Article Text

Abstract
Background/Aim To describe an optical coherence tomography angiography (OCTA) system adapted for anterior segment imaging, compared with indocyanine green angiography (ICGA) in eyes with corneal vascularisation.
Methods Retrospective study of subjects with corneal vascularisation secondary to microbial keratitis who had OCTA scans performed using a commercially available split-spectrum amplitude-decorrelation algorithm angiography system (AngioVue; Optovue Inc., Fremont, California, USA) and ICGA images (Spectralis; Heidelberg Engineering, Heidelberg, Germany). The agreement between OCTA and ICGA techniques in terms of area of vascularisation measured, using Bland–Altman 95% limits of agreement (LOA).
Results We compared the area of corneal vascularisation in 64 scan images (eight eyes, four scans for each angiography technique). In our series, the overall mean area of vascularisation from the ICGA scans was 0.49±0.34 mm2 and OCTA scans was 0.51±0.36 mm2. We obtained substantial repeatability in terms of image quality score (κ=0.80) for all OCTA scans. The agreement between OCTA and ICGA scans was good, although ICGA measured a smaller area compared with the OCTA with a mean difference of −0.03 mm2 (95% CI −0.07 to 0.01). The LOA ranged from a lower limit of −0.27 (95% CI −0.34 to −0.19) to an upper limit of 0.20 (95% CI 0.13 to 0.28, p=0.127).
Conclusions We found that rapid, non-contact OCTA adapted for the cornea was comparable with ICGA for measurement of the area of corneal vascularisation in this pilot clinical study. Further prospective studies are required to confirm if this relatively new imaging technique may be further developed to replace invasive angiography techniques for the anterior segment.
- Cornea
- Imaging
- Neovascularisation
Statistics from Altmetric.com
Introduction
Angiography for the anterior segment has a variety of clinical applications, ranging from the evaluation of corneal and scleral inflammatory disorders1 ,2 to guiding the treatment of corneal vascularisation.3 Fluorescein angiography (FA) and indocyanine green angiography (ICGA) have already been described for imaging both normal and abnormal corneoscleral vessels.1–5 Although fluorescein rapidly fills and delineates vessels during the first transit of dye, subsequent leakage through the normal fenestrated capillaries in the conjunctiva prevents visualisation of any deeper vessels.4 On the other hand, indocyanine green (ICG) is primarily bound by proteins and remains in the vessels for a longer time and leaks only in the presence of damage or inflammation.5 Despite the potential advantages and clinical indications of both techniques, the clinical use of these angiography methods has been limited due to their invasive nature and infrequent but potentially severe, adverse events.6
Recently, optical coherence tomography angiography (OCTA) has been used to successfully delineate vessels within the retina, choroid and the vasculature associated with the optic nerve.7–11 These non-contact imaging systems detect phase variations or changes in reflectivity to detect vascular flow, with the added benefit of concurrently obtaining optical coherence tomography (OCT) scans of the surrounding tissue.12 This allows for rapid, non-invasive evaluation of ocular pathologies with their associated vessels, exemplified by OCTA assessment of choroidal neovascularisation with the evaluation of surrounding choroidal and retinal layers simultaneously.13 In particular, split-spectrum amplitude-decorrelation angiography (SSADA) improves the signal-to-noise ratio of flow detection and has been shown to be useful for visualising the microvasculature networks within the eye.12
Since current OCTA systems are optimised for the retina and optic disc, we had previously described a technique adapted to perform scans in the anterior segment for normal corneal and limbal vessels.14 As objective evaluation of corneal vascularisation is becoming increasingly important for its diagnosis and monitoring, new non-invasive imaging modalities are a welcome addition to our clinical practice.15 However, while the OCTA system rapidly produced angiograms of the corneal and limbal vasculature with substantial consistency,14 its role in evaluating abnormal corneal vessels in comparison with current angiography techniques has not been established. Thus, we conducted this pilot clinical study to evaluate the same OCTA technique adapted for cornea and compared it with anterior segment ICGA—reported to be more useful than FA for delineating pathological corneal vessels.16
Materials and methods
In this observational study, we conducted a retrospective review of subjects with corneal vascularisation at Moorfields Eye Hospital from 1 December 2014 to 30 May 2015. We included patients with corneal vascularisation secondary to microbial keratitis; extending more than 3 mm from the limbus into the cornea with significant corneal lipid keratopathy and scarring; which did not respond to topical steroid therapy for at least 12 weeks and were planned to undergo fine-needle diathermy. Eyes with active inflammation, infection or ulceration were excluded. After the specific areas of corneal vascularisation for study were identified, photographs were taken using digital slit-lamp cameras (Topcon ATE-600, with D1X digital camera, Nikon Corp) with a standard diffuse illumination (×10 magnification, flash power 4, 45° angle). Our study followed the principles of the Declaration of Helsinki .
