Article Text

Abstract
Objective The objective of this study was to characterise the incidence rates of herpes zoster (HZ), also known as shingles, and risk of complications across the world.
Design We systematically reviewed studies examining the incidence rates of HZ, temporal trends of HZ, the risk of complications including postherpetic neuralgia (PHN) and HZ-associated hospitalisation and mortality rates in the general population. The literature search was conducted using PubMed, EMBASE and the WHO library up to December 2013.
Results We included 130 studies conducted in 26 countries. The incidence rate of HZ ranged between 3 and 5/1000 person-years in North America, Europe and Asia-Pacific, based on studies using prospective surveillance, electronic medical record data or administrative data with medical record review. A temporal increase in the incidence of HZ was reported in the past several decades across seven countries, often occurring before the introduction of varicella vaccination programmes. The risk of developing PHN varied from 5% to more than 30%, depending on the type of study design, age distribution of study populations and definition. More than 30% of patients with PHN experienced persistent pain for more than 1 year. The risk of recurrence of HZ ranged from 1% to 6%, with long-term follow-up studies showing higher risk (5–6%). Hospitalisation rates ranged from 2 to 25/100 000 person-years, with higher rates among elderly populations.
Conclusions HZ is a significant global health burden that is expected to increase as the population ages. Future research with rigorous methods is important.
- EPIDEMIOLOGY
- VIROLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
We comprehensively reviewed the global burden of herpes zoster.
-
We found a similar age-specific incidence of herpes zoster in North America, Europe and Asia-Pacific; however, there is a scarcity of research from other regions.
-
Because the quality of the study, study design and study population varied widely across studies, we could not synthesise the data quantitatively.
Introduction
Herpes zoster (HZ), also known as shingles, is typically characterised by painful, blistering dermatomal rash.1 ,2 The estimated lifetime risk of HZ in the general population is approximately 30%, with the risk increasing sharply after 50 years of age.3 After conducting a careful long-term observational study in the 1960s, Hope-Simpson4 showed that HZ results from reactivation of the varicella-zoster virus (VZV) in sensory ganglia after a long latency period following primary infection from varicella (chickenpox). In some patients particularly in the elderly, the pain continues to persist after the rash heals and develops into postherpetic neuralgia (PHN), which is the most common complication. PHN causes physical disability, emotional distress and interference with daily activities and sleep.5 HZ also causes neurological sequelae, HZ ophthalmicus (HZO) with eye involvement or disseminated disease. Severe cases of these complications often require hospitalisation.
A live-attenuated VZV vaccine (ZOSTAVAX by Merck) has been demonstrated to significantly reduce the incidences of HZ and PHN in addition to the severity and duration of pain associated with HZ.6 Public health interventions that promote healthy ageing are increasingly becoming more important, as the elderly population is growing rapidly worldwide. Over the next half century, the proportion of people ≥60 years of age is projected to double, reaching more than 20% of the total population in all regions of the world.7 Moreover, the prevalence of disability in the elderly populations is increasing across the world.8
It is essential for healthcare practitioners and health policymakers to be informed by the best available and up-to-date evidence on the HZ burden of disease. In a previous review by Thomas and Hall9, there were limited population-based studies on HZ incidence. Since then, many studies have been conducted across countries to examine the incidence rates and temporal trends of HZ. Other reviews have been restricted to specific geographic regions.10 ,11 Moreover, to the best of our knowledge, there has been no systematic review of studies examining the risk of complications and hospitalisation. The objective of this study is to characterise the incidence rates of HZ and risk of complications across the world. We systematically reviewed studies examining the incidence rates of HZ, temporal trends of HZ, risk of HZ complications including PHN and HZ-associated hospitalisation and mortality rates in the general population.
Methods
Literature search
We performed a literature search in PubMed, EMBASE, and the WHO's Global Health Library Regional Index up to December 2013. For PubMed, we used Medical Subject Headings (MeSH) and the title terms ‘herpes zoster’, ‘zoster’ or ‘shingles’ in combination with the term ‘incidence’. We also searched eligible articles using MeSH and the title terms ‘postherpetic neuralgia’ or ‘post-herpetic neuralgia’. We used the same search strategy with text terms in EMBASE and the WHO library. We manually searched the references cited by the retrieved articles and review articles for additional references. Two investigators (KK and BG) independently conducted a systematic review of the literature, assessed study eligibility and extracted data. Discrepancies were settled through discussion with a third investigator (CJA).
