Article Text

Abstract
Background Retinopathy of prematurity (ROP) is a severe complication of preterm birth and can lead to severe visual impairment or even blindness if untreated. The incidence of ROP requiring treatment is increasing in some developed countries in conjunction with higher survival rates at the lower end of gestational age (GA).
Material and methods The incidence of ROP and severe ROP (sROP) requiring treatment in Switzerland was analysed using the SwissNeoNet registry. We conducted a retrospective cohort analysis of very preterm infants with a GA below 32 weeks who were born between 2006 and 2015 in Switzerland. Patient characteristics were stratified according to GA.
Results 9.3% and 1.8% of very preterm infants in Switzerland developed ROP of any stage and sROP, respectively. The incidence of ROP treatment was 1.2%. Patients with 24 and 25 weeks GA had the highest proportion of ROP treatment at 14.5% and 7.3%, respectively, whereas the proportion of treated infants at or above a GA of 29 weeks was 0.06%. Similarly, the risk of sROP declined strongly with increasing GA. During the observation period of 10 years, the incidence of ROP treatment ranged between 0.8% and 2.0%. Incidences of sROP or ROP treatment did not increase over time.
Conclusion The incidence of ROP treatment in Switzerland is low and was stable over the analysed period. The low incidence of sROP in patients with a GA of 29 weeks or more leaves room for a redefinition of ROP screening criteria.
- neonatology
- ophthalmology
- epidemiology
Statistics from Altmetric.com
What is already known on this topic?
Retinopathy of prematurity (ROP) is a severe complication of preterm birth and can lead to visual impairment or even blindness.
The risk of developing ROP increases with decreasing gestational age or birth weight.
The incidence of ROP differs between countries, but high quality data of ROP treatment in preterm infants are scarce.
What this study adds?
The risk of preterm infants below 32 weeks gestational age (GA) in Switzerland to develop retinopathy of prematurity (ROP) ≥ stage I, severe ROP and ROP requiring treatment was 9.3%, 1.8% and 1.2%, respectively.
ROP treatment was extremely low (0.06%) in preterm infants between 29 0/7 and 32 weeks GA.
The extremely low risk of requiring ROP treatment in patients ≥ 29 0/7 weeks GA might allow to optimize Swiss ROP screening criteria
Introduction
Retinopathy of prematurity (ROP) is a two-stage developmental vascular proliferative disorder resulting from a mismatch between oxygen demand and oxygen supply within the retina.1 2 During the first stage, relative hyperoxia causes reduced growth of blood vessels within the retina. In the second stage, relative hypoxia leads to accelerated and irregular growth of vessels causing abnormal fibrovascular tissue which tends to contract and may ultimately result in retinal distortion or even retinal detachment.1–3
ROP was first described by Terry in 1942.4 Since then, the incidence of ROP in preterm infants peaked several times which has been frequently described as three epidemics of ROP. The first epidemic occurred in the 1940s and 1950s predominantly in the USA and to a lesser extent in Europe. It was caused by a liberal use of oxygen in preterm infants. Higher survival rates of preterm infants in the 1970s in developed countries led to the second epidemic. Around 2000, a third epidemic was described in developing countries, which was probably caused by decreasing infant mortality rates, higher rates of preterm birth in these countries and limited resources for titration and continuous oxygen monitoring.
In developed countries, the incidence of ROP seemed to be declining in the surfactant era. However, studies that are more recent show that the incidence of ROP requiring therapy might be increasing in Europe.5 6
The aim of this study was to assess the incidence of ROP in Switzerland in very low birthweight infants who were born between 2006 and 2015.
Material and methods
Study population
We conducted a retrospective cohort analysis of preterm infants that were born between 2006 and 2015 and were registered at the national registry of very preterm infants in Switzerland (SwissNeoNet, SNN). The network prospectively collects a routine data set of perinatal and follow-up data of live born infants with a gestational age (GA) between 22 0/7 weeks and less than 32 0/7 weeks from birth to primary discharge home. In addition, the network collects routine follow-up data at 18 to 24 months corrected. This study focused on data from the perinatal dataset plus the information of any ROP treatment after primary discharge home from the 18 to 24 months follow-up assessment. All nine Swiss perinatal centres and most step-down units participated. Routine comparison with the Swiss Federal Statistical Office reveals population coverage compared with the Swiss vital statistics.
