Article Text

Statistics from Altmetric.com
Age related macular degeneration (AMD) is a degenerative disease usually occurring in people over the age of 50 years. Macular involvement can cause vision impairment and result in legal blindness due to atrophic or neovascular complications.1
The definition of specific lesions associated with AMD has led to classifications of the condition and its severity.1 The “dry” or non-neovascular form of AMD is characterised by drusen or abnormalities of the retinal pigment epithelium (RPE) such as atrophy, or hypopigmentation or hyperpigmentation. “Wet” or neovascular AMD is manifested by choroidal neovascularisation (CNV).2 The prevalence of non-neovascular AMD is greater than that of neovascular AMD. However, 10–20% of patients with non-neovascular AMD progress to neovascular AMD.34 Severe vision loss usually occurs when CNV extends under the centre of the foveal avascular zone (subfoveal CNV).5 Neovascular proliferation from the choriocapillaris extends through Bruch's membrane, invades the space under the RPE and leaks serous fluid, including lipid or blood, into this space.6 This neovascular process is associated with the development of fibrous tissue which replaces the normal architecture of the outer retina, often leading to severe, irreversible loss of central vision.7 Neovascular AMD, although present in less than 20% of all patients with AMD, is responsible for approximately 90% of cases with severe vision loss.8 It occurs in up to 200 000 individuals in the USA each year,9 with approximately 500 000 new cases throughout the world. Without treatment, most affected eyes have poor central vision (⩽20/200) within 2 years.10
The prevalence of AMD has been estimated in several epidemiological studies and ranges from 2% to over 10%, depending on the working definition of AMD, the grading system used, and the age and environment of the study population.3 All the studies, however, point to the association between AMD prevalence and age. AMD occurs most frequently in people above 50 years of age, with a strong increase in prevalence in people over 65 years of age.11-15 This rapid increase in AMD prevalence with age will probably pose a growing health problem for developed countries because of the increasing proportion of the population in older age groups. By 2020, as many as 7.5 million people over 65 years of age may suffer from vision loss due to AMD.16 Data from the UK have shown that the number of new registrations of blindness due to AMD has increased by 30–40% in the past 50 years.17
Untreated CNV secondary to AMD is usually associated with a poor vision outcome.10 The risk of severe visual acuity loss in untreated cases, for which photocoagulation would have been beneficial, can be at least twice that of cases treated with laser photocoagulation.5 However, photocoagulation is indicated in only a small proportion of cases.18-21 Until now, no effective treatment was available for most patients presenting with neovascular AMD.2223
Patients with CNV secondary to AMD in one eye are at high risk of severe vision loss in the fellow eye, which, when it occurs, will result in a significant adverse impact on the patient's quality of life. About 50% of patients presenting with bilateral CNV are legally blind within 5 years, compared with 12% of patients with unilateral CNV. In the latter group, however, CNV can develop in the fellow eye.24 Recent studies have also indicated that the prognosis of the fellow eye is strongly affected by four risk factors: three characteristics of the macula (presence of five or more drusen, focal hyperpigmentation, and one or more large drusen) and systemic hypertension.24 The 5 year incidence of CNV in the fellow eye has been estimated to be 87% in patients with all four factors, compared with 7% in patients with none of these risk factors.24 Thus, the four CNV risk factors are important for the identification of patients who are at risk of developing CNV in the fellow eye.
The ideal treatment for neovascular AMD should stabilise visual acuity or prevent the development of severe visual acuity loss, as well as preserve or limit the destruction of the retina overlying the choroidal neovascular lesion while destroying the pathological choroidal neovasculature. Such treatment would benefit most patients with CNV, without causing side effects, and would improve the patient's quality of life. Given the public health impact of neovascular AMD, many therapies are under investigation for this condition, leading to an explosion of information in this field. This paper reviews current and experimental treatments for neovascular AMD, focusing on the impact of verteporfin therapy (Visudyne; Novartis Ophtalmia, Bülach, Switzerland).
