with reticular pseudodrusen
Discussion
In this study, we investigated the appearance of medium–large drusen and reticular pseudodrusen on AO in non-neovascular AMD. Overall, medium–large drusen appeared on en face AO images as highly hyper-reflective round/oval lesions, centred and/or surrounded by a continuous/discontinuous hyporeflectivity. However, pseudodrusen deposits appeared as isoreflective lesions, surrounded by a continuous/discontinuous hyporeflective halo. We used the correlation feature of Spectralis to establish the correspondence of AO images with medium–large drusen and pseudodrusen deposits, as visualised by cSLO IR-referenced SD-OCT scans. These differences in the overall appearance on en face AO imaging further support current in vivo evidence that medium-large drusen and reticular pseudodrusen exhibit different localisations of material collections (ie, under vs above the RPE).3–9
AO also allowed us to describe the ultrastructural features of medium–large drusen and reticular pseudodrusen. Particularly, continuous ‘bright’ hyper-reflective dots over a ‘dark’ hyporeflective background, or an isoreflective background, presumably representing the cone mosaics, were unambiguously detected overlying/on the border of medium–large drusen and pseudodrusen deposits, respectively. However, subtle irregularities within the cone mosaic were noted in all eyes over medium–large drusen and pseudodrusen deposits on en face AO. Moreover, the hyporeflective AO signal corresponded with hyporeflectivity of the IS/OS interface in SD-OCT images directly overlying medium–large drusen and pseudodrusen. Interestingly, in three eyes, continuous ‘dark’ hyporeflective dots over a ‘bright’ hyper-reflective background were also detected overlying (only) medium–large drusen. This finding has never been reported in previous analyses of AO images in normal and diseased eyes. ‘Dark’ hyporeflective and ‘bright’ hyper-reflective dots (detected over a ‘bright’ hyper-reflective and a ‘dark’ hyporeflective background, respectively) were coincident, and both showed a continuous appearance. We hypothesise that they may represent different AO presentations of cone mosaics, possibly related to variable AO IR signal reflectivity originating from variably elevated RPE (due to sub-RPE material accumulation). Of note, ‘dark’ hyporeflective dots were not detected in eyes with reticular pseudodrusen, suggesting that in the absence of RPE elevation, this peculiar presentation of cone mosaics cannot be visualised on AO images.
In the current analysis, to limit the causes impacting reflectivity, and thus visualisation of cones in the AO images (ie, change in orientation over medium–large drusen and pseudodrusen deposits), cone photoreceptors were counted on the border of medium–large drusen and pseudodrusen deposits, respectively, and in a visibly healthy zone in its absolute vicinity. Overall, we observed a similar decrease in cone appearance for medium–large drusen and pseudodrusen (15.7% vs 16.2%). It is noteworthy that cone photoreceptors were computed by automatically detecting the central coordinates of ‘bright’ hyper-reflective dots (the brightness of which differed from the surrounding background level). However, given that this was performed on the border of medium–large drusen and pseudodrusen deposits, we believe that the computation of automatically detected ‘bright’ hyper-reflective dots was not influenced by either the change in orientation of cones (because they are typically irrelevant on the border of medium–large drusen and pseudodrusen deposits), or by the ‘dark’ hyporeflective dots (because they are typically absent in these locations without RPE elevation).
Previous evaluations of cone mosaics over medium–large drusen revealed that reduction in cone packing density over conventional drusen is modest.21–24 In a recently published study, cone packing density over pseudodrusen deposits was distinctly decreased compared with that over conventional drusen.24 In the current study, we also found only a modest decrease in cones, which was similar for medium–large drusen and pseudodrusen. However, considering that in our analysis we investigated cone photoreceptors on the border of and not over medium–large drusen and pseudodrusen deposits, this makes any comparison actually impossible.
Nonetheless, assuming that we limited the causes impacting reflectivity, and thus visualisation of cones in the AO images, our study further supports the concept of a modest decrease in cones in the presence of medium–large drusen and pseudodrusen. The widespread disruption and loss of the photoreceptor IS/OS interface5–9 ,14 and the reduced retinal sensitivity in eyes with reticular pseudodrusen compared with eyes with typical drusen12 ,13 may be at least in part related to impaired rod photoreceptors (which were not visualised in this study). Local electroretinography activity from the cone-driven retina in eyes harbouring reticular pseudodrusen was recently investigated by Alten et al25 utilising a multifocal electroretinogram approach. Definite interference of electrophysiological activity in reticular pseudodrusen-affected retinal regions was not demonstrated using multifocal electroretinogram measurements.25 Conversely, a recent study utilising microperimetry to assess macular function revealed reduced retinal sensitivity in eyes with reticular pseudodrusen compared with eyes with typical drusen. Dark adaptation was employed in this study to facilitate the investigation of cone and rod activity. These data suggest that cone-driven function and rod-driven function (possibly, primarily rod-driven function) are diminished in patients with reticular pseudodrusen.12
No histological data exist providing an insight into the biological substrate of centrally reflective/fluorescent lesions (target aspect) as visualised on cSLO imaging, corresponding to pseudodrusen deposits.5 Possibly, the hyporeflective halo, as visualised on AO imaging, might consist of deflected photoreceptors while the isoreflective central lesion might consist of unphagocytosed photoreceptor outer segments. A hyper-reflective signal on cSLO IR reflectance has been previously described by our group for conventional drusen with RPE alterations.26 In a study of autofluorescence imaging in large drusen, Landa et al27 suggested that hypoautofluorescent and hyperautofluorescent changes mostly correlate with the disruption of the overlying IS/OS layer. Current data from AO support the idea that different degrees of impairment in the RPE and photoreceptors could be responsible for the different imaging features recorded between medium–large drusen and reticular pseudodrusen. In other words, the status of the RPE and IS/OS layer appears to be equally important in reticular pseudodrusen and conventional drusen regarding their imaging properties (highly hyper-reflective round/oval lesions, centred and/or surrounded by a continuous/discontinuous hyporeflectivity, and isoreflective lesions, surrounded by a continuous/discontinuous hyporeflective halo, respectively).
Therefore, utilising multiple imaging technologies may enable a more definitive understanding of the prognostic value of these lesions28–30 and their respective clinical impact on macular function.12
Our study is not without limitations, which are mainly due to the small number of included eyes and the lack of normative data on AO features of the macula.
In conclusion, AO allows differences in reflectivity between medium–large drusen and reticular pseudodrusen to be appreciated. The cone mosaics may be unambiguously detected as continuous ‘bright’ hyper-reflective dots overlying/on the border of medium–large drusen and pseudodrusen deposits, and possibly as continuous ‘dark’ hyporeflective dots overlying medium–large drusen only. However, a similar decrease in cone photoreceptors is observed on the border of medium–large drusen and pseudodrusen. These findings may yield insights into the pathophysiology of different non-neovascular AMD phenotypes.
Acknowledgments
We would like to thank Samuel Levy, MD for editorial support.
References
Footnotes
-
Contributors Study design and conduct (GQ, EHS); data collection, management, analysis (CKL, AG, AP, RBG, VC, FP GQ, EHS), and interpretation (CKL, AG, AP, RBG, VC, FP GQ, EHS); manuscript preparation, review, or approval (GQ, ES).
-
Competing interests None.
-
Ethics approval French Society of Ophthalmology Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.