Article Text

Statistics from Altmetric.com
How much cataract surgery do we have to do? When is enough enough? Around the world, this is a common question asked by governments, regional health authorities, health trusts, hospital managers, operating theatre staff, and ophthalmologists themselves.
These are fair questions. The volume of cataract surgery already has increased dramatically around the world over the past 20 years. It increased approximately fourfold in just 10 years in both the United States and Sweden through the 1980s1 2; and increased threefold in the United Kingdom over this time.3 In many areas cataract surgery now forms over half of all ophthalmic surgery, and in a number of countries cataract surgery has become the most common elective surgical procedure.4 5
There are three factors that influence the amount of cataract surgery that is performed in a community; the age structure of the community, the indications or thresholds that are used for surgery, and the proportion of those who need or are eligible for surgery who actually have surgery. These three factors combine to give the overall “cataract surgery rate” that has been defined by the World Health Organisation as the number of cataract operations performed per million population per year.6
We need to consider the importance and effect of each of these factors.
The single most important “risk factor” for cataract is increasing age. Data from the Visual Impairment Project in Australia are representative of data from other population based studies.7-10 They show that the prevalence of cataract increases dramatically after the fifth decade (40s). By the eighth decade (70s), half will have significant cataract and by the tenth decade (90s) everyone will be affected.11 Similarly, the proportion who have had cataract surgery doubles with each decade until every second person in their 90s will have had cataract surgery.
Age is clearly an important factor in determining the cataract surgery rate. In the next 20 years the population of the world will increase by about one third but the number over 65 years will more than double.6 This increase alone would double the amount of cataract surgery we, as the world's ophthalmologists, will have to do, even if everything else remained the same. However, everything else will not remain the same.
The second major factor in determining the cataract surgery rate is the indication or threshold used to determine whether an individual is suitable or eligible for cataract surgery. For generations the threshold was set as bilateral blindness. The quality of vision with aphakic correction did not justify earlier surgery. This threshold was turned on its head with the introduction of intraocular lenses (IOLs), first used 50 years ago. Modern IOLs provide excellent visual rehabilitation in almost every instance and the acuity threshold has tumbled from 6/60 to 6/24, then to 6/18 and is now often 6/9 or less.2 11-13 In addition, more attention is now paid to the functional impact of the lens opacities and the requirements of the patient as an individual. This has led to additional weight being given to the patient's perceived difficulties in their daily life and their visual needs.14 Questionnaires such as the VF-14 have been developed to specifically quantify this,12 but they still seem to be used more often in surgical audit or research activities than in routine clinical management.
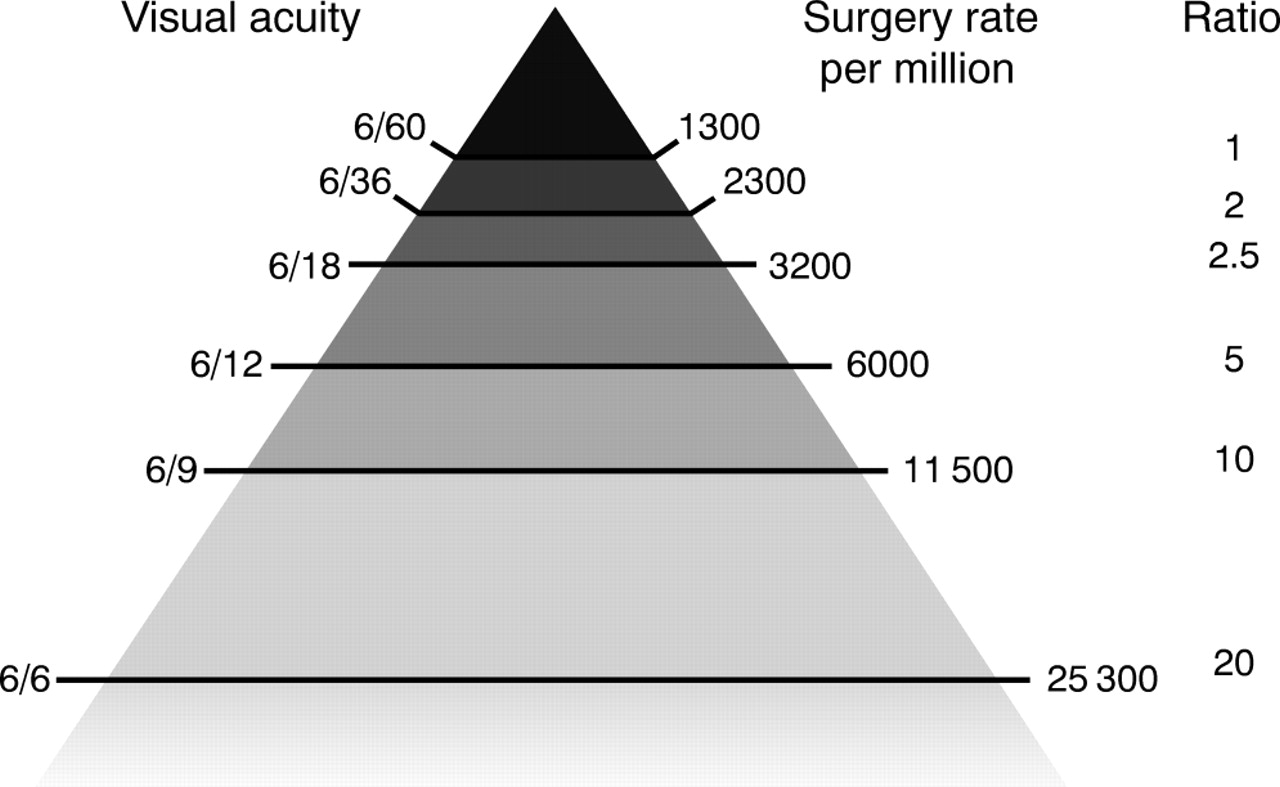
A change in threshold for cataract surgery can have a dramatic impact in the number of people who require surgery (Fig 1). The number of cataract operations increases 2.5 times as the acuity criterion changes from less than 6/60 to less than 6/24 and fivefold if it goes to less than 6/12. In many communities an acuity of less than 6/9 is regarded as the threshold for independent living as more and more elderly people depend on their ability to drive a car to be able to continue to live independently.15

{kind=link}
The golden triangle of ophthalmology; the relation between different thresholds of visual acuity and the cataract surgery rate. Data recorded from the Visual Impairment Project.11