Angiography technique
A standard technique was used for anterior segment ICGA using the Heidelberg scanning laser ophthalmoscope (Heidelberg Engineering, Heidelberg, Germany) in ‘Hi-Res Mode’, using a 20° field of view with the focus setting on ‘+32.00 D’. Infrared images were captured before slow injection of 5 mL of ICG dye (5 mg/mL at 1 mL/s) and the video was recorded for 30 s, followed by single-frame ICGA images of the whole cornea every 10 s for 3 min. Four of the ICGA latest frames were chosen once the image was stable with no increase or visible leakage. All eyes then had four 6×6 mm scans of the identified area of corneal vascularisation on a separate day at least 1 week apart, using the AngioVue OCTA system (Optovue Inc., Fremont, California, USA) with the long corneal adaptor module (CAM-L) using a previously described technique.14 In the OCTA system used for this study, the autofocus function had to be deactivated, and the lens moved very close (2–3 cm) to the corneal surface before fine-tuning and manual adjustments to the focal lengths were made to achieve adequate focus on the area of interest in the cornea. Scans had transverse resolution of 15 μm and axial resolution of 5 μm using a light source centred on 840 nm with the beam width of 22 μm. Coronal or ‘en face’ OCTA scan images were reconstructed from 304×304 A-scans captured at 70 000 scans per second.17
Image analysis
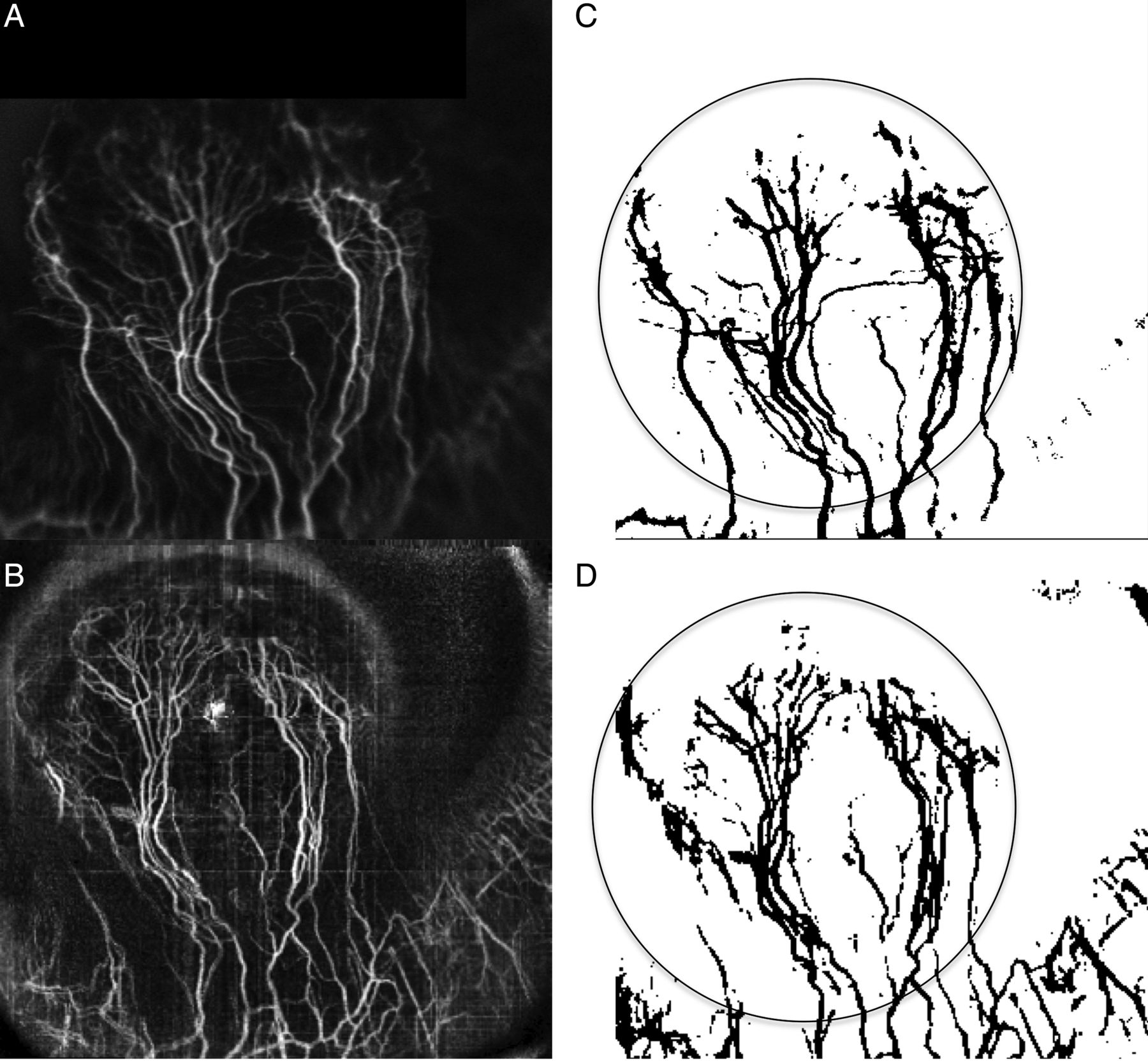
