Article Text

Abstract
Purpose To determine if final visual acuity (VA) is affected by duration of macular detachment (DMD) within the first week of macula-off retinal detachment (RD).
Methods This is a retrospective study of eyes that underwent repair within 7 days with vitrectomy or vitrectomy with scleral buckle for macula-off RD at Stanford University Hospital between 1 May 2007 and 1 May 2017. A generalised linear model was constructed using DMD, postoperative lens status, preoperative VA, patient age and surgeon as the independent variables and the final VA as the dependent variable. The main outcome measure was the final VA.
Results Seventy-nine eyes met the entry criteria. Group 1 included 52 eyes with RD repaired within 3 days of DMD, and group 2 included 27 eyes repaired between 4 and 7 days of DMD. The average final VA in group 1 eyes was logarithm of the minimum angle of resolution (logMAR) 0.21 (Snellen 20/33) and in group 2 eyes was logMAR 0.54 (Snellen 20/69). In group 1 and group 2 eyes, preoperative VA (p=0.017and p=0.007), DMD (p=0.004 and p=0.041) and final lens status (p<0.0001 and p<0.001) predicted postoperative VA. Post-hoc analysis showed significant differences in final VA between detachments of 1day vs 3 days (p=0.0009).
Conclusion DMD affects the final VA even among patients whose DMD is <3 days. Based on these results, interventions that shorten DMD, including those occurring within the first 3days, may result in improved long-term VA outcomes.
- retina
- treatment surgery
Statistics from Altmetric.com
Introduction
Advances in surgical techniques have achieved high anatomical success rates for primary retinal detachments (RDs).1 Despite anatomical successes, macula-off RDs continue to have a variable visual prognosis. A number of factors have been identified as predictive of poor visual outcomes, including presenting visual acuity (VA), height of the detachment and duration of macular detachment (DMD).2 3 For the retinal surgeon, timing of the surgical repair is the only factor that has reliably been shown to affect visual outcomes.
Initial studies on surgical timing for macula-off detachments demonstrated that outcomes were improved when surgery was performed within 7 days of macular detachment4; however, a meta-analysis showed that delay of more than 3 days was associated with statistically decreased final VA.5 One shortcoming of these studies is the large variation in final VA outcomes, which may mask the benefit of earlier intervention.
We hypothesise that even within the first 3 days, DMD has an effect on final VA. This hypothesis is based on animal experiments demonstrating photoreceptor damage begins on the first day of detachment and progressively increases as long as the retina remains detached.6–11
The purpose of this study was to evaluate VA outcomes after surgery for macula-off RD based on DMD at the time of repair.
Materials and methods
A review was performed of all eyes that underwent repair for macula-off RD at Stanford University Hospital between 1 May 2007 and 1 May 2017.
Eyes were included in the analysis if they had a macula-off RD with DMD of 7 days or less. Eyes were only included if the fovea was documented as detached. Eyes were excluded from analysis if the total DMD could not be determined, there was other visually significant pathology other than cataract, baseline proliferative vitreoretinopathy was present, or if they had a history of RD. Eyes were also excluded if RD was repaired with primary pneumatic retinopexy or primary scleral buckling procedure, if they underwent repeat surgical intervention after the initial repair, or if follow-up after the RD repair was less than 2 months.
Baseline patient characteristics including age, gender, phakic status and VA were recorded. VA was measured as the recorded best-corrected Snellen VA on the patient chart. DMD at the time of presentation determined by patient-reported timing of onset of loss of central vision was recorded. Time to repair of the RD after presentation, surgical technique and type of tamponade agent as specified in the operative report, final VA, lens status, and duration of follow-up after RD repair were recorded.
Analysis
All VAs were converted to logarithm of the minimum angle of resolution (logMAR) for statistical analysis. Using JMP V.13 (SAS Institute, Cary, North Carolina), a generalised linear model was constructed using DMD, postoperative lens status, preoperative VA, age of patient and surgeon as the independent variables and the final VA as the dependent variable. The model assumed a normal distribution with a maximum likelihood estimation method. Because a meta-analysis by van Bussel et al 5 showed a benefit of operating within 3 days, the patients were separated into two subgroups, a priori. Group 1 included only those patients in whom the detachment duration was ≤3 days, and group 2 included only those patients in whom the total detachment duration was 4–7 days. These groups were similarly analysed with the above generalised linear model. This allowed us to determine whether the total DMD affected even those patients in whom surgery was performed within 3 days. Finally, a post-hoc analysis was performed by a pairwise comparison of the effect of RD duration on final VA between patients with a duration of 1, 2 or 3 days.