Definitions
ROP was assessed by funduscopy by the local ophthalmologists in all Swiss perinatal centres. Screening criteria for ROP differed slightly between the individual centres but mostly included preterm infants born before 31–32 weeks of gestation and/or a birth weight below 1500 g. Stages of ROP were categorised according to the international classification of retinopathy of prematurity.7 Severe ROP (sROP) was defined as ROP stages 3–5 in any retinal zone.
ROP treatment included any form of therapy (cryotherapy, laser coagulation or intravitreal antivascular endothelial growth factor) that was performed according to current recommendations as indicated by the local ophthalmologist. All ROP proportions are in relation to children with available information on ROP that survived at least until discharge home after primary hospitalisation.
In Switzerland, all ROP treatments are performed at one of five ophthalmological units. During the observation period, guidelines for screening and treatment of ROP as well as target values for oxygen saturation in preterm infants did not change on a national level.
Definition of covariates
Patients were classified as small for gestational age when the birth weight was below the 10th percentile based on the growth curves by Voigt et al.8 Supplemental oxygen, continuous positive airway pressure (CPAP) and mechanical ventilation were defined as number of days during hospitalisation with more than 12 hours of respiratory support, respectively. We defined bronchopulmonary dysplasia as an oxygen requirement at 36 weeks GA according to the National Institute of Child Health and Human Development consensus conference paper9 and antenatal steroid use as any administration prior to birth, regardless of the time interval.
Statistical methods
We calculated patient characteristics and outcome measures for all patients as well as stratified by year of birth, GA and birth weight. Missing data were excluded from further analyses. Analyses were performed with R (The R Project for Statistical Computing; https://www.r-project.org/). Cochran-Armitage test for trend was used to analyse trends over time.
Ethics
Data collection and evaluation for this study were approved by the Swiss Federal Commission for Privacy Protection in Medical Research and the Swiss ethical review boards (KEK-ZH-Nr. 2014–0551 and KEK-ZH-Nr. 2014–0552). The patients’ representatives were informed about the use of data for research.
Results
Swiss Society of Neonatology (SSN) registered 7817 patients between 2006 and 2015. Between 2007 to 2015, the Swiss Federal Statistical Office registered 7454 live births, between 22 0/7 and 31 6/7 gestational weeks (including births from non-residential mothers), corresponding to 7127 patients in SSN resulting in 96% population coverage (reference data for 2006 were not available as GA was not included in the national register prior to 2007).
Of the 7817 eligible patients, a complete data set including data on all parameters of interest was available for almost all of the patients. ROP treatment data were missing in 1116 patients, of which we were able to retrospectively complete 942 cases by checking the patient records at the ophthalmology units, leaving 174 patients with unavailable ROP data. Information on ROP treatment was missing for infants mostly in the upper range of GA. This resulted in completeness of ROP data in 97.8% of patients registered in SwissNeoNet and of 97.4% survivors at discharge home. Table 1 gives an overview of baseline characteristics and missing data.
Baseline patient characteristics and missing data of all infants
Five hundred and fifty-five of the 7817 infants died in the delivery room. The majority of these patients was treated with a priori palliative care and did not receive medical resuscitation. Of the remaining 7262 patients, 616 died during hospitalisation, leading to a survival rate of 91.5% for patients who received resuscitation. figure 1 shows numbers of included and excluded patients.