Inclusion and exclusion criteria
We included studies examining the incidence of HZ, risk of PHN, risk of a recurrent episode of HZ, risk of HZO, HZ-associated hospitalisation or HZ-associated mortality. For studies examining the efficacy or effectiveness of vaccination against HZ, we included estimates of incidence rates among unvaccinated individuals. We did not apply language restrictions. We did not include studies limited to children, immunocompromised populations (eg, HIV, cancer and chronic kidney disease) or patients on immunosuppressive therapy (eg, corticosteroids). We also excluded review articles and case reports.
Data extraction
We developed a standard abstraction form for data extraction. We extracted information regarding authors, publication year, journal, country, study design, study year(s), population, number of cases, number at risk, case definition, case ascertainment, incidence rates of HZ (per 1000 person-years), risk of PHN and other complications, HZ-associated hospitalisation rates and HZ-associated mortality rates. For studies on incidence that did not report 95% CI, we computed exact 95% CI.
Results
After conducting a literature search, we included 130 studies conducted in 26 countries in this review (figure 1). There were 63 studies on the incidence of HZ from 22 countries3 ,4 ,6 ,12–71; 25 studies on trends of HZ from 7 countries3 ,12 ,15–19 ,23–25 ,27 ,28 ,49 ,53 ,65 ,68 ,72–80; 60 studies on PHN from 19 countries3 ,4 ,6 ,12 ,18 ,33–36 ,38 ,40 ,42 ,43 ,46 ,54 ,56 ,60–63 ,69 ,81–118; 9 studies on HZ recurrence from 5 countries4 ,12 ,13 ,57 ,60 ,119–122; 12 studies on HZO from 5 countries12 ,35 ,43 ,61 ,123–130; 28 studies on hospitalisation rates from 14 countries24 ,26 ,27 ,30 ,37 ,41 ,44 ,46 ,48 ,52 ,55 ,56 ,58 ,62–64 ,72 ,73 ,76 ,77 ,131–137 and 10 studies on mortality rates from 10 countries.26 ,30 ,37 ,41 ,44 ,48 ,58 ,62 ,134 ,138
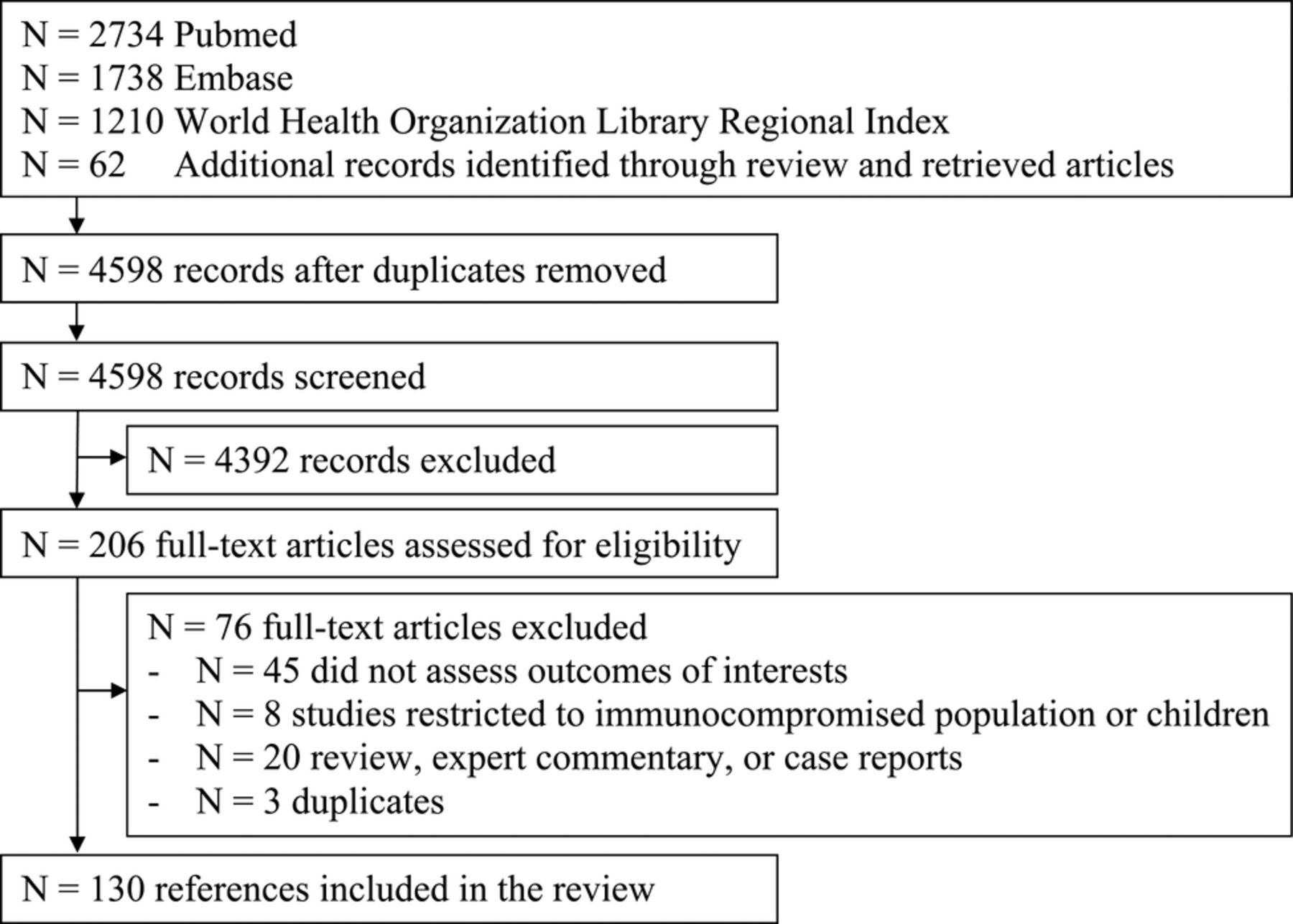
Study selection.
Incidence rates of HZ
Studies examining the incidence rates of HZ were conducted in countries from North America (N=18), Europe (N=33), Asia (N=7), South America (N=3) and the Middle East (N=2; table 1). The incidence rate of HZ ranged between 3 and 5/1000 person-years in North America, Europe and Asia-Pacific, based on studies using prospective surveillance, electronic medical record data or administrative data with medical record review. The age-specific incidence rates of HZ were similar across countries, with a steep rise after 50 years of age (figure 2). The incidence rate was about 6–8/1000 person-years at 60 years of age and 8–12/1000 person-years at 80 years of age. We observed an increase in the reported incidence rate over time within a country. For example, studies conducted more than 20 years ago in the USA by Ragozzino et al12 and Donahue et al13 showed lower rates compared with studies conducted in recent years. It is noteworthy that prospective population-based studies that identified relatively small numbers of patients with HZ (eg, by Scott et al,33 Paul and Thiel,39 Di Legami et al55 and Lionis et al59) estimated lower incidence compared with other studies.
Incidence of HZ

{kind=link}
{kind=link}
Age-specific incidence rate of herpes zoster in North America, Europe and Asia-Pacific.
Trends of HZ incidence
In the USA, studies conducted during the postvaricella vaccination era showed inconsistent results, with some showing no change in incidence but others reporting an increase in HZ incidence, suggesting a potential impact of varicella vaccination (table 2). However, Leung et al,19 Hales et al23 and Yawn et al75 examined trends over a longer period and found that incidence rates increased continuously across all age groups before the introduction of the varicella vaccination programme and continued to increase throughout the postvaccination era. These studies concluded that the increase was not due to the varicella vaccination programme. Most studies conducted in Canada, the UK, Spain, Taiwan and Japan reported an increase in the incidence of HZ over the past decade often occurring in the absence of the national varicella vaccination programmes.24 ,25 ,49 ,65 ,68 Several studies in Australia suggested increasing trends in HZ outpatient visits or hospitalisation during prevaricella and postvaricella vaccination eras.76 ,77 ,79
Temporal trends of herpes zoster
Risk of PHN
The risk of developing PHN varied from 5% to more than 30% (table 3; 49 studies). The estimated risk of PHN varied by study design, age distribution of study populations and definitions used for PHN. For studies that used multiple definitions of PHN, we present results based on the definition of at least 90 days of persistent pain. Studies that reported risk of PHN by age groups consistently found that older patients have a greater risk of developing PHN (see online supplementary table S1). In this review, we found that researchers have used a different duration of persistent pain (persisting for 30, 90 or 180 days) and severity of pain (clinically meaningful pain or any pain) to define PHN. For example, 18% of patients had pain for at least 30 days and 10% for at least 90 days in a population-based study using medical records by Yawn et al3 in the USA. Similarly, 20% of patients had pain for at least 30 days and 14% for at least 90 days in a study by Gauthier et al34 in the UK. Administrative database studies (eg, Ultsch et al42 (4.5%), Opstelten et al43 (2.6%) and Gialloreti et al56 (6.2%)) were more likely to report a lower estimated risk of PHN compared with other studies. Researchers have used diagnosis and medication data in various algorithms, many of which are not validated. It is noteworthy that retrospective studies involving specialists (eg, Mick et al38 (32.5%), Kanbayashi et al102 (52%) and Ro et al103 (39.4%)) may have included existing severe cases of patients with PHN and possibly overestimated the overall risk of PHN.