All OCTA and ICGA images were exported from the system as a portable network graphics image file into the National Institutes of Health Image J 1.38X (National Institutes of Health, Bethesda, Maryland, USA) software for analysis using a previously described method (figure 1).14 Briefly, the ‘adjust threshold’ function set to ‘default, HSB’ was first applied to reduce the surrounding noise and highlight the blood vessels by a single analyst masked to the diagnosis and slit-lamp photographs.18 The region of interest (ROI) was encircled (radius 2.50 mm, threshold 0.05) using the in-built ‘Angioflow’ software, which identified the appropriate corneal vessels and the limbus estimated from the marginal corneal vascular arcade in the corresponding area of the corneal vascularisation of all OCTA images.19 Next, we used a selective filter to produce the vessels as a binary image, with pixel resolution (mm/pixel) for ICGA images defined as the ratio between the diameter of the cornea (mm) and the image diameter of the cornea in pixels; and diameter:pixel resolution was determined from the 2.50 mm circle on OCTA scans.20 The resulting binary image was used to calculate the area of corneal vessels within the ROI in mm2 (‘1’ for black pixels over the vessels, ‘0’ for the white background). We assessed the image quality score using a recognised system, that is, 0–4 (0, no vessel discernible; 1, poor vessel delineation; 2, good vessel delineation; 3, very good vessel delineation; 4, excellent vessel delineation), performed by two independent masked assessors.16 We also documented the signal strength of all OCTA scans as determined by the AngioVue system (Optovue Inc.).