There are obviously many forces that influence the threshold for cataract surgery. Consumer demand following the excellent rehabilitation obtained with modern IOL surgery, fee for service contracts, private practice, surgical performance incentives, and so forth will tend to push the threshold lower; limitations in budgets, resources, staff, theatre availability, etc, will tend to push the threshold higher and so reduce the number of procedures. Interestingly, the number of hospital beds used to limit the volume of cataract surgery that could be done. With modern day cases cataract surgery beds are no longer important and theatre availability has become the common “choke point”.
The third factor that determines cataract surgery rates is surgical coverage—that is, the proportion of those who actually have the surgery they need. This is a function of effectiveness of the healthcare delivery services in their community. Poor services that are inaccessible, inappropriate, or unaffordable will not be utilised and people with unoperated cataract will accumulate to form a surgical “backlog”. Globally, there are an estimated 20 million people blind (less than 3/60) from cataract and they form the world's cataract backlog.6 There are about 8 million cataract operations performed each year worldwide but there are about 10 million people newly added to the backlog. Most of the backlog occurs because of the lack of the appropriate cataract surgery services in the areas of need. The WHO, through its global initiative to eliminate avoidable blindness, Vision 2020, aims to increase the global volume of cataract surgery to 32 million per year by the year 2020 to meet these global needs.6 16 The target cataract surgery rate set by the WHO for established market economics for the year 2000 is 3500.
Another cause of a cataract backlog is rationing. Sometimes factors that lead to rationing can be quite subtle. Any factor that controls or sets the number of operations to be performed in a given time, at a number less than the demand, will lead to an ever increasing waiting list. These limiting factors are often fiscal and may be part of national policy. Inefficient or outdated work practices can also limit the number of operations performed in a unit of time. These types of factors may account for some of the regional variation seen in cataract surgery rates.17
Given all this, where do we stand? The report by Minassian and co-authors in this issue of the BJO (p 4) on cataract surgery in England and Wales is very sobering and shows that much needs to change. They have taken into account recent population based data from the North London Eye Study on the amount of cataract in the community, recent data on cataract surgery rates from the National Cataract Audit, and current demographic and mortality data for England and Wales. They show that at present, there is an estimated cataract backlog of 2.4 million people with visual impairment (<6/12) due to cataract and that there will be 1.1 million new cases in the next 5 years. To address this there were a total of 156 000 cataract operations performed in England and Wales in 1995–6 with 133 000 operations in those 65 years and older.
Given the current trends, Minassian and co-authors project an increase in volume of cataract surgery of 6.7% operations per year. At this rate the cataract backlog will actually increase by 8.5% in the next 5 years. Over the next 5 years, almost as many people (733 000) will come off the cataract backlog because they will have died as will have had cataract surgery (764 000)!
Minassian and co-authors suggest some strategies to help stop the backlog growing, but all require an increase in the number of cataract operations to be performed. But this would be just standing still and would maintain a backlog of 2.4 million people with visual impairment due to cataract. Surely the challenge for the UK is to eliminate the surgical backlog of cataract. This is the target set for the whole world by the WHO, albeit with a different threshold.
By way of comparison, the backlog of cataracts in Australia is estimated to be 30 000 and approximately 120 000 cataract operations were performed in 1999 for a population of 19 million; this gives a cataract surgery rate of 6300. The cataract surgery rate in the United States is about 5700 and about 4000 for Sweden,18 but it is only 2700 for the United Kingdom.
However one looks at them, the figures that Minassian and colleagues present are disturbing and they indicate that one way or another there still is a whole lot more cataract surgery to do.