Risk of PHN in patients with herpes zoster
We identified six prospective cohort and three cross-sectional studies examining the duration of PHN in North America and Europe (table 4). Several studies reported that PHN may last up to 10 years. Prospective cohort studies demonstrated that approximately 30–50% of patients with PHN experienced pain lasting for more than 1 year. Cross-sectional studies also reported a similar high proportion of patients with PHN; however, these studies are most likely an overestimate because they are more likely to include patients experiencing a longer duration of pain.
Duration of postherpetic neuralgia (sorted by study design)
Risk of recurrence
A limited number (N=9) of studies examined recurrence of HZ. Four studies reported a risk of <1.5%, with three of these studies conducted over 1–2 years of follow-up.13 ,57 ,119 ,122 About 2.9% of patients had recurrence of HZ in Israel during 2 years of follow-up, while 2.3% of patients had recurrence in South Korea up to 10 years of obervation.60 ,121 However, studies with a long-term follow-up period tended to report a higher risk of recurrence. Hope-Simpson et al115 reported that 4.7% had recurrence of HZ during 16 years of follow-up in the UK. Similarly, Ragozzino et al12 reported that 5.3% of patients had episodes of recurrence during more than 20 years of follow-up. A recent study by Yawn et al120 also demonstrated that a recurrence of HZ occurred with a rate of 6.2% after 8 years of follow-up. The risk of recurrence may also depend on immune status.120 Thus, overall risk of recurrence may vary by inclusion of those immunocompromised individuals.
Risk of HZO
HZO occurs when VZV reactivation affects the distribution of the ophthalmic division of the trigeminal nerve and can occur with or without eye involvement. Although the number of population-based studies is limited, similar risks of HZO were reported across studies. The reported risks of HZO among patients with HZ were 10.1% (Ragozzino et al,12 USA), 12.3% (Chidiac et al,35 France), 14.4% (Opstelten et al,43 the Netherlands) and 14.9% (Alakloby et al,61 Saudi Arabia). Borkar et al124 reported an overall incidence of 30.9/100 000 person-years, which corresponds to an approximately 10% risk among patients with HZ in the USA. As has been previously recognised, the risk of HZO is similar across age groups.123 ,124
A wide range of eye complications, such as keratitis, uveitis and conjunctivitis, could result from HZO. The reported risk of these eye complications in patients with HZO ranged widely from approximately 30% to 78%.125–129 In a population-based study in the USA, the risk of HZO with eye involvement among patients with HZ was 2.5%.130 The HZ-associated eye complications required an average of 10 months of medical care with 6% of cases resulting in vision loss.130
Hospitalisation rates associated with HZ
We identified 28 studies that reported HZ-associated hospitalisation (table 5). All studies used hospital discharge or claims data. Rates of HZ-related hospitalisation ranged widely from 2 to 25/100 000 person-years in studies examining all ages. The variation in the estimates may reflect the differing admission criteria in the different settings. Hospitalisations with a primary diagnosis of HZ accounted for about 29–42% of HZ-related hospitalisations.37 ,62 ,73 Studies that included hospitalisations with non-primary diagnosis codes (eg, secondary) may have overestimated the hospitalisation rate because they may represent prior or incidental HZ. Hospitalisation rates increased steeply with age, with the majority of the cases occurring in adults ≥50 years of age. For example, Jackson et al73 reported HZ-associated hospitalisation rates (confirmed with medical records) ranging from 10/100 000 in adults 60–69 years of age to 65/100 000 in adults ≥80 years of age in the USA. Similarly, the rate of hospitalisation with primary diagnosis of HZ ranged from 13/100 000 in adults 60–64 years of age to 96/100 000 in adults ≥80 years of age in Australia.62 The rates ranged from 31/100 000 in adults 60–64 years of age to 100/100 000 in adults ≥80 years of age in Germany.41
Hospitalisation rates associated with herpes zoster
Mortality rates associated with HZ
Mortality rates associated with HZ ranged from 0.017 to 0.465/100 000 person-years in studies (see online supplementary table S2). Most studies reported that the majority of deaths occurred in adults ≥60 years of age.
Discussion
HZ is a significant global health burden that is expected to increase as the population ages. The incidence rises steeply after 50 years of age and many working-age adults and elderly individuals are at increased risk. Risk of complications, particularly debilitating and long-lasting PHN, and hospitalisation is common in the elderly population. The major strength of our study is that we assessed the HZ burden across the globe and comprehensively reviewed incidence, risk of complications, hospitalisation and mortality. Our review included 63 studies on incidence, substantially more than the prior review by Thomas and Hall,9 which included 17 studies with overall incidence ranging from 1.2 to 4.8/1000 person-years. Other reviews were restricted to specific geographic regions and/or assessed only incidence.10 ,11
Relatively similar estimates of the HZ incidence rate (between 3 and 5/1000 person-years) were reported in North America, Europe and Asia-Pacific. However, we observed some variations in estimates most likely due to the various study designs, case ascertainments, age distributions of the population and year of the study. It is difficult to accurately estimate the incidence rates because it is not a commonly reportable disease and surveillance systems are not usually in place. Most studies had limitations in their study methodology. Almost all studies may be susceptible to under-reporting due to patients who did not seek medical care. However, administrative database studies using diagnostic and billing codes may have overestimated the incidence due to misclassification. Several validation studies reported a relatively high sensitivity for the International Classification of Diseases (ICD)-9 code (98%) and positive predictive value (PPV; 84–94%).15 ,83 ,139 Furthermore, studies using administrative insurance data may lack generalisability because they may not be representative of the general population. Population-based surveillance studies face difficulty in estimating the numbers of the population at risk in the study catchment area. Several prospective cohort studies that identified relatively small numbers of patients with HZ (eg, by Scott et al, Paul and Thiel, Di Legami et al and Lionis et al) may have underestimated the rate of HZ due to under-reporting of cases or inaccuracy in estimating the numbers of the population at risk. In spite of these limitations, it is reassuring to find similar incidences across countries in well-conducted studies.
There is a scarcity of research examining the incidence of HZ in Asia, Latin America and Africa. HZ may be regarded as a low health priority in many of these countries; however, the proportion of people ≥60 years of age is projected to double in the next several decades, and the numbers of HZ cases are expected to increase substantially. Further research is needed because it is unclear whether the incidence would be similar in these regions. Age-specific incidence rates may vary because of the regional differences in epidemiology of varicella infection and VZV genotype distribution. Varicella primarily affects young children in temperate countries, whereas varicella tends to occur at a later age during adolescence and adulthood, presenting in severe form with frequent risks of complication and mortality in tropical countries.140 ,141 Severe varicella infections during adolescence may result in greater numbers of VZVs remaining latent and possibly resulting in earlier reactivation of VZV.142 The distribution of VZV clades varies globally.143 ,144 VZV can be classified into at least five major clades. VZV clades 1 and 3 are dominant strains in Europe and the Americas, whereas clade 2 is a dominant strain in Asia and clade 5 in Africa.143 Molecular epidemiology of VZV is still an active area of investigation and requires more research. Furthermore, the incidence of HZ may be higher in the countries heavily affected by HIV/AIDS or other immunocompromising conditions.