Examples of image analysis comparing indocyanine green angiography (ICGA) frames and optical coherence tomography angiography (OCTA) scans. (A and B) The area of corneal vascularisation in the cornea was first identified from ICGA frame and OCTA scan. (C and D) Examples of one ICGA frame and OCTA scan image, which were exported from the system as a portable network graphics image file into the ImageJ software (V.1.49p, Wayne Rasband; National Institutes of Health, Bethesda, Maryland, USA). The ‘adjust threshold’ function in ImageJ was used to highlight the blood vessels and reduce the surrounding noise. The area within the region of interest of 2.5 mm radius was calculated from the binary image and the total area of vessels was calculated, for example, in these images the ICGA frame (0.64 mm2) was compared with the OCTA scan image (0.69 mm2).
Statistical analysis
We analysed all scan images obtained for repeatability, image quality and vessel area measurements between angiography techniques. The area of corneal vascularisation measured from ICGA and OCTA images was assessed using the method described by Bland and Altman, that is, 95% limits of agreement (LOA) and mean difference ±1.96 SD with its 95% CIs calculated with the derived p value.21 We calculated the kappa coefficient (κ) value for the repeatability of scans using the image quality score, where κ≤0.2 was considered slight, 0.21–0.40 weak, 0.41–0.6 moderate, 0.61–0.8 substantial and 0.81–1.0 was considered ‘almost perfect’ in agreement.22 A p value <0.05 was considered statistically significant for comparisons between two quadrants. Statistical Package for the Social Sciences V.17.0 (SPSS Inc., Chicago, Illinois, USA) was used to analyse the data.
Results
In this study, we analysed a total of 64 scans, that is, four OCTA images and four ICGA frames in each of the eight eyes that were included. The mean age of our subjects was 45±0.5 years and five (62.5%) were men. All eyes had significant corneal vascularisation extending more than 3 mm from the limbus into the paracentral cornea with a mean duration of 17±3 months and median visual acuity of 20/50 (20/30–20/80). All scans were performed with substantial repeatability in terms of image quality score (κ=0.80) with a mean image ICGA score of 2.7±0.5, and mean image OCTA score of 2.5±0.6 with mean signal strength of 38±14. The overall mean area of vascularisation from the OCTA scans was 0.51±0.36 mm2 and ICGA scans was 0.49±0.34 mm2. There was no statistically significant difference in the mean measurements from eight eyes comparing both techniques (p=0.674; mean difference of −0.01 mm2, 95% CI −0.11 to 0.08). Overall, the analysis of 64 scans revealed a consistent mean difference of −0.03 mm2 (95% CI −0.07 to 0.01) where the ICGA measured a smaller area compared with the OCTA. We found a good agreement between the two techniques (p=0.127) as the LOA ranged from a lower limit of −0.27 mm2 (95% CI −0.34 to −0.19 mm2) to an upper limit of 0.20 mm2 (95% CI 0.13 to 0.28 mm2) (figure 2).

Bland–Altman plot comparing indocyanine green angiography (ICGA) frames and optical coherence tomography angiography (OCTA) scans. The measured area of corneal vessels within the region of interest from the ICGA and OCTA scans (32 images each) performed in each eye was compared using the Bland–Altman plot. We found a good agreement between OCTA and ICGA scans, although ICGA underestimated the area with a mean difference of −0.03 mm2 (95% CI −0.07 to 0.01).