Results
Baseline characteristics
Seventy-nine eyes of seventy-nine patients met the entry criteria and were included in the statistical analysis. Group 1 consisted of 52 of the 79 eyes that had a DMD of ≤3 days. The mean VA of group 1 at presentation was logMAR 1.39+0.98 (Snellen 20/490; range: 20/25, hand motions), and the average DMD at presentation was 2.0+0.9 days. Group 2 consisted of 27 of the 79 eyes with a DMD of 4–7 days. The mean VA of group 2 at presentation was logMAR 1.76+1.02 (Snellen 20/1150, range: 20/25, hand motions), and the average DMD at presentation was 4.0+1.5 days (table 1).
Baseline patient characteristics
Surgical procedure
Of the seventy-nine eyes, 58 (73%) underwent a combination scleral buckle-vitrectomy and 21 (27%) underwent primary vitrectomy. The choice of tamponade agent varied: C3F8 in 60 cases (76%), SF6 in 13 cases (16%), silicone oil in 5 cases (6%) and air in 1 case (1%). In group 1 eyes, C3F8 was used in 79% of cases, SF6 in 14% of cases, silicone oil in 6% of cases and air in 2% of cases. In group 2 eyes, C3F8 was used in 70% of cases, SF6 in 22% of cases and silicone oil in 7% of cases.
The average time to surgery from diagnosis was 0.8+1.0 days, with an average total DMD of 3.1+1.8 days. In group 1, the average time to surgery from diagnosis was 0.5+0.8 days, with an average total DMD of 2.0+0.8 days. In group 2, the average time to surgery from diagnosis was 1.4+1.2 days, with an average total DMD of 5.3+1.0 days. Operative repair was performed by one of seven surgeons.
VA outcomes
The average follow-up was 19.6 months (range: 2–105 months). The average final VA of all patients was logMAR 0.32+0.42 (Snellen 20/41). The average final VA in group 1 eyes was logMAR 0.21 (Snellen 20/33) and in group 2 eyes was logMAR 0.54 (Snellen 20/69). At final follow-up, 63 eyes (80%) were pseudophakic and 16 eyes (20%) were phakic.
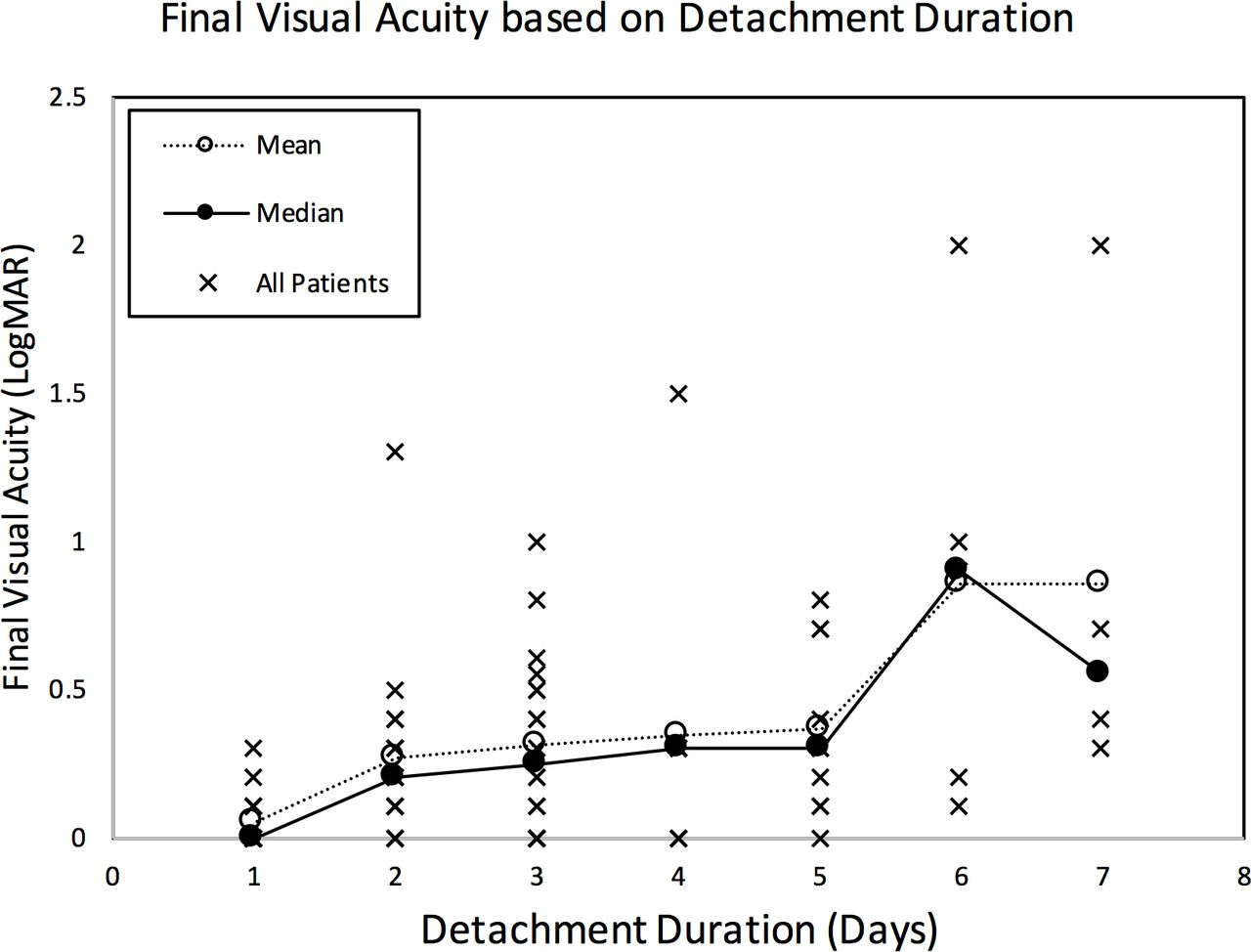
Among all eyes, preoperative VA (p=0.0001), total DMD (p=0.0002) and lens status (p<0.0001) all were associated with postoperative VA. Age (p=0.14) and surgeon (p=0.65) did not correlate with postoperative VA. Figure 1 shows the final VA as a function of preoperative VA. On average, approximately one line of vision (logMAR 0.1) was lost for each additional day of total detachment duration.
{kind=link}
Final visual acuity as a function of duration of macular detachment in days. LogMAR, logarithm of the minimum angle of resolution.
Among eyes with a total detachment duration of ≤3 days (group 1), preoperative VA (p=0.017), total DMD (p=0.004) and lens status (p<0.0001) were associated with postoperative VA. Age (p=0.56) and surgeon (p=0.56) did not correlate with postoperative VA.