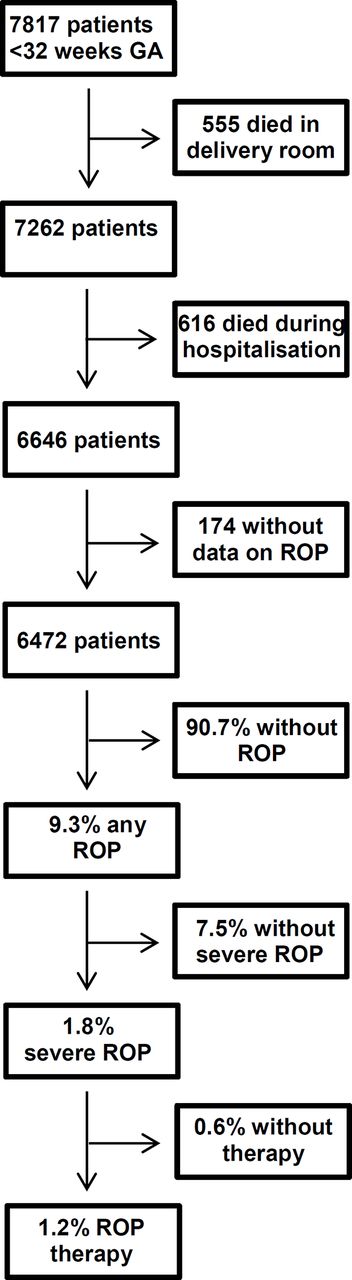
Flow chart of patients and results of the study. GA, gestational age; ROP, retinopathy of prematurity.
The patient numbers increased with increasing GA. More than 40% of patients were born at 30 or 31 weeks of gestation and the minority of patients was born below 27 weeks when the risk of ROP is highest. Around one-third of patients were born in multiple pregnancies. Table 2 summarises frequencies of risk factors and parameters describing neonatal morbidity.
Patient characteristics stratified by gestational age
ROP treatment also increased with lower GA (Cochran-Armitage test p=0.027) and was necessary for patients with a GA as of 24, 25, 26, 27, 28, 29, 30 and 31 weeks in 14.5%, 7.3%, 2.7%, 1.1%, 0.5%, 0.0%, 0.2% and 0.1%, respectively (table 2). The incidence of ROP treatment was 1.2% in all patients together, 2.8% in patients below 28 weeks GA and 0.06% in infants born 29–31 weeks GA. The analysis of treatment depending on GA revealed that 13, 7 and 3 patients with a GA of more than 26, 27 and 28 weeks were treated for ROP in Switzerland during the observation period, respectively. The three patients with highest GA were preterm infants of 30 1/7, 30 5/7 and 31 4/7 weeks GA, respectively with birth weights of 1530 g, 1370 g and 1300 g. figure 2 shows patient distribution according to birth weight and GA.
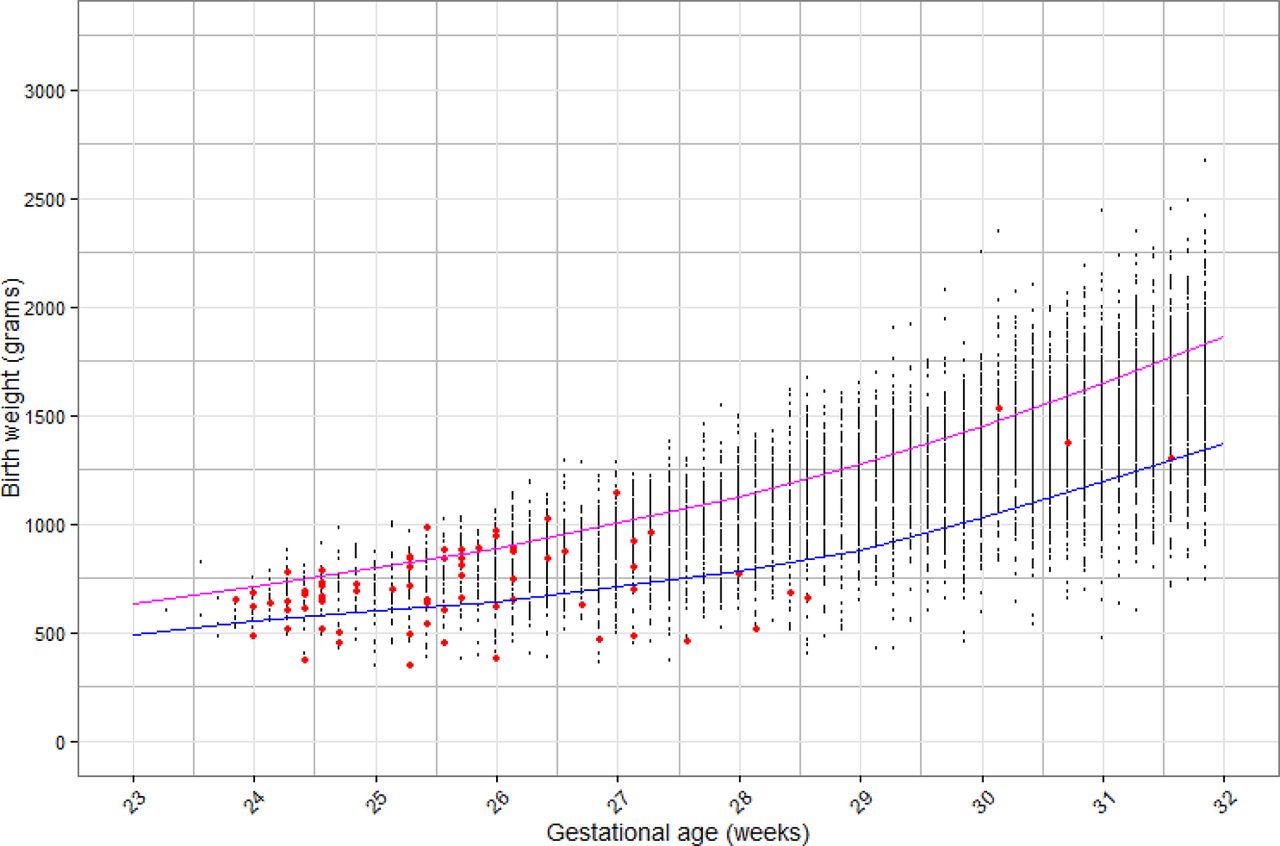
Study cohort plotted by birth weight (grams) and gestational age (weeks). Infants receiving an intervention for retinopathy of prematurity are marked red. The lower blue line denotes the 10th percentile while the upper purple line denotes the 50th percentile of birth weight per gestational age.
During the observation period, the incidence of ROP intervention did not change significantly (table 3; Cochran-Armitage test for trend p=0.503).
Patient characteristics stratified by year