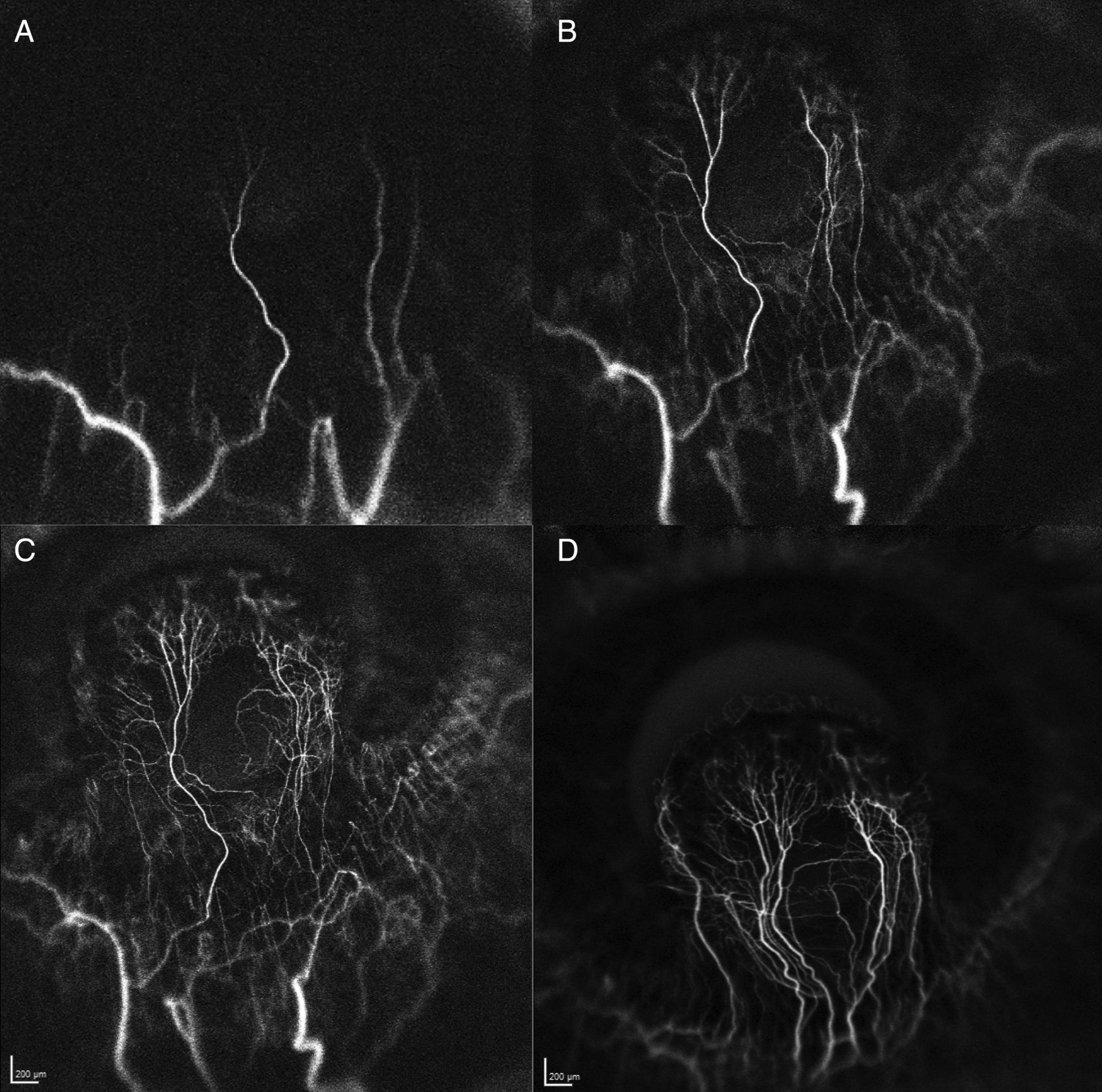
In order to highlight the differences in images obtained from each angiography technique, we present an example of an eye with herpetic keratitis and secondary lipid keratopathy, whose OCTA and ICGA images are also shown in figure 1. As his corneal scarring and vascularisation did not respond to a 6-month course of topical steroid treatment, angiography was performed to delineate the corneal vessels in preparation for fine-needle diathermy. The early ICGA scans (figure 3A,B) demonstrated the afferent vessels within the first 15–30 s, while the later scans demonstrated the remaining efferent vessels at 45 s (figure 3C). There was no leakage detected in the late frames such as that seen at 3 min (figure 3D). Figure 4 demonstrates the use of OCTA images in the same eye, which allows the depth of the corneal vessels to be assessed.