Among eyes with total DMD of 4–7 days (group 2), preoperative VA (p=0.007), total DMD (p=0.041) and lens status (p<0.0001) were associated with postoperative VA. Age (p=0.16) and surgeon (p=0.36) did not correlate with postoperative VA.
Post-hoc analysis showed that the total DMD predicted final VA between patients with 1-day (n=17) detachment duration vs 3-day detachment duration (n=18) (p=0.0009), but the total detachment duration did not predict final VA between patients with a 2-day detachment duration (n=17) vs a 3-day detachment duration (p=0.058).
Discussion
The photoreceptors have enormous metabolic needs that are met only by their close apposition to the retinal pigment epithelium (RPE) and the choroidal circulation. During RD, the outer retina is separated from the RPE and choroid leading to major metabolic derangements at least in part due to hypoxia.6 7 In experimental models of RD, these metabolic derangements result in photoreceptor apoptosis, particularly among cones, that begins during the first day and peaks by day 3.8–11 Within just a week after the detachment, the outer segment layer is reduced to approximately 10% of its normal width with complete loss of cone-specific cellular markers.12
Given the progressive photoreceptor damage that occurs in animals during the first week of a RD, it is surprising that clinical studies have not demonstrated a strong relationship between detachment duration and VA outcomes for detachments of up to 5–7 days in duration. In 1982, Burton4 reported on a series of patients who had undergone scleral bucking for repair of RD, and showed better VA outcomes resulted when surgery was performed within the first 5 days. In 1998, Ross and Kozy published a prospective study of patients undergoing scleral buckling for macula-off RD and concluded that delay of repair for up to 7 days does not negatively affect visual outcome.13 Subsequently, several other groups have reported similar findings that delays in repair of macula-off RD with scleral buckle up to 6–10 days provided similar VA outcomes.14–16 However, in 2009, Henrich et al published results with scleral buckling in macula-off detachments and suggested a much shorter interval of 3 days should be used for the optimal timing of repair.17 One reason why it may be hard to find a difference in the first 5–7 days with scleral buckling alone is because at the end of a scleral buckle, the macula is rarely attached, even with drainage. This adds a source of variability if the DMD is the primary driver of eventual vision outcomes. For this reason, we excluded patients from our study who underwent scleral buckling alone.
