Article Text

Abstract
Aims The accuracy of biomarker assessment in breast pathology is vital for therapy decisions. The therapy predictive and prognostic biomarkers oestrogen receptor (ER), progesterone receptor, HER2 and Ki67 may act as surrogates to gene expression profiling of breast cancer. The aims of this study were to investigate the concordance of consecutive biomarker assessment by immunocytochemistry on preoperative fine-needle aspiration cytology versus immunohistochemistry (IHC) on the corresponding resected breast tumours. Further, to investigate the concordance with molecular subtype and correlation to stage and outcome.
Methods Two retrospective cohorts comprising 385 breast tumours with clinicopathological data including gene expression-based subtype and up to 10-year overall survival data were evaluated.
Results In both cohorts, we identified a substantial variation in Ki67 index between cytology and histology and a switch between low and high proliferation within the same tumour in 121/360 cases. ER evaluations were discordant in only 1.5% of the tumours. From cohort 2, gene expression data with PAM50 subtype were used to correlate surrogate subtypes. IHC-based surrogate classification could identify the correct molecular subtype in 60% and 64% of patients by cytology (n=63) and surgical resections (n=73), respectively. Furthermore, high Ki67 in surgical resections but not in cytology was associated with poor overall survival and higher probability for axillary lymph node metastasis.
Conclusions This study shows considerable differences in the prognostic value of Ki67 but not ER in breast cancer depending on the diagnostic method. Furthermore, our findings show that both methods are insufficient in predicting true molecular subtypes.
- breast cancer
- Ki67
- immunocytochemistry
- immunohistochemistry
Statistics from Altmetric.com
Introduction
The prognosis for patients with breast cancer is highly variable and dependent on several prognostic attributes. In recent years, gene expression signatures and intrinsic subtyping based on global mRNA expression have been used to classify invasive breast tumours into high-risk and low-risk subtypes. The PAM50 algorithm divides tumours into four major subtypes: luminal A and B, human epidermal growth factor receptor 2 (HER2) enriched and basal-like.1 These subtypes can also be recapitulated to some extent by using the immunohistochemical (IHC) biomarkers oestrogen receptor α (ER), progesterone receptor (PR), HER2 and the proliferation-associated nuclear protein Ki67.2–5 Since treatment decisions are based on these IHC-determined biomarkers, its accuracy is vital. Unfortunately, biomarkers are prone to intraobserver and interobserver variability, which hampers their reproducibility. This is especially evident for Ki67.6 7 According to international guidelines, ER, PR, HER2 and Ki67 should be analysed by IHC on the resected primary tumour or on a preoperative core biopsy.3 8 During tumour progression, biomarker expression can switch from expression to non-expression and vice versa.9 This highlights the importance of tumour reassessment in the metastatic or relapse setting, particularly when deciding on targeted treatment modalities.9–11 This reassessment is typically performed on core biopsies or fine-needle aspiration cytology. However, since biomarker evaluation on breast cytology has not been validated in prospective trials, adjuvant or neoadjuvant treatment decisions should preferentially be based on histological material. Fine-needle aspiration, however, is sometimes the only choice to obtain tumour cells from distant metastatic lesions.
In the local clinical setting immunocytochemical (ICC) assessment is in some cases performed on cytological material from breast tumours even though a re-evaluation by IHC on histological material follows. This dual analysis provides a unique opportunity to investigate and compare the diagnostic efficacy of both methods. Related to this, we have previously shown that Ki67 and other predictive biomarkers differ in preoperative fine-needle aspiration cytology compared with resected primary breast tumours.12 The aims of the present study were to investigate the concordance of consecutive biomarker assessment in invasive breast tumours performed on preoperative fine-needle aspiration cytology using ICC and on the tumour resection specimen using IHC, and to investigate concordance with molecular subtype and outcome with both methods.
Materials and methods
Patient records and registry
For this study, two retrospectively obtained cohorts of breast cancer tumours were included and the study was approved by the Regional Ethical Review Board at Karolinska Institutet (2 December 2015, ref: 2013/1274-31/4 with amendment 2015/2090-32, and 2013/1833-31/2). As it was a retrospective study using pre-existing specimen, written consent was not required.
Cohort 1 comprised 301 primary breast tumours. Through the laboratory information system at Karolinska University Laboratory, 1671 cases with fine-needle aspiration cytology of the breast during 2005 and 2006 were identified (online supplementary figure 1). Cytological benign lesions, recurrent breast tumours (subject to previous treatment) and cases without Ki67 included in the biomarker assay were excluded (n=1154). The consecutive surgical resections with Ki67, and when available also ER, PR and HER2 assessment, had been analysed at the Department of Clinical Pathology, Karolinska University Laboratory or at the Department of Clinical Pathology, Capio S:t Görans Hospital in Stockholm, Sweden. Of 392 cases with both Ki67 evaluations by ICC from aspiration cytology and by IHC from resection specimen, 301 were included in the study. Reasons for further exclusion were as follows: neoadjuvant treatment (n=43), no numeric Ki67 value (n=39), previous breast cancer diagnosis within 5 years (n=9). In total, 299 patients remained with 301 invasive tumours (one bilateral cancer) of the breast (table 1). Six patients had a breast cancer diagnosis in the same breast more than 5 years prior to the diagnosis in this study (11 with contralateral breast cancer and one with unknown laterality). Further clinical data were obtained from the patient medical record system. All events of breast cancer recurrence, locoregional and distant metastasis as well as date and cause of death were gathered from detailed clinical follow-up history and the cause of death certificate, when available. Overall survival was defined as time from date of diagnosis to death or end of follow-up and breast cancer specific survival was defined as time from diagnosis to breast cancer caused death by end of follow-up.
Supplementary file 1
Characteristics of patients and material for cohorts 1 and 2 included in this study
Cohort 2 consisted of 194 mainly primary breast tumours from the Karolinska University Hospital in 2002–2010 and Stockholm South General Hospital in 2012, both in Stockholm, Sweden, with available biomarker evaluations performed on resected tumours using IHC and PAM50 gene assay data from consecutive tumours (table 1; online supplementary figure 1). This cohort has previously been published.13–15 No follow-up data were yet available for this cohort. Of these cases, 84 had corresponding preoperative aspiration cytology with ICC-assessed biomarkers performed, identified through the laboratory information system. This cohort was, in addition, used for analysis for concordance in IHC surrogate subtype and PAM50 subtype between cytology and corresponding tumour resection.
Eligible cases and biomarkers
In cohort 1, the women had a mean age of 62 years at diagnosis (SD 14.1, range 25–92 years), and the patients’ medical record was accessed at end follow-up in April to July 2016 at which time 27% of the patients were deceased. The median follow-up time was 10.3 years. From the 301 tumours, available data on ER, PR, HER2 and Ki67 evaluations on aspiration cytology and corresponding tumour resections from routine pathological assessments, as well as patient age at diagnosis, gender, tumour variables (invasive tumour size, Nottingham histological grade and histological type) and axillary lymph node involvement were collected and analysed (table 1), according to the College of American Pathologists’ guidelines.16
For 84 tumours with corresponding cytology and PAM50 molecular subtype in cohort 2, additional data on ER, PR and Ki67 evaluations from routine cytological assessments using ICC were collected and analysed. Of these, 70 tumours had ICC Ki67 evaluation and ICC-assessed ER and PR were available for 78 and 65 cases, respectively (table 1).
ICC and IHC
At the Department of Clinical Pathology and Cytology, Karolinska University Laboratory, fine-needle aspiration-based cytological assessment is performed by smear cytological evaluation along with air-dried smears for ICC analysis of ER, PR and Ki67. This protocol has previously been described.12 HER2 testing was not performed on cytology smears. Liquid-based cytology techniques were not routinely performed at the Karolinska University Laboratory and cell block preparations were only used for specific cases and therefore not available for this study. According to standard procedures, all smear cytology samples had been read by two cytologists at primary diagnosis.
The IHC biomarker assay (ER, PR, Ki67, HER2) was performed from an adjacent section to the H&E sample from the resected breast tumour tissue, according to previously described protocols.12 14
The routine pathological evaluation of hormone receptor status was performed through manual assessment of the percentage of ER-positive and PR-positive cells in the entire invasive tumour or on the smear cytology glass slide. The ER and PR cut-off was set to ≥ 1% for positive assessment in this retrospective analysis. Ki67 index was assessed by manual count of the percentage of positive stained tumour cells out of at least 200 tumour cells in the ‘hot-spot’ area with the highest positive stained tumour cell density (online supplementary figure 2).8 17 For HER2 evaluations, the intensity of membrane protein staining of the tumour cells of the entire glass slide was assessed and scored 0, 1+, 2+ or 3+. According to routine guidelines fluorescent in situ hybridisation was performed for the majority of IHC 2+ and 3+ tumours to determine HER2 gene amplification.8
PAM50 gene expression-based subtypes
RNA sequencing methods of snap-frozen tissue from the resected tumours of cohort 2 have been described before.13 15 Based on the PAM50 gene expression algorithm, these tumours were assigned a molecular subtype (luminal A, luminal B, HER2 enriched or basal-like) and used for this study.13 15
Surrogate subclassification
The assessments of ER, PR, Ki67 and HER2 when available from cytological and resected tumour material were combined into IHC surrogate subtypes for the four gene expression-based subtypes luminal A and B, HER2 enriched and basal-like, using definitions stated by expert recommendations.2 3 18 To date, there is no established agreement for standardisation of Ki67 measures for routine clinicopathological purposes. However, in the St Gallen 2013 consensus, the use of Ki67 index with a cut-off of <20% for ER-positive HER2-negative tumours was recommended,4 and in 2015 the cut-off value within 20%–29% was mainly accepted for the division between luminal A-like and luminal B-like tumours.3 Based on these international recommendations, and adjusted to laboratory-specific protocols at the Karolinska University Laboratory, high proliferation was defined as Ki67 ≥20% in this study. The surrogate subtype classifications used in the present study were ‘Luminal A-like’: hormone receptor (HR) positive, HER2 negative and Ki67 <20%; ‘Luminal B-like’: HR positive, HER2 negative and Ki67 ≥20% or HR positive, HER2 positive and any Ki67; ‘HER2-enriched’: HR negative, HER2 positive and any Ki67; ‘Triple-negative’: HR negative, HER2 negative and any Ki67.
Statistical methods
Independent samples Mann-Whitney U tests were used to compare non-parametric group data. Pearson’s correlations and Spearman’s rank order coefficients were calculated for correlation of Ki67 indices in cytology versus tumour resections, and for tumour size versus axillary lymph node engagement. Cohen’s κ statistics were computed for agreement of high and low proliferation and tumour subtype. The Kaplan-Meier method was used for survival analysis. Cox regression likelihood ratio (LR) χ2 and change in LR (LR−Δχ2) were used to test individual and relative prognostic values of ICC and IHC-assessed Ki67. Cox regression HR for all-cause mortality and breast cancer-specific mortality was calculated and presented as forest plots. Receiver operating characteristic was performed for ICC and IHC Ki67 with equal emphasis on sensitivity and specificity for survival outcome. All p values were two sided and significance was considered at p<0.05. All data analyses were performed using IBM SPSS Statistics V.23 (IBM). Sankey diagrams were computed using JSFiddle V.0.5a2 (http://jsfiddle.net). Forest plots were created using Microsoft Excel for Mac 2017 (Microsoft, Redmond, WA, USA).
Results
Ki67 and ER by ICC versus IHC
In the combined cohorts (n=385), 369 tumours had numerical Ki67 index in cytology and corresponding tumour resection with a median Ki67 index of 12% (range 0%–80%) and 20% (range 0%–100%), respectively (figure 1A). There was a significant positive correlation between ICC and IHC-assessed Ki67 index (r=0.629, n=355, p<0.001; figure 1B). Three hundred and sixty tumours were evaluated for ‘low’ and ‘high’ Ki67 status using a ≥20% cut-off, and for 121 tumours (33.6%) there was a change in classification between cytology and corresponding tumour resection (figure 1C). Among the IHC low tumours, 19 were considered high by ICC. Conversely, among IHC high tumours, 102 were classified as low by ICC. This showed a 33.6% discordance in classification between the two assessments (Cohen’s κ=0.354, n=360; figure 1C). ER evaluations by ICC and IHC for the same tumour were available for 345 tumours, and 12 tumours (3.5%) switched ER status between cytology and corresponding tumour resection. Consequently, here the concordance for ER between the two methods was 96.5% (Cohen’s κ=0.882, data not shown). To confirm this high ER concordance, smear cytology slides from the 12 discordant ER cases were re-evaluated by a board-certified cytologist (EDR), who was blinded to the original score. This resulted in an even improved concordance in classification between cytology and tumour resection (98.5%, total n=342, Cohen’s κ=0.949, data not shown). However, three of the cases were not available for reassessment.

Comparison of Ki67 assessment and discordance status of Ki67 between preoperative fine-needle aspiration cytology and resection specimen of sequential breast tumours. (A) Box plots showing median, quartiles, range, outliers (circles) and extremes (asterisks) for Ki67 index assessment by immunocytochemistry (ICC) and immunohistochemistry (IHC) from 369 breast tumours in cohorts 1 and 2. (B) Scatter plot of Ki67 index in IHC and ICC for tumours in cohorts 1 and 2. (C) Discordant status of ICC-assessed Ki67 ‘low’ and ‘high’ of tumours using a ≥20% cut-off for positive classification in cohorts 1 and 2. The green bar indicates tumours where there is concordance between IHC and ICC (n=239). The blue bars indicate tumours where there is discordant Ki67 status between IHC and ICC (n=121).
IHC surrogate subtype reclassification
ER, PR, Ki67 (≥20%) and HER2 status were available and used to classify 339 out of 385 tumours in cohorts 1 and 2, into the IHC-based surrogate subgroups. Of these 339 tumours, 119 (35.1%) switched IHC surrogate subtype between cytology and tumour resection assessment (figure 2; online supplementary table 1). The concordance of IHC surrogate subtypes between cytology and tumour resection when ‘ICC or IHC n/a’ was excluded (n=46) was 64.9% (Cohen’s κ=0.44).

Sankey diagram illustrating the flow of breast cancer surrogate subtype reclassifications between sequential immunocytochemical (ICC) and immunohistochemical (IHC) evaluations from cytology and tumour resection, respectively (cohort 1 n=301, cohort 2 n=84). *HER2 status was generally not assessed by ICC, thereby precluding the distinction between triple-negative and HER2-enriched tumours within the hormone receptor-negative subset.
Survival analysis
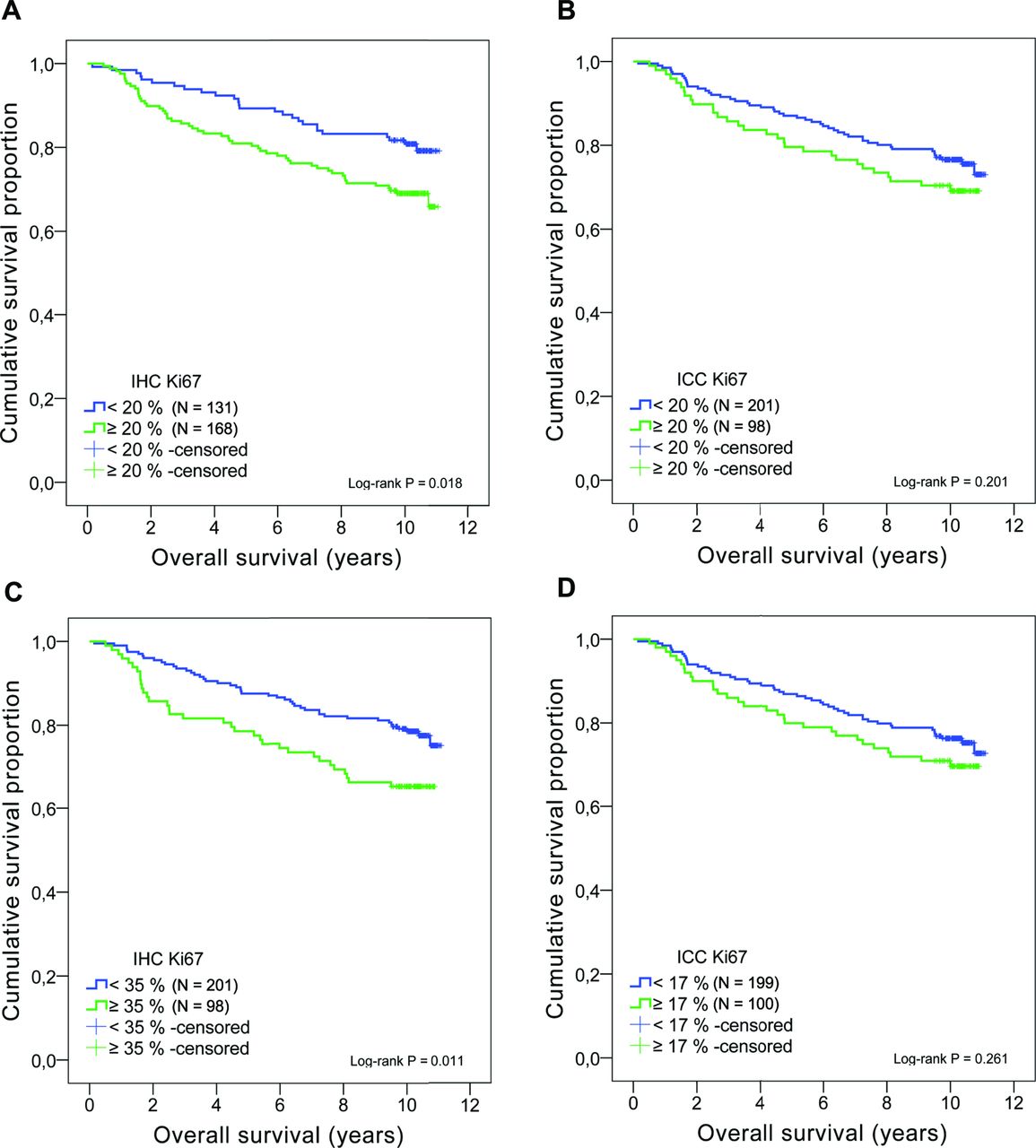
In cohort 1, the 10-year overall survival for all subgroups was 72.8% and statistically significant differences in overall survival of cases with ‘low’ and ‘high’ Ki67 were observed when assessed on tumour resections using IHC (log-rank p=0.018; figure 3A). There was no significant difference in overall survival time for ‘low’ versus ‘high’ Ki67 assessment on smear cytology (log-rank p=0.201; figure 3B). Furthermore, when cases with IHC Ki67 in tumour resections were analysed for Cox regression HRs, cases with high Ki67 (≥20% cut-off) had a significantly higher hazard for all-cause mortality compared with cases with low Ki67 (HR 1.748, 95% CI 1.093 to 2.795, p=0.020; online supplementary figure 3). For ICC Ki67 (≥20% cut-off), the HR was not significant (HR 1.344, 95% CI 0.853 to 2.117, p=0.203; online supplementary figure 3).
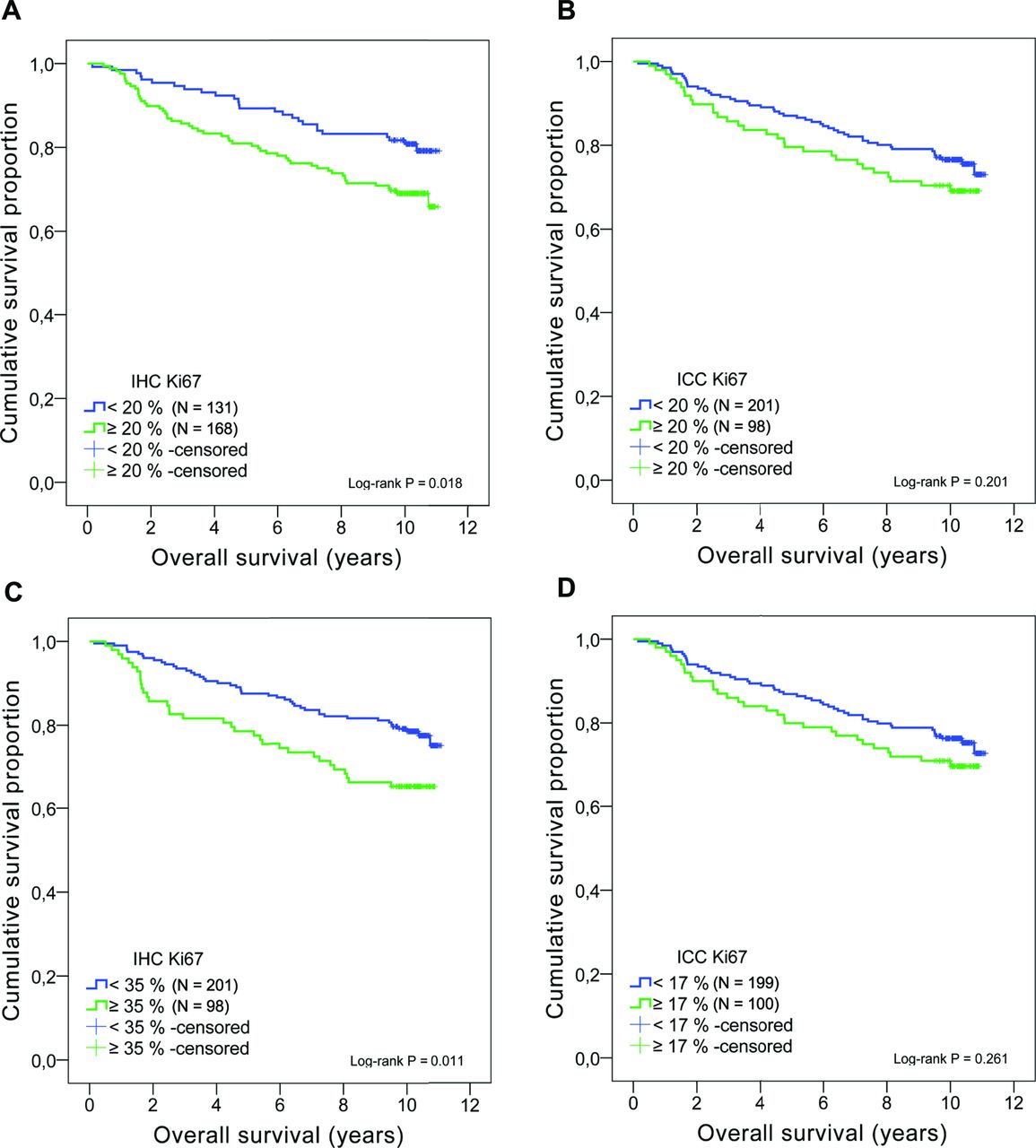
Kaplan-Meier estimate of overall survival functions by Ki67 status for cohort 1. (A) Overall survival comparison of immunohistochemistry (IHC)-assessed Ki67 in tumour resections using a ≥20% cut-off (log-rank p=0.018). (B) Overall survival comparison of immunocytochemistry (ICC)-assessed Ki67 in cytology using a >20% cut-off (log-rank p=0.201). (C) Overall survival comparison of Ki67 in tumour resections using a 2/3 cut-off. The 35% Ki67 cut-off corresponds to the highest third for IHC with a significant decreased overall survival (log-rank p=0.011). (D) Overall survival comparison of Ki67 in cytology using a 2/3 cut-off. The 17% Ki67 cut-off corresponds to the highest third for ICC (log-rank p=0.261).
When analysing hormone receptor positive tumours separately, the difference in overall survival for Ki67 <20% versus >20% on tumour resections showed a similar trend towards significance (log-rank p=0.075). In the hormone receptor negative cases, there was no significant difference in survival between cases with Ki67 <20% versus >20% (log-rank p=0.893; online supplementary figure 4).
The recommendation in Sweden is that each pathology laboratory sets its local cut-off for high proliferation, in order to calibrate the cut-off level against staining equipment, IHC technique and antibody clone which may affect the cut-off. The cut-off for high proliferative tumours is considered as the percentage level that discriminates 1/3 of the tumours with highest proliferation from the 2/3 of the population considered low proliferative (determined from the last 200 cases retrospectively). A cut-off of 2/3 for high proliferation has been established for setting the local Ki67 cut-off, in this study referred to as the ‘2/3 cut-off’.8 19 With a 2/3 cut-off, high Ki67 in surgical resections was associated with worse overall survival (Ki67 cut-off ≥35%, log-rank p=0.011; figure 3C). Analysing the 2/3 cut-off for ‘high’ Ki67 in cytology did not produce a significant difference between the ‘high’ and ‘low’ Ki67 groups (Ki67 cut-off ≥17%, log-rank p=0.261; figure 3D). In the ER-positive resected tumours there was no significant association between overall survival and high Ki67 (Ki67 cut-off ≥35%, log-rank p=0.153; online supplementary figure 4). However, there was a significant decrease in survival for hormone receptor negative cytological assessed tumours with high Ki67 (Ki67 cut-off ≥17%, log-rank p=0.043) although the findings were based on a small number of cases (<17% n=14, ≥17% n=48; online supplementary figure 5).
The 10-year breast cancer-specific survival including all subgroups in cohort 1 was 87.1%, although no significance could be found based on the same Ki67 cut-offs as for overall survival analysis. In this cohort, breast cancer-specific survival time generated too few events for comparison (online supplementary figure 6). Furthermore, the Cox regression HR for breast cancer-specific mortality in patients with IHC Ki67 ≥20%, but not ICC Ki67 ≥20%, was significantly higher than patients with IHC/ICC Ki67 <20% (online supplementary figure 3).
When ICC and IHC scores of Ki67 from cytology and tumour resections, respectively, were tested for their individual prognostic value by Cox regression LR χ2, IHC was found to contribute with significant prognostic information (χ2 5.567, p=0.018), but not ICC (χ2 1.634, p=0.201). IHC Ki67 was then added to ICC-assessed Ki67 for a comparison of their relative amount of prognostic information. Again, the LR−Δχ2 indicated that IHC added significantly more prognostic information than ICC (LR −Δχ2 4.276, p=0.039).
Receiver operating characteristics were analysed for ICC and IHC-assessed Ki67 to identify cut-offs with equal emphasis on sensitivity and specificity for all-cause mortality as well as breast cancer-specific mortality within 5 and 10 years from diagnosis, respectively, in cohort 1. For ICC Ki67 versus breast cancer-specific mortality within 5 years this produced an area under the curve (AUC) of 0.58, a sensitivity of 59.1% and a specificity of 52.7% at a cut-off ≥14.5%. Lower numbers were observed for all-cause mortality within 5 and 10 years as well as breast cancer-specific mortality within 10 years (AUC in the range of 0.548–0.578, sensitivities and specificities in the range of 51.6%–59.4%). Turning to IHC Ki67, larger AUC and higher sensitivities and specificities were produced. IHC Ki67 versus breast cancer-specific mortality within 5 years from diagnosis yielded an AUC of 0.705, a sensitivity of 68.2% and a specificity of 60.2% at cut-off ≥29%, whereas lower numbers were produced for the three other outcome comparisons (AUC in the range of 0.608–0.688, sensitivities and specificities in the range of 54.7%–66.7%). Still, all IHC AUC were higher than any ICC AUC. Considering combining all tested outcome measures, a 14% cut-off (range 12.5%–14.5%) for ICC Ki67 and a 26% cut-off (range 22.5%–29%) for IHC Ki67 were calculated for discrimination of good versus relatively poor prognosis (online supplementary figure 7).
Furthermore, in cohort 1, as determined by independent samples Mann-Whitney U tests, IHC Ki67 was significantly higher in patients with one or several axillary lymph node metastases (≥pN1 a, p=0.016). In contrast, ICC Ki67 was not significantly higher in lymph node-positive patients (p=0.101). Using a >20% cut-off, the OR for lymph node metastasis in patients with high ICC Ki67 was 1.17 (95% CI 0.72 to 1.91), whereas it was 2.07 for patients with high IHC Ki67 (95% CI 1.28 to 3.34).
IHC-based surrogate subtype versus PAM50 subtype
In cohort 2, out of the 63 tumours for which all biomarker ICC values were available, 38 had an IHC-based surrogate subtype identical to its PAM50 subtype (60%, Cohen’s κ=0.23; figure 4). When the tumour resections in the same cohort were assessed, 47 out of 73 tumours had concordant subtypes (64%, Cohen’s κ=0.31; figure 4). Consequently, neither of the two methods was excellent nor superior to the other for agreement with gene expression profiling. Of note, we also tested a PR cut-off of ≥20% to separate luminal A from luminal B patients but this resulted in poor agreement (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Breast cancer subtype reclassifications. (A) Sankey diagram illustrating the flow of breast cancer subtype reclassifications between sequential immunocytochemical (ICC) evaluations and PAM50 gene expression assays (cohort 2, n=63). (B) The flow of subtype reclassifications between sequential immunohistochemical (IHC) evaluations and PAM50 gene expression assays (cohort 2, n=73). *HER2-status was generally not assessed by ICC, thereby precluding the distinction between triple-negative and HER2-enriched tumours within the hormone receptor-negative subset.
Discussion
In breast cancer samples evaluated during routine diagnostic cytology and pathology, we found discordance in Ki67 assessment from preoperative fine-needle aspiration cytology to the corresponding tumour resection. This could partly be explained by tumour heterogeneity and the fact that the assessments were made in different tumour areas, with methods that to some extent analyse dissimilar portions of the tumour. The IHC evaluation was performed in the Ki67 ‘hot-spot’ area of whole tissue sections whereas the ICC evaluation is based on a non-specific small portion of the tumour in which the ‘hot-spot’ is likely to be missed. Importantly, in this study, ER assessments by cytology and consecutive tumour resections showed high concordance (96.5%–98.5%). However, previous results from our laboratory have shown 9% discordance between ICC and IHC-assessed ER using the same cut-off ≥1%.12 This discrepancy could be explained by a smaller sample size in the previous study (eligible patients for ER comparison n=133). Furthermore, breast cancer IHC surrogate subtype classifications showed discordance between cytology and tumour resections. Importantly, based on surrogate classification, both methods were equally poor to distinguish breast cancer molecular subtypes.
To our knowledge, this is the first study investigating the prognostic value of Ki67 protein expression in cytology and comprising a cohort including 10-year survival data. In this material, we found a considerable difference in the prognostic value of Ki67 evaluation depending on the diagnostic method. Moreover, combined material with ICC and IHC biomarker assays in addition to molecular PAM50 data provides valuable information. In a combined analysis comparing tumour classification by PAM50 with IHC surrogate subtypes, Prat et al 20 reported a discordance rate of 30.72% (Cohen’s κ=0.564), which is slightly better than our results, and highlighting the discrepancies of these two methods in identifying intrinsic breast cancer subtype.20 In the luminal spectrum of breast tumours, a concordance of 81%–85% has been reported between PAM50-based luminal A tumours and IHC-based surrogate subtype, whereas 35%–52% of luminal B tumours in this study were also classified as IHC luminal A.18 Regarding IHC subtyping methods and PAM50, the discordance has been well described and published before.2 21 22 The IHC subtypes are all present within each of the PAM50 subtypes,23 a finding with clinical importance among HER2-enriched tumours. Studies show that the highest benefit from anti-HER2 therapy is observed for the HER2-positive tumours by IHC, which are also HER2 enriched by PAM50.24 25 Further, PAM50 has been shown to have the potential to add significant prognostic information to Ki67 and IHC subtypes.26
The prognostic role of IHC-assessed Ki67 has been previously demonstrated,27–31 and there is strong evidence of Ki67 distinguishing good and poor prognostic groups among patients with node-negative breast cancer.32 33 However, the evaluation of Ki67 has been based on different methods and cut-offs for ‘high’ and ‘low’ or ‘positive’ and ‘negative’ assessment. Variation in cut-offs for ‘high’ and ‘low’ Ki67 and the lack of an optimal cut-off are an established issue concerning Ki67.6 17 As described in an earlier paper from our group, local adjustment to optimise Ki67 cut-off is one way to improve discrimination of luminal A versus B tumours.12 In Sweden, we are now implementing a guideline with a Ki67-intermediate subgroup. Within this subgroup, classification into luminal A or B is weighed on PR status and tumour grade.34 Combined with ER, PR and HER2, Ki67 has a prognostic role in subgroups of breast cancer.35 Within ER-positive tumours, high Ki67 identifies patients with poor outcome who should receive chemotherapy.36 37 In the analysis of the ER-negative tumours, there was no significant difference in survival between Ki67 above or below the 20% cut-off (ER-negative ICC-Ki67 <20% n=19, ER-negative IHC-Ki67 <20% n=6), in line with earlier reports describing poor prognosis in ER-negative tumours irrespective of Ki67.1 38 39 It should be noted that the ER-negative cases were few (n=62) limiting the statistical power.
Neither the analyses of overall survival nor breast cancer-specific survival were adjusted for breast cancer stage or adjuvant treatment. However, data on lymph node involvement, adjuvant treatment and relapse or distant metastasis are provided in table 1. Furthermore, tissue-specific cut-offs need to be addressed since Ki67 results differ across different sample types.40
We show here that IHC has a prognostic value for Ki67 assessment in highly proliferating tumours. With a 2/3 cut-off, established for setting the local Ki67 cut-off in pathology laboratories in Sweden,8 19 we show that IHC-assessed Ki67 has a larger prognostic value. Furthermore, these findings are supported by the results showing that tumours with ‘high’ Ki67 in tumour resections had a significantly higher probability for lymph node metastasis. Similar findings were reported by Marrelli et al,41 although a lower cut-off for high proliferation (≥10%) was used.41 High proliferation by Ki67 evaluated on whole sections and tissue microarrays has been associated with lymph node metastasis.40 Ki67 was an independent prognostic factor in patients with breast cancer with ≥4 lymph node metastasis42 and showed increased proliferation in node-positive patients.43 However, in most large studies, there are no clear results that would indicate the ability of Ki67 to discriminate between good and bad prognoses within node-positive breast cancer populations.32
Based on our findings, neither ICC Ki67 high nor low can be regarded as a reliable measure of outcome, since we did not find any prognostic value of cytology-assessed Ki67, but cytology can still be critical in diagnosing early malignancies and thus give valuable clinical information. For a patient with a suspected breast cancer metastasis, biomarker assessment is of great importance to guide treatment. In certain cases, tumour material from the metastasis may only be available through fine-needle aspiration cytology and biomarker evaluations must be performed by ICC. In this study, we have identified concerns and strengths with biomarker assessment in primary tumours, which might be extrapolated to the metastatic setting.
The techniques which give best prognostication and/or prediction are the ones to choose, but the cytological and histological techniques used for biomarker assessment can, however, to some extent not be compared straight off. In the present study, we identified different cut-off levels for ICC and IHC-assessed Ki67 (14% and 26%, respectively) in relation to all-cause and breast cancer-specific mortality. The reason for drawing conclusions on comparisons of ICC and IHC biomarkers in this study is that these methods are the ones available in the diagnostic procedure and for therapy decisions. The use of cell blocks from cytology aspirations may enhance the prognostic value. However, cell blocks require larger amount of cell material and formalin-paraffin processing prolongs the time to diagnosis. Smear cytology has therefore been the standard choice in our laboratory.
In summary, IHC assessment of Ki67 in tumour resections is significantly better than ICC in terms of predicting regional lymph node metastasis and survival outcome. Reliable assessment of prognostic biomarkers is of utmost importance for accurate treatment of patients with breast cancer. Moreover, our results suggest that both IHC and ICC-based surrogate classification of molecular subtypes is suboptimal.
Take home messages
Ki67 index varies substantially between preoperative cytology and corresponding tumour resections of invasive breast cancer.
Only immunohistochemical assessment of Ki67 in invasive breast tumour has a prognostic value.
Immunohistochemistry-based and immunocytochemistry-based surrogate classification of molecular subtypes shows poor concordance.
References
Footnotes
Handling editor Dhirendra Govender.
Contributors SR contributed to study concept and design, data acquisition, interpretation and statistical analyses, and drafting the manuscript. GS contributed to study concept and design, data interpretation and statistical analyses, and drafting the manuscript. EDR contributed to pathological re-evaluations of tissue samples and critically reviewed the manuscript. MR provided gene expression subtype data and contributed to preparation of the manuscript and critically reviewed the manuscript. NPT and JB contributed to preparation of the manuscript and critically reviewed the manuscript. JH contributed to study concept and design, supervision of the study, data interpretation, preparation of the manuscript, and critically reviewed the manuscript. All authors have read and approved the final manuscript.
Funding This work was supported with grants from Swedish Society for Medical Research (SSMF), Swedish Cancer Society, Stockholm Cancer Society, King Gustaf V Jubilee Fund, Karolinska Institutet, Stockholm County Council Research Strategy Committee and Swedish Breast Cancer Association (BRO).
Competing interests JH is a member of the advisory board at Visiopharm, and has obtained speaker’s bureau and honoraria from Roche. Other authors have no competing interests to declare.
Patient consent Not required.
Ethics approval Regional Ethical Review Board at Karolinska Institutet.
Provenance and peer review Not commissioned; externally peer reviewed.