Treatments with proved benefits
LASER PHOTOCOAGULATION
Laser photocoagulation based on fluorescein angiography was the only treatment of proved efficacy for neovascular AMD in large scale, randomised clinical trials throughout the 1990s.25 The aim of laser photocoagulation is to treat the entire neovascular lesion in order to limit any subsequent destructive effects of CNV and therefore halt or slow the loss of visual acuity. Four important determinants in the use of laser photocoagulation are: visual acuity, CNV composition on fluorescein angiography, size of the entire choroidal neovascular lesion, and location of the lesion relative to the centre of the macula on fluorescein angiography. Laser photocoagulation has been shown to be beneficial in the treatment of CNV with well defined (well demarcated) boundaries not extending under the centre of the foveal avascular zone (extrafoveal or juxtafoveal CNV).26-28 Further, for CNV that extends under the centre of the foveal avascular zone (subfoveal CNV), not only should the lesion be well demarcated and include evidence of classic CNV, but its size should also be ⩽3.5 MPS (Macular Photocoagulation Study) disc areas for new lesions and ⩽6.0 MPS disc areas for recurrent lesions.529
Photocoagulation of subfoveal CNV, however, usually results in an immediate decrease of central vision,5 which may be delayed by perifoveal photocoagulation.30 The use of a thermal laser destroys overlying retinal tissue, which can lead to an immediate and irreversible loss of residual visual function.5 In addition, the inner choroid may be irreversibly damaged by this technique.
High rates of recurrence of CNV have been noted with laser photocoagulation. About 50% of laser treated eyes experience persistent or recurrent CNV within 3 years of treatment.28These recurrences usually lead to further deterioration in visual acuity.28 Apart from inadequate coverage of the area to be treated by laser photocoagulation or an inadequate level of energy used, recurrence may also be due to the fact that the underlying disease process continues and stimulates renewed neovascular growth.
It is estimated that only 10–20% of patients with neovascular AMD would benefit from laser photocoagulation that would reduce the risk of additional severe vision loss compared with no treatment.1831 This has led to the development and investigation of new modalities to treat neovascular AMD.
PHOTODYNAMIC THERAPY
Photodynamic therapy is a new treatment which has recently been proved in large scale, randomised clinical trials to reduce the risk of vision loss in selected cases of AMD with CNV that extend under the centre of the foveal avascular zone.32 Photodynamic therapy is a two step technique that can be performed as an outpatient procedure. The first step of the process involves an intravenous infusion of a light activated drug; the second step is activation of the drug by non-thermal light at a wavelength absorbed by the drug in the presence of oxygen.33 This probably results in the formation of cytotoxic oxygen species such as singlet oxygen and free radicals, which can damage cellular structures. This process may then lead to platelet activation and subsequent thrombosis and occlusion of new vessels within the treated area as well as destruction of fibrovascular tissue in the immediate vicinity of the new vessels.34
Numerous studies have found that light activated drugs can be retained preferentially in tumours35 and that photodynamic therapy leads to tumour death via occlusion of the tumour vasculature as well as a direct cytotoxic effect.36 These studies suggested that photodynamic therapy could be useful in the treatment of ocular diseases which are characterised by neovascularisation, such as AMD.
Several features of a light activated drug can affect its efficacy. Theselectivity of the drug can determine the degree of iatrogenic damage to diseased versus healthy tissue. An ideal selectivity for treating CNV would be a drug that causes damage only to the neovascularisation and not to any surrounding tissue. Theabsorption spectrum of the drug defines the optimum wavelength of the activating light and the depth of light penetration. A long wavelength of light may be able to penetrate through lens opacity in older people with AMD and penetrate through most of the retinal structures. The photosensitising potency of an agent determines the light dose required for optimum specificity—the greater the potency, the less thermal reaction caused by the light dose required. Thepharmacokinetic properties of the drug determine the timing of light administration and the period of risk of indiscriminate damage to the skin and eyes. Light activated drugs previously used in medicines such as haematoporphyrin derivative (HPD) and porfimer sodium (Photofrin, Axcan Pharma Inc) were limited by a weak photosensitising potency and production of prolonged skin photosensitivity lasting up to 12 weeks.33 Ideally, to minimise the time taken to treat a patient, these pharmacokinetic properties should allow a brief time between administration of the drug and light application for activation. In addition, the time in which indiscriminate damage to the skin and eyes might occur is decreased if a drug clears rapidly from the body.