During the observation period, overall mortality rates ranged between 16.7% in 2006 and 12.4% in 2014. Patient mortality tended to decrease over time (figure 3). Mortality rates include patients with a GA of 22 and 23 weeks for which resuscitation was recommended only in special circumstances according to Swiss national guidelines, resulting in a mortality of 100% and 93.3% in these patients, respectively.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier analysis showing survival for each birth year during the observation period.
Discussion
This study assessed the incidence of treated ROP between 2006 and 2015 in Switzerland and trends over time. As detailed below, the Swiss ROP requiring therapy was generally low. Only 1.2% of children born below 32 weeks GA and 0.06% in infants born between 28 and 32 weeks were treated for ROP between 2006 and 2015. During the 10-year observation period, only nine patients with a GA of more than 27 weeks needed treatment for ROP. The incidence of ROP treatment varied between 0.8% and 2.0% of patients born below 32 weeks in Switzerland and did not increase over time even though there was a tendency towards a higher proportion of infants at risk for developing ROP.
In Denmark, the national birth registry provides a database with comparably high data quality including stillbirths. Similar to our collection, data were collected prospectively for the purpose of assessing the prevalence of various outcomes concerning very preterm born children. An analysis of Danish data showed an increase of ROP treatment already from 1998 to the end of the observation period in 2005,10 resulting in 4% ROP treatment in patients below 32 weeks GA who survived for at least 5 weeks.
A large retrospective analysis of ROP incidence in England assessed an observation period of 22 years (1990 to 2011). This study showed that ROP treatment by cryotherapy or laser rose from 0.17% of very preterm infants in 1990 to 1.48% in 2011 with a trend to further increased treatment rates. The authors state that the dramatic rise in the number of babies treated from 2005 was most likely secondary to publication of the Early Treatment for Retinopathy of Prematurity (ETROP) Study in 2003.11 This study showed a significant reduction in visual adverse outcomes with earlier treatment from 19.5% to 14.5%. At 9 months of age, unfavourable structural outcomes were reduced from 15.6% to 9.1%.