Examples of indocyanine green angiography (ICGA) frames from Case 1 (figure 1). (A) 15 s. (B) 30 s. (C) 1 min. (D) 3 min. Early ICGA frames identified the afferent vessels within the first 15 s (A), extending into the cornea scar (B). The efferent vessels and capillary loops within the corneal scar become evident at 30–45 s (C). Of note, no leakage was detected in the late frames up to 3 min (D).

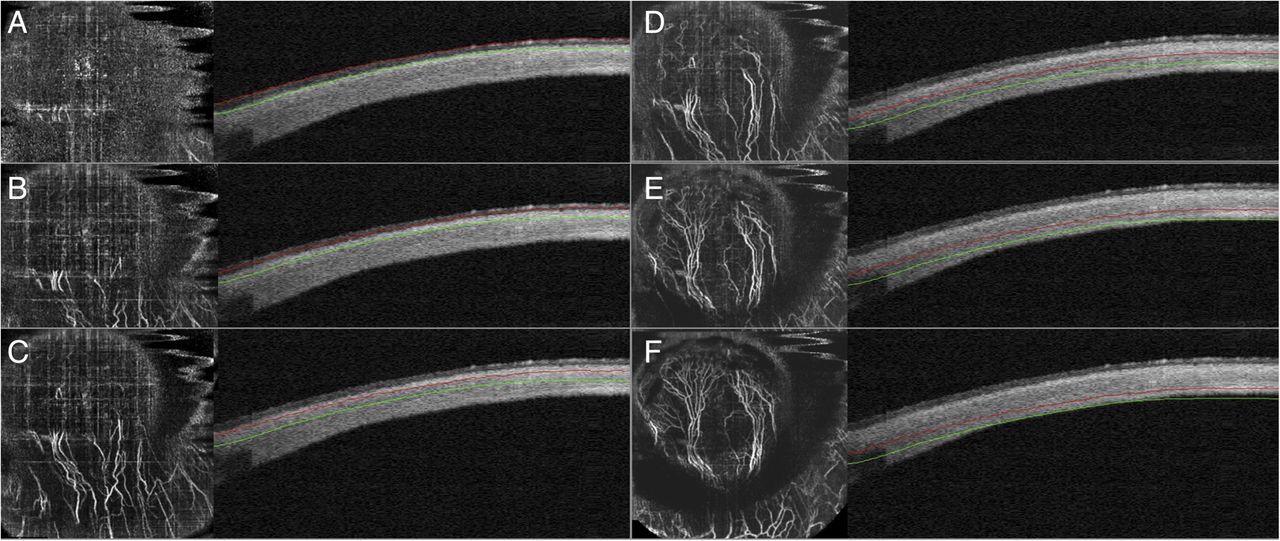
Serial optical coherence tomography angiography (OCTA) scans from Case 1 (figure 1). Cross-sectional OCTA scans of the corneal scar and vessels at varying corneal and scleral depths. ‘Depth-sectioning’ allows for simultaneous assessment of the structure, depth of corneal stromal invasion and the abnormal blood vessels in this lesion. Estimated depth—(A) 0–50 μm; (B) 100–150 μm; (C) 200–250 μm; (D) 300–350 μm; (E) 400–450 μm; (F) 500–550 μm. Scans on the left of each frame (A–F) demonstrate the coronal or ‘en face’ view at varying depths, while the scans on the right of each frame show the traditional cross-sectional view of the cornea, which provides the depth of scan obtained within the cornea scar. Note that the segmentation lines (red and green) are not perfectly parallel with the corneal curvature, leading to several vessels being visible in overlapping cross-sectional segmental scans.