Hope-Simpson4 hypothesised that exogenous exposure to VZV from individuals with varicella or HZ may boost VZV-specific cell-mediated immunity and thereby decrease the risk of HZ. Because varicella vaccination programmes reduce VZV circulating in the community, thus potentially leading to a decrease in the opportunity for boosting immunity against VZV, it has been hypothesised that the introduction of varicella vaccination might increase the incidence of HZ in the population. However, based on the current literature, there is no conclusive evidence as to whether varicella vaccination programmes have been associated with an increase in the incidence of HZ. In fact, a number of studies across countries have found an increase in the incidence of HZ before introduction of the varicella vaccination programme. It is unclear why the incidence of HZ is increasing. The temporal change or emergence of infectious disease is usually due to changes in the society, technology, virus itself or environment, such as climate change.145 The temporal increase was independent of age. It may partly be explained by an increase in the prevalence of risk factors, an increase in the use of immunosuppressive agents (eg, chemotherapy) or an increase in diagnosis through improved access to healthcare and public awareness. Because HZ is usually clinically diagnosed, diagnostic modalities are unlikely to have affected the reported incidences. Given the steady continuous increase in the incidence of HZ across age groups, it is plausible that a genetic change in the VZV may be playing a role. For example, a study in the UK suggested that changes in genotype distribution have occurred through importation of different strains.146 Although VZV is considered a genetically stable virus, a recombination between different VZV strains could possibly occur.143 ,147
We reviewed the risk of PHN in patients with HZ. Several long-term prospective cohort studies demonstrated that more than 30% of patients with PHN could experience pain lasting for more than 1 year. The reported risk of developing PHN in patients with HZ varied widely from 5% to more than 30%. The risk of PHN may have differed across countries due to the varying prevalence of disability and other underlying comorbidities in the elderly population.8 ,148 However, we could not conclude whether the risk of PHN differed by country because of wide variation. The wide variation in the estimates could be partly due to the different study designs used in prior studies. Prospective cohort studies of patients with HZ tend to report greater risk of PHN than studies utilising electronic medical records or administrative databases. We found that administrative database studies often face a numbers of challenges in identifying patients with PHN and they are likely to underestimate the risk of PHN. Currently, there is only one study, by Klompas et al,83 that developed and validated an algorithm for PHN using ICD-9 codes and claims for a filled prescription. The algorithm detected PHN with a sensitivity of 86% and PPV of 78%; however, they defined PHN as a persistent pain for 30 days or more after zoster onset rather than 90 days or more. More validation studies are needed.
Researchers used different definitions of PHN. A difficulty in reaching consensus on a definition for PHN is probably due to a multifactorial pathophysiological nature of the condition and difficulty in objectively assessing the pain.149 Patients with PHN also experience different types of pain including a steady burning pain, a sudden stabbing pain or stimulus-evoked pain (allodynia). The best option for defining PHN would be clinically meaningful pain lasting for more than 90 days after rash onset, considering the pathophysiology and definitions suggested from prior trials on antiviral treatment and zoster vaccination.6 ,150 ,151 We also believe that healthcare utilisation patterns and prescribed treatment for PHN vary across countries and that characterising the treatment patterns would be important for future research.
Several prior studies with a long-term follow-up found that recurrence of HZ is frequent, with a rate of 5–6%, which is comparable to rates of first occurrence of HZ. However, a limited number of studies examined the risk of recurrence and more studies are needed to confirm these findings. There were a limited number of population-based studies examining HZO, a severe condition that may lead to significant visual impairment.
Several limitations of this review are worth noting. Because the quality of the study, study design and age distribution of population varied widely across studies, we could not synthesise the data quantitatively to estimate the pooled incidence rates. We did not conduct a formal study quality assessment. However, we described the study design and outcome ascertainment of each study and discussed limitations of studies. Our review focused on general populations, primarily immunocompetent populations, and we did not include studies restricted to immunocompromised populations (such as HIV/AIDS, malignancy or autoimmune disease). Our review also did not include uncommon complications of HZ, such as Ramsay Hunt syndrome, Bell's palsy and transverse myelitis.
In conclusion, similar age-specific incidence of HZ was reported in North America, Europe and Asia-Pacific; however, there is a scarcity of research from other regions. Risk of complications, particularly PHN, and hospitalisation is common in the elderly population. HZ is a global health burden that is expected to increase as the population ages across the world in the near future. The prevalence of disability in the elderly populations is also increasing. It is important for healthcare practitioners and health policymakers to consider implementing effective preventive measures such as vaccination against HZ across the globe.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Contributors KK, BG and CJA designed the study. KK and BG conducted the literature search and extracted data. KK wrote the first draft of the manuscript. KK, BG and CJA interpreted the data, critically revised the manuscript and approved the final version of this manuscript.
-
Funding Merck & Co, Inc.
-
Competing interests KK is a consultant working for Merck & Co, Inc. BG is a research fellow funded by Merck & Co, Inc. CJA is employed by Merck & Co, Inc.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.