Our study did not include the year 2005 when the increase in ROP treatment commenced in the English population. In contrast to this study, results of our study showed relatively stable treatment rates in preterm infants with a birth weight below 1500 g. The highest rate of ROP treatment occurred in 2010 with 2.0%. Lower rates were demonstrated for 2013–2015 and the lowest rate was shown in 2015 (0.8%), confirming that there was no trend to increased numbers of ROP therapies. Furthermore, a publication on trends of mortality and morbidity in Switzerland showed low rates of sROP also in the years 1996, 2000, 2004 and 2008 without increasing incidence over time.12
Other European countries published higher rates of ROP therapy in very preterm infants than we found in Switzerland. For example, the incidence of ROP requiring treatment at certain centres in Germany was 3.2% of all infants screened.13 This study was based on a registry including several centres providing data obtained in routine clinical practice. Centre participation was voluntary and only a subgroup of infants treated for ROP in Germany was represented. Therefore, a selection bias in this German study is more likely than in our population based study. In Sweden, 19.6% of preterm infants with a GA of less than 27 weeks were treated for ROP in the period from 2004 to 2007.14
A direct comparison of these incidences might be limited by the definition of viability and, therefore, the initiation of resuscitation in extremely preterm infants with highest risks for mortality and morbidity. In Switzerland, preterm infants often received comfort care at a GA below 24 weeks.15 This limit is higher than in other countries and may bias the incidence of ROP in these patients with the highest risk.
A recently published comparison of data from 10 neonatal networks including patients from 24 0/7 to 27 6/7 weeks was therefore limited to patients who were above the locally defined limit of viability in some countries.16 This study revealed a wide variation in ROP treatment incidence between neonatal national networks. It also confirmed that the incidence is significantly lower in Switzerland compared with all other networks. Furthermore, it was shown that 79.5% of very low birth weight infants survived to 32 weeks GA in Switzerland. In other neonatal networks, survival rates ranged between 67.8% (Spain) to 91.8% (Japan) with a mean survival rate of 81.8%, making Swiss data comparable to most other countries. These findings are mirrored by a similar study focusing broader on morbidity and mortality in very preterm infants, showing lower incidence in the Swiss population than in other networks.17
Possible explanations of lower incidence of ROP treatment include, as discussed before, the competing risk factors of mortality and ROP. A lower threshold of GA to initiate full therapy despite the presence of risk factors would probably result in higher ROP rates. Furthermore, thresholds to withdraw therapy in the tiniest and sickest infants who have highest risk for ROP might also differ between countries. For example, Japan shows high survival rates at the limit of viability at 22–24 weeks GA18 but higher rates of ROP therapy.16
We expected to find an increasing rate of ROP treatment over time. This assumption was based on the publication of three large trials assessing target oxygen saturations in preterm infants showing that lower oxygen saturation targets are associated with higher mortality, whereas higher oxygen saturation targets increased the ROP incidence.19–21 Since reducing mortality may be considered superior to avoiding ROP, we expected a more liberal use of oxygen targets leading to more patients requiring ROP treatment. However, we did not find these results. In fact, during the last years of the observation period 2013 to 2015, the ROP treatment incidence was below the average and 2015 had even the lowest ROP treatment rate overall. At the same time, as confirmed before, the mortality showed a tendency to decrease from 16.7% in 2006 to 13.1% in 2015, while the decrease in delivery room deaths at the lower end of GA is noteworthy.22
The proportion of patients in our study increased with GA. Patients ≥29 weeks represented more than 50% of the patient population. These patients showed a very low ROP treatment incidence of less than 0.1%. In turn, more than 99% of patients born at 29–32 weeks were screened without requiring therapy, raising the question of whether current Swiss screening criteria could be optimised.
Funduscopy for ROP screening has been shown to be painful,23 24 and reducing pain exposure is a goal in neonatal care, particularly for preterm infants. Furthermore, reducing the workload on the wards and financial expenses may be additional positive effects to thrive for.
This study has some limitations. Similar to other large databases, an uncertainty about data quality remains. However, several studies based on the SNN have been published, demonstrating robust data quality for most variables. Concerning data from the SNN specifically on ROP treatment, we were able to complete missing data retrospectively to a large extent, leaving only 2.6% of patients with missing data. An additional statistical limitation is the relatively low number of patients with treated ROP; only 76 patients were treated during the 10-year observation period.
The strengths of this study are the large number of patients, the long observation period and the geographical coverage of more than 96%, making this report population based. Almost 8000 patients have been included in this retrospective analysis over a 10-year period.
In summary, the results of this study show that the incidence of ROP requiring therapy is low and did not increase over time from 2006 to 2015 in Switzerland. Furthermore, the incidence of treated ROP is lower in Switzerland than in several other European countries. In particular, patients between 29 and 32 weeks of gestation have a very low risk for ROP intervention. This suggests a potential for adapting ROP screening criteria in Switzerland to decrease stress for very preterm infants with low risk.
Acknowledgments
We would like to thank the following units for collaborating in this study of the SNN: Aarau: Cantonal Hospital Aarau, Children’s Clinic, Department of Neonatology (Ph Meyer, C Anderegg), Department of Neuropaediatrics (A Capone Mori, D Kaeppeli); Basel: University Children’s Hospital Basel, Department of Neonatology (S Schulzke), Department of Neuropaediatrics and Developmental Medicine (P Weber); Bellinzona: San Giovanni Hospital, Department of Paediatrics (G P Ramelli); Berne: University Hospital Berne, Department of Neonatology (M Nelle), Department of Paediatrics (B Wagner), Department of Neuropaediatrics (M Steinlin, S Grunt); Biel: Development and Paediatric Neurorehabilitation Centre (R Hassink); Chur: Children’s Hospital Chur, Department of Neonatology (T Riedel), Department of Neuropaediatrics (E Keller, Ch Killer); Fribourg: Cantonal Hospital Fribourg, Department of Neuropediatrics (K Fuhrer); Lausanne: University Hospital (CHUV), Department of Neonatology (J F Tolsa, M Roth-Kleiner), Department of Child Development (M Bickle-Graz); Geneva: Department of Child and Adolescent, University Hospital (HUG), Neonatology Units (R E Pfister), Division of Development and Growth (P S Huppi, C Borradori-Tolsa); Lucerne: Children’s Hospital of Lucerne, Neonatal and Paediatric Intensive Care Unit (M Stocker), Department of Neuropaediatrics (T Schmitt-Mechelke, F Bauder); Lugano: Regional Hospital Lugano, Department of Paediatrics (V Pezzoli); Muensterlingen: Cantonal Hospital Muensterlingen, Department of Paediatrics (B Erkert, A Mueller); Neuchatel: Cantonal Hospital Neuchatel, Department of Paediatrics (M Ecoffey); St. Gallen: Cantonal Hospital St. Gallen, Department of Neonatology (A Malzacher), Children’s Hospital St. Gallen, Neonatal and Paediatric Intensive Care Unit (J P Micallef), Department of Child Development (A Lang-Dullenkopf); Winterthur: Cantonal Hospital Winterthur, Department of Neonatology (L Hegi), Social Paediatrics Centre (M von Rhein); Zurich: University Hospital Zurich (USZ), Department of Neonatology (D Bassler, R Arlettaz), University Children’s Hospital Zurich, Department of Neonatology (V Bernet) and Child Development Centre (B Latal, G Natalucci).
References
Footnotes
Contributors RG was responsible for study design, supervised data collection and analyses. He also wrote the first and subsequent versions of the manuscript. VB was responsible for data collection, validation of existing data and completion of missing data. DB, BL, REP, MN and BM were involved in the design of the study and contributed to data collection at neonatal centres as well as editing of the final manuscript. CG-K was involved in the assessment of ROP stages, gave valuable input in interpretation of ophthalmological data and reviewed the manuscript critically. MA was responsible for data collection and validation of the SwissNeoNet. He also performed statistical analyses, was responsible for interpretation of data quality and edited the final manuscript. All authors revised the results and their interpretation carefully, approved the final version of the manuscript and are accountable for all aspects of the work.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval Swiss Federal Commission for Privacy Protection in Medical Research and the Swiss ethical review boards (KEK-ZH-Nr. 2014-0551 and KEK-ZH-Nr. 2014-0552)
Provenance and peer review Not commissioned; externally peer reviewed.