Our study also allowed us to examine some limitations of this relatively new OCTA system, originally designed for the retina. An important observation to highlight is that while the OCTA was able to image most of the vessels in the areas of corneal vascularisation, on closer examination, vessels with segments or branches with a predominant flow in the axial direction may not be delineated as well. We illustrate this characteristic using the eye with herpetic keratitis with a relatively large area of lipid deposition and corneal scarring (figure 5A,B). A single late-frame ICGA image (figure 5C) provides a 2D transverse view of the abnormal corneal vessels with no information on the depth or axial direction of each branch. A ‘close-up’ 3×3 mm OCTA scan of the same region (figure 5D) still suffers from motion artefacts, limited image resolution and a ‘gap’ in the main branch of afferent vessel as the ‘missing’ segment actually loops in the axial direction (anterior to posterior towards the viewer) before continuing down in a transverse direction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figures to demonstrate a closer examination of slit-lamp images, indocyanine green angiography (ICGA) frames and optical coherence tomography angiography (OCTA) scans in another example of corneal vascularisation. In this example of an eye with lipid keratopathy and corneal vessels (A), a higher-magnification of the slit-lamp image reveals the abnormal vasculature (B). The late ICGA frame taken at 3 min confirms the branching patterns of the pathological vessels in a 2D view without stereoscopic appreciation of the depth or direction of vessels (C). Multiple 3×3 mm OCTA scans of good signal strength were taken of the same area and consistently showed a gap in the main vessel (D) as the segment loops from a transverse to axial direction, before extending further down. As this segment of the afferent vessel was superficial, the discontinuity of the vessel shown on OCTA is unlikely to be secondary to minimal flow or blocked signal from the overlying lipid deposition, but may be due to the OCTA being less sensitive to axial flow.
Discussion
Our preliminary study using a relatively new OCTA imaging technique suggests that the measurements of corneal vascularisation are generally of good agreement with ICGA images, with at least 95% of measurements and differences within the 95% prediction intervals and 95% LOA, respectively. However, improvements to image processing and optimisation of the OCTA for the anterior segment may be required in the future developments of OCTA systems. The observed underestimation of corneal vessel area measured by the ICGA compared with OCTA in our study is probably of minimal clinical relevance—but should be taken into consideration and reconfirmed in future studies planning to use these imaging modalities in evaluating new treatments for corneal vascularisation. The small (0.03 mm2), albeit consistent, difference we observed, that is, ICGA underestimating the area of vascularisation, may be due to fundamental differences in the imaging techniques or minor disparities that have arisen from the image analysis—such as non-parallel segmentation or projection artefacts, which may cause a superficial vessel to appear thicker than they should be.12 Our study also suggests that while the SSADA used in this study reduced noise from the images without compromising the flow signal, in the cornea this OCTA system may suffer from image artefacts from light scatter due to corneal scars, which may overestimate the area of vascularisation or lose detection of segments in the vessel with minimal flow or axial flow—as the algorithm used is optimised for the retina and choroid, where vessels exhibit mainly transverse flow.12 However, the aim of this early clinical study was not to determine whether either imaging technique was superior or why these observed differences exist—but instead, to demonstrate the usefulness of this fairly unproven OCTA retinal imaging system adapted for the cornea, and how the measurements compare with the more widely accepted ICGA technique in our current clinical practice.
This study also reinforced several advantages, as well as the current limitations of OCTA adapted for the anterior segment and cornea, compared with an established angiography technique such as ICGA. The first and most obvious advantage of the OCTA is its ability to perform non-contact, cross-sectional and coronal sections of areas of interest in the cornea and associated vessels within seconds.14 However, the field of view and image resolution are currently limited, with several image artefacts, which may be due to the presence of scarring, and the coronal reconstruction of OCT scans, as demonstrated in figures 4 and 5. While clinicians may make up for this by performing multiple scans and ensuring an acceptable signal strength (as determined by the in-built ‘Angioflow’ system in this study), improvements to the software and optimisation for the anterior segment may further improve the field of view and image resolution—before which a clinician may choose to perform ICGA in eyes with concomitant dense corneal scarring.
Second, the OCTA is able to provide high-resolution scans of the cornea with accompanying information on the depth of abnormal vasculature—useful for evaluating corneal scars and any associated vessels while planning for procedures such as lamellar keratoplasty and fine-needle diathermy,3 or evaluation of peripheral corneal infiltrates or melts with the adjacent inflamed sclera and limbal vessels.14 However, unlike the FA or ICGA, the OCTA is unable to demonstrate the sequence of flow, that is, the afferent versus efferent vessels, and is unable to demonstrate any vessel leakage or presence of lymphatics. Leakage of fluorescein occurs rapidly during anterior segment FA through normal vessels, which may actually obscure the true extent of corneal vascularisation.16 While the presence of fluorescein or ICG leakage influences clinical management for retinal or choroidal pathology, in the anterior segment leakage that suggests inflammation may add limited clinical information in the presence of already inflamed sclera.4 On the other hand, the absence of limbal vessels may be a more useful clinical sign of severity in corneal melting disorders and peripheral ulcerative keratitis—a sign that is often obscured by the leakage or extravasation of dye.2 The progression of corneal melting and the need for systemic immunosuppression in such severe inflammatory conditions are usually preceded by vasculitis and vaso-occlusion of the limbal vessels, while recanalisation and new capillary formation may indicate response to treatment.2 Thus, OCTA has the potential to play an important role in detecting progression, prognostication and management of these corneoscleral destructive diseases, which requires further studies in these specific conditions to confirm.
Lastly, our study revealed that performing the OCTA, by trained technicians as well as clinicians, had a relatively easy learning curve. As this is a non-invasive procedure that requires minutes to perform multiple scans (3–4 s per scan) with substantial consistency, patients are not exposed to the potential adverse reactions associated with the administration of intravenous dyes. Significant time and preparation are required before each ICGA or FA imaging session, while some patients may not be suitable for this procedure at all, due to various contraindications.23 ,24 However, it must be emphasised that current OCTA systems are not optimised for the anterior segment, and adjustments had to be made to the scanning technique while using the lens adapter.
The potential clinical applications of OCTA for the anterior segment, apart from those already mentioned, could also extend to addition to intra-operative OCT assessment,25 assessment of graft vascularisation with prognostication for graft rejection,26 evaluation of new antiangiogenic treatments for corneal vascularisation,27 studying limbal vasculature associated with limbal stem cell deficiency28 or even evaluation of bleb vascularity and morphology after glaucoma surgery.29 We recognise the limitations of this preliminary study, which describes the adaptation of the retinal OCTA compared with ICGA for the evaluation of corneal vascularisation. Ideally, a large prospective study of various pathological corneal vessels with comparisons with slit-lamp photography and angiography should be performed to evaluate this OCTA technology specifically for the anterior segment. It would also be useful to perform serial OCTA scans on the same eyes to monitor progression or treatment outcomes. Nonetheless, we present observations from an early clinical study that objectively discusses the advantages and limitations of this novel OCTA system, which may develop further to fulfil its potential as a non-invasive alternative to current angiography techniques. In its current iteration, our findings suggest the OCTA system used in this study may be useful for monitoring areas of corneal vascularisation, but less effective for identifying afferent vessels to guide targeted therapy. Further research using OCTA systems optimised for the anterior segment in various other corneal vascular pathologies would be required to support the observations from this study.
References
Footnotes
Twitter Follow Mark Wilkins at @wilkoman
Funding PAK, DAS, CAE, AT, DFL and MRW have received a proportion of their funding from the Department of Health's National Institute for Health Research (NIHR) Biomedical Research Centre for Ophthalmology at Moorfields Eye Hospital and UCL Institute of Ophthalmology.
Competing interests AT is a member of the Optovue Inc. users group that received non-financial, technical support.
Patient consent Obtained.
Ethics approval Moorfields Eye Hospital NHS Trust and local institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Any additional unpublished data may be obtained from the corresponding author.
Linked Articles
- At a glance