In 2013, Kim et al reported optimal results of vitrectomy for macula-off RD occur within the first 6 days, and a similar study by Kikushima et al in vitrectomy patients suggested repair within the first 10 days.18 19 Interestingly, in Kikushima et al’s study, the number of patients who achieved 20/40 or better vision after 2 days significantly decreased, although no significant decrease in visual prognosis was found with delay of surgery up to 10 days.18
One universal finding among these studies is the large variation in final VA that is observed after repair of macula-off detachments, which cannot be solely attributed to preoperative characteristics, surgical timing or the choice of surgery. This large variation in final VA may in part be explained by histopathological findings of non-uniform photoreceptor damage that occurs after RD.12 20 When focal areas of damage occur subfoveally, VA can be severely compromised, but if the subfoveal region is spared, VA can be preserved.21–23 Such variation may make it difficult to identify clear effects of detachment duration on final visual outcomes without large numbers of patients undergoing similar types of interventions. Overbinning patients during statistical analysis can further mask clinically significant effects by reducing the number of patients in each group.
Our study sought to directly address the issues encountered in these other studies. We restricted our inclusion criteria to only include patients who underwent primary vitrectomy or combined vitrectomy scleral buckle in which subretinal fluid was drained leaving the macula effectively attached at the end of the case. To determine appropriate bin size, we used the meta-analysis performed by van Bussel et al,5which we consider the most extensive analysis of timing of repair for macula-off RD. In this study, macula-off detachments of 3 days or less in duration had better VA outcomes than detachments of 4–7 days in duration. To date, there have been no studies that have found that surgical intervention within the first 3 days of a macula-off detachment affects final VA. To avoid overbinning, while still addressing the question of whether surgical timing is important during the first 3 days, we a priori separated eyes into two groups, those that were repaired within 3 days and those that were repaired within 4–7 days. The expected result based on existing literature of this binning strategy was that DMD would not affect VA outcomes in either the group of 3 days or less or the group of 4–7 days.
We found that even for detachments repaired within 3 days, the DMD was correlated with the final VA, independent of preoperative VA, lens status, age and surgeon. Consistent with previous reports, we also found that better preoperative VA and pseudophakia at final follow-up were associated with better final VA.
There are several potential confounding factors that may have affected our results. First, our study was retrospective and we did not have information on the height of RD at the time of presentation. This is a major weakness since detachment height has been linked to final VA outcomes, independent of detachment duration.3 It is possible that the distribution of detachment heights across patients having detachments of 3 days or less was asymmetric and may have compromised our findings.
A second factor that could have affected our results is the accuracy of dating DMD. We used the patient’s reported loss of central vision as a marker for foveal detachment; however, non-retinal causes of central acuity reduction, such as a Weiss ring or vitreous haemorrhage may have caused the decrease in VA. While none of the patients in our study had vitreous haemorrhages obscuring the macula, significant floaters may not have been documented and the distinction between visual loss from vitreous debris versus macular involvement may not have been properly assessed. We also cannot rule out the possibility that some patients had detachments for durations longer than their perceived reductions in central acuity. Of note, accurate dating of macular detachment is a limitation faced by all prior studies on surgical timing of macula-off detachments.4 5
Finally, due to the retrospective nature of the study, there was a wide range in the follow-up duration. Although follow-up was added to our generalised linear model and showed no statistically relationship with VA outcomes, longer follow-up for some patients would have been preferred given the slow recovery that can be observed after RD.
Despite these weaknesses, our study does indicate that shorter DMD is associated with better final VA even among patients whose detachment is ≤3 days. These findings are consistent with our current understanding of progressive photoreceptor damage that begins within 24 hours of RD and can be halted with retinal reattachment.8 Based on these results, interventions that shorten the duration of the macula-off RD, including those occurring within the first 3 days, may result in improved long-term VA outcomes.
References
Footnotes
Contributors Design of the study: MAG, IHS. Conduct of the study: MAG, TL, RAS, L-SBL, PAK, DMM, SRS, IHS. Collection of data: MAG. Management, analysis and interpretation of data: MAG, TL, RAS, L-SBL, PAK, DMM, SRS, IHS. Preparation of manuscript: MAG, TL, RAS, L-SBL, PAK, DMM, SRS, IHS. Review and approval of manuscript: MAG, TL, RAS, L-SBL, PAK, DMM, SRS, IHS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MAG: consultant: Alimera Sciences. TL: consultant: Carl Zeiss Meditec, 23andMe; research grants: Genentech, Allergan, Ohr. RAS: no financial disclosures. L-SBL: consultant: Google. PAK: consultant: Google. DMM: consultant: Alcon, Iconic Therapeutics, Krypton Vision, Visunex; SAB: Allergan; Equity, dSentz, Grand Legend Technologies, PromiSight, Versl, Visunex; Founder/Director: dSentz, PromiSight, Versl. SRS: no financial disclosures. IHS: no financial disclosures.
Patient consent for publication Not required.
Ethics approval The Stanford University Hospital and Clinics IRB approved the study. Data collection and reporting were in compliance with all Health Insurance Portability and Accountability Act regulations.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance