Article Text

Statistics from Altmetric.com
Since vision is the major sensory modality in humans, normal vision is important for the general development of a child.1 2 Visual impairment has significant implications for the affected child and family in terms of education, future employment, and personal and social welfare throughout life.
Using the World Health Organisation (WHO) classification of levels of visual impairment3 (shown in table 1 and used throughout this paper), it is estimated that globally almost one in 1000 children are blind, which is less than a tenth of the prevalence in adults.4 5 However, the 1.5 million blind children in the world account for about 75 million person years of blindness,6 equivalent to the burden due to cataract related blindness, which accounts for 40% of adult blindness worldwide.7 As the combined categories of low vision in childhood (table 1) are three to 10 times more common than blindness,5 6 the total burden of childhood visual impairment is considerable. It has been estimated that globally, the financial costs of childhood blindness incurred by countries, in terms of care and productivity lost, are between 6 and 27 thousand million US dollars.8 Most of this is accounted for by children in high income countries where childhood blindness is less common but life expectancy and earning capacity are greater than in low income countries. Reduction of avoidable visual impairment remains an important international public health goal.
WHO classification of levels of visual impairment (adapted from International Classification of Diseases, 10th revision3)
Knowledge of the magnitude and causes of childhood visual impairment is important to the planning, provision, and evaluation of educational and health services for affected children. This is also essential information for all strategies to reduce visual disability in the population. The purpose of this paper is to review the available data, highlighting relevant sources, on the incidence, prevalence, and causes of childhood visual impairment in Britain which are relevant to both hospital and community based child health.
Normal visual development
The visual system is relatively immature at birth. Maturation depends on both structural and functional changes. Development is particularly rapid in the first year of life, although some changes continue into late childhood.1 9 10 As a child with normal vision only achieves adult levels of visual function at about 5 years,9 it is difficult to predict final visual outcome in younger children with visual defects.
The plasticity of the visual system is a key principle in the management of ophthalmic disease in children. In early life there are “sensitive periods”, of varying length, during which visual function can be profoundly impaired by a variety of insults such as stimulus deprivation arising from congenital cataract.1Additionally “critical periods” exist during which treatment must be instituted to have maximal, or sometimes any effect. Some adverse changes in the visual system become largely irreversible outside these critical periods.1
Measuring visual function
The visual function most frequently measured is distance acuity. However other visual functions, such as visual fields, contrast sensitivity, colour vision, and binocularity may be particularly relevant to overall functional assessment. Despite recent advances in the development and refinement of age appropriate methods for testing vision, the assessment of acuity remains difficult in infants and preschool children as well as those with other disabilities. Young children are increasingly assessed using psychophysical tests based on preferential looking techniques and electrophysiological tests. These are based on different principles and are not directly comparable with each other or with methods used in older children.1 Acuity measurement is less problematic in older children but systems used in testing adults are generally inappropriate for children of less than school age.
Classification of visual impairment
The categorisation of levels and causes of childhood visual impairment is difficult. While the use of standard functional, anatomical, and aetiological classifications has increased, allowing more meaningful interpretation and comparison of studies, some issues remain unresolved.
The impact on a child of a given visual deficit depends, among other factors, on whether the child has any additional disabilities. The current WHO paradigm of impairments, disabilities and handicaps, based on a medical model of disability, does not readily provide an epidemiologically useful classification of childhood visual impairment.11 The WHO classification of levels of visual impairment3 (table 1), based on the distance visual acuity in the better eye measured wearing the best optical correction where necessary, applies to individuals with bilateral visual loss and excludes those with reduced acuity due to refractive errors alone. The definitions of blindness and partial sight for the purposes of registration in Britain12 differ from WHO definitions making extrapolation and direct comparison difficult. A key unresolved issue is the categorisation of young or multiply disabled visually impaired children, in whom acuity is not easily measured.13 All studies of visually impaired children should include an adequate duration of follow up to ensure reliable assessments of a range of visual outcomes.
The classification of the underlying or associated causes of visual loss has also been problematic. Table 2 summarises the system developed by the WHO Prevention of Blindness Committee which classifies causes both by the anatomical site affected and the timing of the insult leading to the visual defect and is aimed at highlighting preventable or treatable causes.14
Classification of underlying or associated causes of blindness and low vision (adapted from the WHO Prevention of Blindness Committee eye examination record14)
Size of the problem in the UK
INCIDENCE
There are few data on the incidence of childhood visual impairment in any region of the world3 4 6 including Britain. Most serious ophthalmic disorders in children which result in visual impairment are present or become manifest in early childhood. The new occurrence of serious bilateral visual loss in later childhood is uncommon by contrast with adults in whom the incidence of visual impairment is highest among those over 65 years.12 15 16
In England and Wales in 1990–91, the combined incidence of certification of partial sight and blindness was eight per 100 000 children aged 0 to 15 years.12 However serious underascertainment and imprecision of information on causes have been documented in this voluntary certification system.12 17The direct benefits of registration for a child differ to those for an adult, in particular there are no financial advantages and special educational needs can be assessed and met without registration. Consequently, in many cases there may be no additional real or perceived gain from registration of eligible children. Therefore, although registration data have traditionally been an important source of information, certification rates provide only general, minimum estimates of the incidence of severe visual impairment and blindness.
The Oxford Register of Early Childhood Impairments is a unique source of information about young children with early onset visual and other neurological impairments which uses multiple community and hospital sources to achieve high ascertainment. Between 1984 and 1991 the reported rate of visual loss (⩽ 6/18) was 1.4 per 1000 live births.18
During the same period in the 1984 Oxfordshire Health District Birth Cohort, the average annual incidence of presentation to a hospital eye clinic with ocular or vision disorders was 11 per 1000 in children under 2 years and 17 per 1000 in 2 to 5 year olds.19However many of these children had uncorrected refractive errors or ocular disorders without visual impairment. Consultation rates provide information on ocular morbidity which, while important in planning eye services, cannot provide estimates of the incidence of visual impairment in the population.
PREVALENCE
In many low income countries, about half the severely visually impaired and blind children die in childhood as a consequence of the blinding disorder or as a result of the disadvantages associated with visual handicap.4 By contrast, in Britain, only those visually impaired children with serious systemic disorders are at increased risk of dying in childhood. Therefore prevalence, dependent on both disease incidence and duration, is a useful measure of the burden of childhood visual impairment in Britain and is important in identifying groups at high risk and in assessing the impact of interventions.
The national prevalence of disability in children is not measured routinely in Britain. Two national surveys in 1985 and 1988 reported one or more specific disabilities in 36 per 1000 children aged under 16. A seeing disability (defined on the basis of vision dependent tasks rather than acuity) affected two per 1000 children overall and 6% of disabled children living in private homes and 16% of those in communal establishments.20 The 1958 and 1970 birth cohorts21 22 are the only large studies from which national estimates of the prevalence of visual impairment and its causes can be determined (table 3). The higher prevalence of partial sight and blindness in the later cohort may be due, among other factors, to differences in methodology or changes in survival patterns of children with multiple disabilities.
Prevalence of visual impairment and its main causes in England, Scotland, and Wales; results are prevalence per 1000 (95% confidence interval)
Prevalence estimates for a variety of different levels of visual impairment in other geographically defined populations in the British Isles are shown in table 4.23-25 The range of reported prevalence reflects varying case definitions, sources, methods, and completeness of ascertainment in these studies. This limits the scope for generating a summary estimate but it is probable that at least one child in a thousand in Britain is visually impaired, severely visually impaired, or blind (table 1). On-going studies of other defined populations, such as the ALSPAC cohort study,26 should provide information on incidence and causes of visual disability in the future.
Prevalence of visual impairment in the UK and Ireland
The long established Liverpool visual assessment team reported the prevalence of visual impairment in the context of other disabilities to be about twice that of isolated visual loss (⩽ 6/18 in either eye, table 4).25 Assessment of all children with serious visual loss by a district multidisciplinary team has been advocated recently27 but is not, as yet, available in all districts. Children with visual impairment which is less severe, isolated, or purely due to ocular disorders, may be managed principally or solely by the ophthalmic team and may be less readily identified in a community through systems primarily designed to ascertain children with multiple disabilities.
Causes of visual impairment in the UK
Both the anatomical and aetiological patterns of the causes of visual impairment and blindness in Britain have evolved with economic development and its attendant social, educational, and health care changes.28 Previously important preventable causes acquired in childhood, such as corneal infections, are now rare and prenatal and perinatal factors predominate. In a large proportion of cases, one or more relevant prenatal factors, such as hereditary disorders, maternal infections during pregnancy, and exposure to teratogens such as drugs, may be identified (table5).23 24 29 Perinatal factors, such as hypoxia, are especially important in low birthweight and preterm infants. In congenital disorders, such as microphthalmos, coloboma and anophthalmos, prenatal insults are implicated, although the specific cause may not be known. Further basic science and epidemiological research is required to elucidate disease mechanisms for these disorders.
Aetiology (%) of low vision and blindness in childhood in Britain
In Britain, the principal causes of serious visual loss are congenital cataract, cortical visual impairment, and optic atrophy28together with disorders of the retina and congenital ocular anomalies (table 3 and fig 1).18 23 29 Trauma is an important and preventable cause of ocular morbidity in children, being more common in boys, school age children, and in the setting of the home.30 However, ocular injuries are often unilateral and mild, so trauma rarely causes visual impairment.

Main causes of childhood visual impairment and blindness in children in the UK and Ireland.
The changes in the relative importance of different causes of blindness in newly registered children between 1969 and 1990 are shown in fig 2. The relative contributions of disorders of visual pathways, the inherited retinal dystrophies and albinism, congenital ocular anomalies, and retinopathy of prematurity have increased whilst cataract and optic atrophy have decreased. A similar pattern is seen in new registrations of partial sight.12 15 17 The interpretation of these time trends is difficult because they are influenced by changes in case ascertainment and registration practices as well as available treatment for and incidence of different disorders.

Traditionally registers of visual impairment and other national reporting systems have been the main sources of information on ophthalmic and vision disorders in children. However it is difficult to derive reliable estimates from single sources, particularly those dependent on routine collection of data. For example, in a recent national study,31 fewer than a quarter of infants with congenital cataract ascertained by active surveillance involving both paediatricians and ophthalmologists had been notified through existing national systems.
Children at higher risk of visual impairment
At least half of all visually impaired children have other disabilities20 23 24 25 and they are a special group for three reasons. Firstly, the impact of visual loss may be greater than in children without other disabilities, especially in hearing impaired children. Secondly, there may be a common underlying cause, such as hereditary disease or prenatal infection, and the recognition of such associations may be relevant to the diagnostic process. Thirdly, the prevalence and pattern of causes differ in children with other disabilities compared with those with isolated visual loss and this is relevant both to the management of individual cases and to policies aimed at early detection of ocular and vision defects.28
Nearly half of the children referred to the Liverpool visual assessment team with additional disorders had cortical visual impairment whereas 41% with isolated visual loss had inherited retinal dystrophies (fig3).25
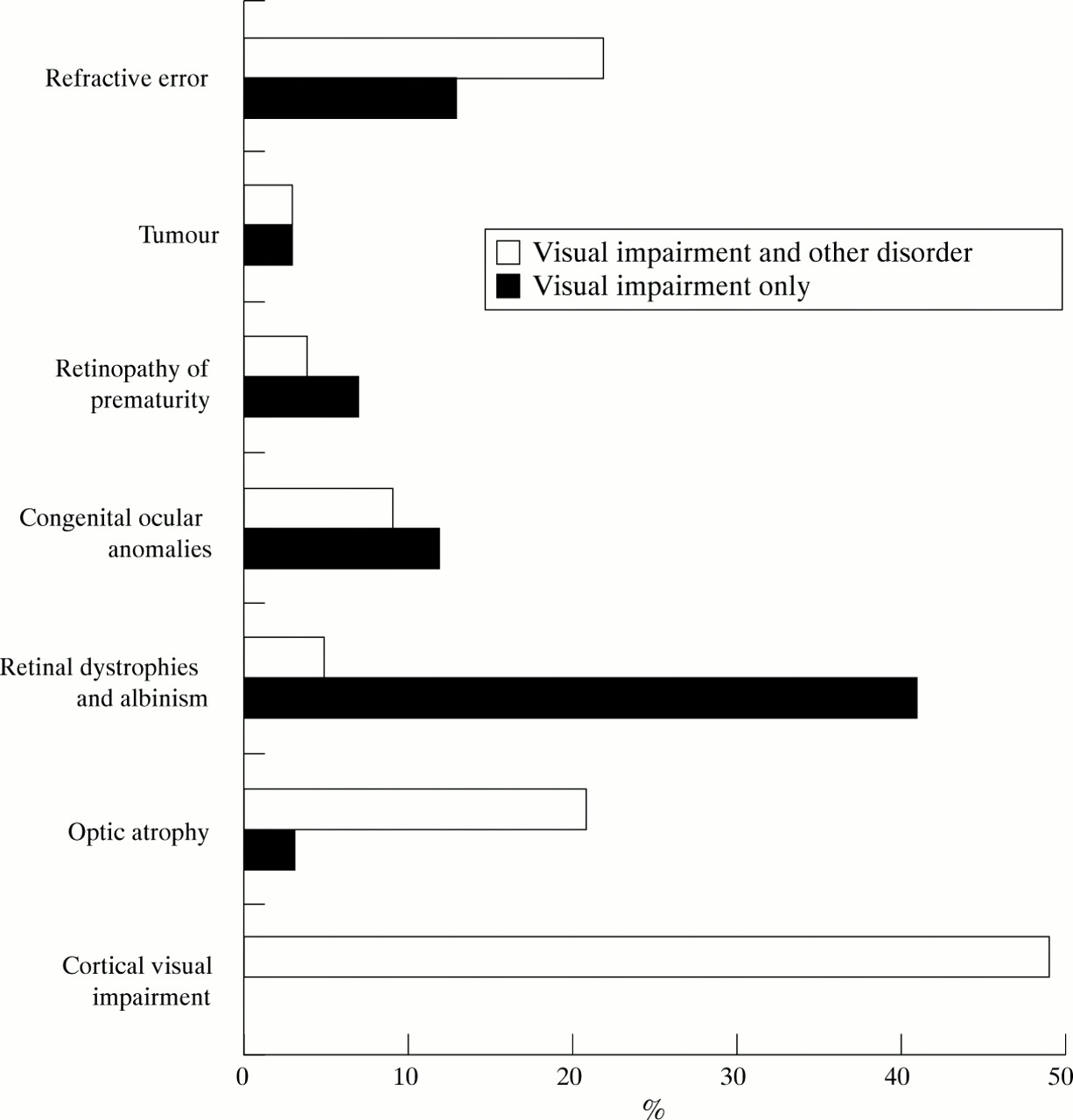
Main disorders among visually impaired children with and without other disabilities.25
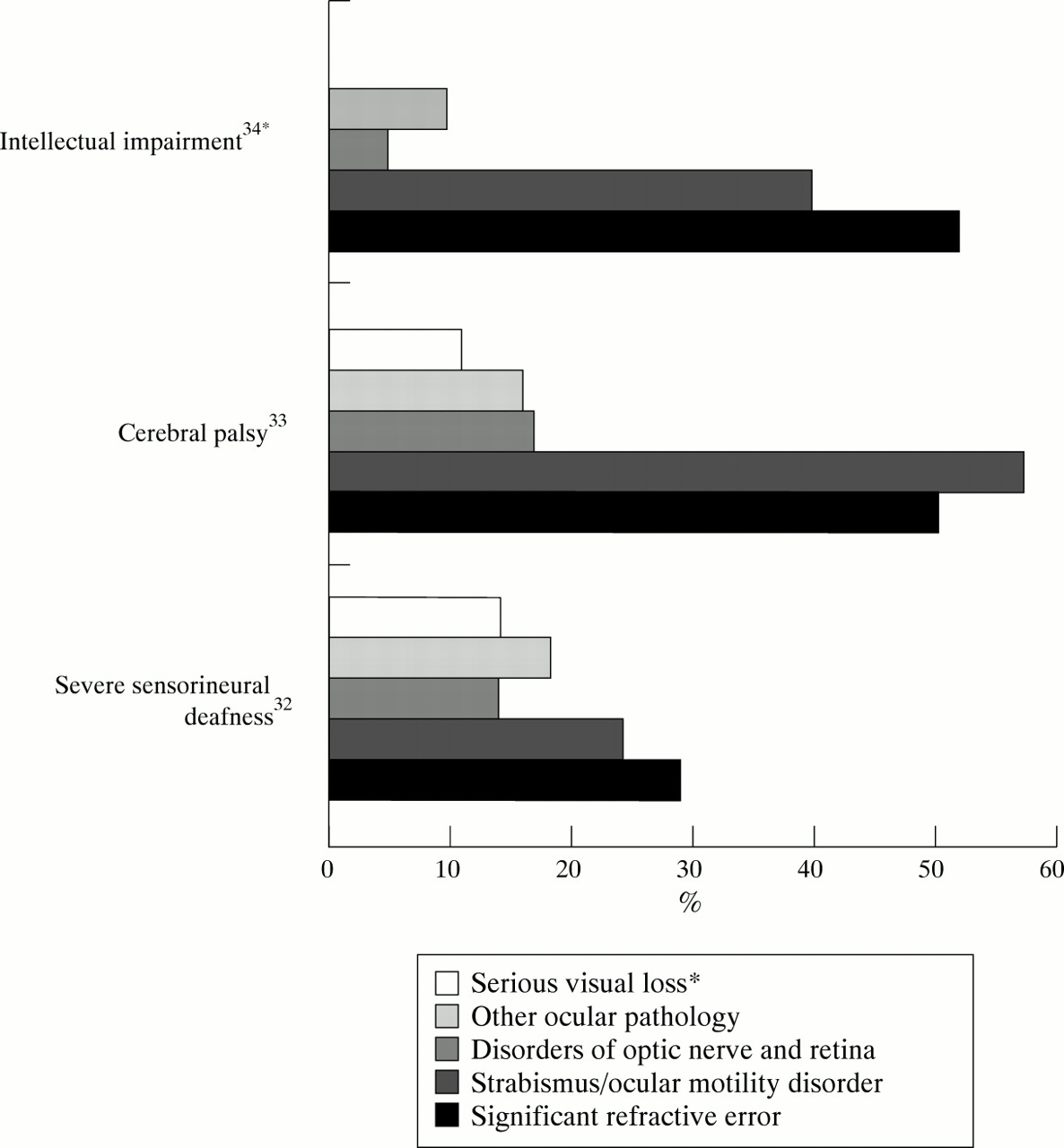
UK case series reporting ocular and vision defects in children with hearing impairment,32 cerebral palsy,33and intellectual impairment34 in the UK are shown in fig4. In Down’s syndrome high refractive errors, cataract, glaucoma, and strabismus occur more frequently than in the general population35 and may not be detected early without routine full ophthalmic assessment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ocular and vision defects in children with other disorders in Britain; * = visual loss not reported in intellectual impairment.
A variety of ocular and vision defects occur more frequently in children born preterm or of low birth weight,18 especially among those with neonatal periventricular haemorrhage or leucomalacia.36 Varying visual assessment techniques and duration of follow up have limited useful comparison of some reported studies of these children. A standard minimum dataset for follow up studies, including information on visual morbidity, has been advocated37 and would improve knowledge about visual outcomes in these children. The major ocular and vision defects in survivors of three cohorts of low birthweight and/or preterm infants are summarised in table 6.38-40
Ocular and vision defects in children born preterm or of low birth weight in Britain
Strategies to reduce childhood visual impairment in the UK
Up to 70% of childhood blindness worldwide is avoidable, that is, arising from causes which are entirely preventable or readily treatable.4 5 13 While the preventable fraction in the UK is likely to be much smaller, precise estimates would require better data on the incidence of different disorders and the distribution and importance of known risk factors. Furthermore the scope for primary prevention is limited by our present understanding of underlying mechanisms in disorders such as microphthalmos or idiopathic congenital cataract and by the availability of effective means of prenatal diagnosis of and early intervention for inherited disorders such as the retinal dystrophies. Nevertheless, there are a number of effective primary, secondary, and tertiary preventive strategies aimed at reducing visual impairment in the community. Some current and future strategies, together with examples of target disorders, are summarised in table 7. Their successful implementation requires a coordinated multidisciplinary approach involving geneticists, obstetricians, neonatologists, hospital and community paediatricians, as well as ophthalmologists and other ophthalmic professionals and those with expertise in the educational needs of the visually impaired.
Current and future strategies to prevent childhood visual impairment in Britain
Areas of future research
This review has highlighted some gaps in the epidemiological data regarding childhood visual impairment in Britain. Better information on the incidence, prevalence, and causes of visual impairment is required to inform and assess health, education, and social services for visually impaired children. The value of much of the currently available epidemiological information is limited by methodological difficulties as well as by the scope and completeness of routinely collected data. The further development and consistent use of standardised approaches to the classification of levels and causes of visual impairment are required together with more effective routine data systems for the collection of information on all children with visual loss in specified populations. Measures of disability associated with vision loss in children, including quality of life, are currently lacking but are particularly relevant to formal evaluation of different treatment options. Finally, there is a need for continued research to enhance understanding of human visual development, as well as natural history and causal pathways, if preventive strategies are to be strengthened and developed.
Conclusion
The prevention of childhood visual impairment in Britain poses an important challenge to clinicians and researchers alike. Effective secondary and tertiary preventive strategies exist and their successful implementation will continue to depend on coordinated services for affected children and their families. Further reduction in the burden of visual impairment will only be achieved by strengthening the scientific basis of primary preventive strategies.
Acknowledgments
Jugnoo Rahi is a Medical Research Council clinical training fellow; Carol Dezateux was supported by the Wellcome Trust.