The advantages of photodynamic therapy include that it is selective in affecting choroidal neovascular tissue with minimal damage of the photoreceptors overlying the neovascular tissue that are viable at the time of treatment. Therefore, photodynamic therapy may lead to destruction of CNV, thus preventing further damage that would lead to impairment of visual acuity. This technique may even be able to improve visual acuity in some cases, where part of the decreased vision is caused by subretinal fluid or haemorrhage which could clear with destruction of the neovascular tissue.3738
VERTEPORFIN
Verteporfin (benzoporphyrin derivative monoacid, BPD-MA, Visudyne) is a new potent second generation light activated drug for photodynamic therapy, which is derived from porphyrin and consists of two regioisomers.39 It is lipophilic and is taken up by plasma membrane cells.40 It is under investigation for potential use in the treatment of a variety of conditions including skin cancer, psoriasis, and the neovascular form of AMD. Verteporfin therapy has been shown to cause little damage to physiological intraocular tissues when used at a proper drug dose, dye dose, and timing of photoactivation.41
Features of verteporfin
Verteporfin is injected intravenously as a liposomal preparation to provide solubility and to increase selectivity. Once in the circulation, verteporfin partitions into lipoproteins and complexes with low density lipoprotein (LDL). In vitro studies suggest that cellular uptake of verteporfin–LDL complexes is mediated by LDL receptors.40 These receptors are expressed on endothelial cells, and their expression is increased in neovasculature,3842 thus leading to an increase in LDL uptake.43 This mechanism may explain, in part, the preferential accumulation of verteporfin in neovascular tissues, which leads to an increased selectivity of the photodynamic therapy effects of verteporfin on CNV and not on other retinal vessels that overlie the CNV.4042-46
Following intravenous injection, verteporfin can accumulate rapidly in the choroid, RPE and photoreceptors of the rabbit eye.4748 Because verteporfin has a long absorption wavelength with a peak at 689 nm, light that activates the drug may be able to penetrate more deeply into outer retinal tissues than the wavelength of light that is required to activate HPD.49Verteporfin is cleared rapidly from the body within the first 24 hours. In addition, it appears to be cleared from the choroid, RPE, and retina faster than HPD,47 so these structures are photosensitive for a shorter time. Verteporfin is no longer detected in the outer retina 2 hours after injection, whereas HPD is detectable 48 hours after injection.47 Light exposure after 24 hours appears to induce only a minimal skin photosensitivity reaction in mice.50 When injected intravenously, verteporfin has a plasma half life of 2–5 hours in different species (QLT Inc, unpublished data, 1996).
Preclinical studies
Preclinical studies have shown that verteporfin is effective in treating experimental choroidal melanomas,45 in causing vascular occlusion in a rabbit choroid without damage to the neuroretinal or the basement membrane of the RPE,49 in producing occlusion of experimental CNV,5152 and in inducing cessation of leakage from CNV induced after laser injury to monkeys.5152 Repeated treatments with verteporfin in normal monkey eyes demonstrated dose dependent recovery of the capillaries with minimal damage to photoreceptors.53 All these findings suggested that verteporfin therapy should be evaluated for the treatment of CNV in humans, and helped to define the range of treatment parameters that could potentially be used in clinical trials.
Phase I/II studies
A phase I/II investigation was designed to evaluate the safety and maximum tolerated doses of verteporfin therapy for the treatment of patients with CNV. These studies were also designed to determine if fluorescein dye leakage from CNV could be stopped by verteporfin therapy without visual acuity loss, on the assumption that cessation of leakage might stop lesion growth and prevent further vision loss.54-56 In a report on single treatments, the results showed that light activated verteporfin could cause short term (1–4 weeks) cessation of fluorescein leakage from CNV without angiographic damage to retinal blood vessels or loss of vision.54 The data showed that the maximum tolerated light dose was less than 150 J/cm2 (above this, loss of selectivity with retinal vascular occlusion occurred). A light dose of 25 J/cm2 was reported to be the minimum dose at which an effect on fluorescein leakage could be produced. In almost all cases, fluorescein leakage recurred by 12 weeks after the initial treatment, even in patients who had received a maximum tolerated light dose. The investigators believed that it was highly probable that fluorescein leakage 12 weeks after an initial treatment would result in continued growth of the neovascular lesion, accompanied by progressive vision loss. Multiple treatments using verteporfin therapy to stop fluorescein leakage from CNV were therefore evaluated to determine whether this would prevent the progressive growth of the neovascular lesion and any vision loss associated with this growth.55 Repeated treatments consistently caused short term cessation of fluorescein leakage from CNV without causing angiographic damage to the retinal blood vessels or short term visual acuity loss.55 Nevertheless, return of leakage from CNV was typically noted by 12 weeks after a retreatment (although often involving an area smaller than that noted before treatment), suggesting that periodic treatment for an indeterminate length of time might be required in future evaluations of verteporfin therapy for CNV.
Systemic safety of verteporfin was very good in this phase I/II investigation. Specifically, the most frequent adverse event of this open label study was headache (4.7%), while other adverse events occurred in less than 4% of patients, with no skin photosensitivity reported.54-56
The results from the phase I/II studies suggested that a potentially effective dose of verteporfin to be considered for phase III trials would be 6 mg/m2 body surface area, which would be infused intravenously over 10 minutes.5455 Irradiation with a diode laser at 689 nm was applied 15 minutes after the start of the infusion; the light dose delivered was between 50 and 100 J/cm2 at an intensity of 600 mW/cm2 over a period of 83 seconds. This regimen had the greatest number of eyes with absence of fluorescein leakage from classic CNV 12 weeks after initial treatment (30%; three of 10 patients), and 36% (four of 11 patients) gained three or more lines of vision with this treatment with short term follow up. The 50 J/cm2 light dose in this regimen was associated with the highest percentage of patients with absence of leakage at 4 weeks (57%) and the lowest percentage of patients with progression of classic CNV at 12 weeks. These and other factors led to the selection of this regimen for future trials.
Phase III studies
Two phase III trials were begun in December 1996, termed the Treatment of Age related macular degeneration with Photodynamic therapy (TAP) investigation in Europe and North America. The objective of the TAP investigation was to determine whether verteporfin therapy, compared with placebo, could reduce the risk of vision loss in eyes with subfoveal CNV secondary to AMD.32 A total of 609 participants were randomly assigned (2:1) to verteporfin or placebo. All patients and treating ophthalmologists were masked to the treatment assignment, as were the visual acuity examiners and photograph graders. The key eligibility criteria for inclusion were a best corrected visual acuity of approximately 20/40 to 20/200, subfoveal CNV secondary to AMD with evidence of classic CNV, and a greatest linear dimension (GLD) of the entire lesion on the retina of 5400 μm or less.
The treatment spot size was determined after measuring the GLD of the entire lesion with a millimetre ruler placed on the fluorescein angiogram, in which the angiographic image was magnified 2.5 times. Dividing the GLD by 2.5 resulted in the approximate GLD of the lesion on the retina. An additional 1000 μm was added to this dimension to provide a 500 μm margin of additional treatment to ensure that the entire CNV would be treated and to compensate for any slight movements of the study eye during light application (Fig 1). The laser parameters were set up to deliver this spot size onto the retina, taking into account the magnification of the contact lens to be used during light application. Because the dose of verteporfin depended on the patient's body surface area, the height and weight of the patient had to be determined on the day of treatment. A 30 ml solution of either placebo (5% dextrose in water) or verteporfin (6 mg/m2 body surface) was prepared and this was infused into the patient over 10 minutes; then, 15 minutes after the start of the drug infusion, light was applied for 83 seconds.

The spot size of the light used to activate verteporfin is calculated by measuring the greatest linear dimension (GLD) of the lesion on the retina from the fluorescein angiogram, adding 1000 μm to ensure a sufficient margin to cover the whole lesion. (Reproduced with permission from Treatment of Age-related Macular Degeneration With Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularisation in age related macular degeneration with verteporfin. Arch Ophthalmol 1999; 117 :1329–45.)
Patients were scheduled to return approximately 3 months after each evaluation (within 2 weeks before or after that date). Retreatment could be considered if there was no serious adverse event judged to be associated with any previous photodynamic therapy. Retreatment with placebo or verteporfin (as assigned at the baseline examination) was administered to the patient if the treating ophthalmologist noted any leakage from any CNV (classic or occult) on a fluorescein angiogram taken every 3 months after the initial or subsequent follow up examination for up to 2 years. The treatment parameters were similar to those at baseline, except that the treatment spot size (GLD + 1000 μm) had to span all areas of leakage from classic or occult CNV (even if these areas were non-contiguous), as well as any hypofluorescence from blood or a fibrovascular pigment epithelium contiguous to CNV. The lesion to be retreated did not include any scar tissue that stained (but did not leak fluorescein from its boundaries), or hyperfluorescence that was not from visible blood. In cases where the GLD to be retreated exceeded the maximum spot size (approximately 6000 μm during the TAP investigation), the treating ophthalmologist positioned the spot to encompass as much of the area of leakage as possible.32
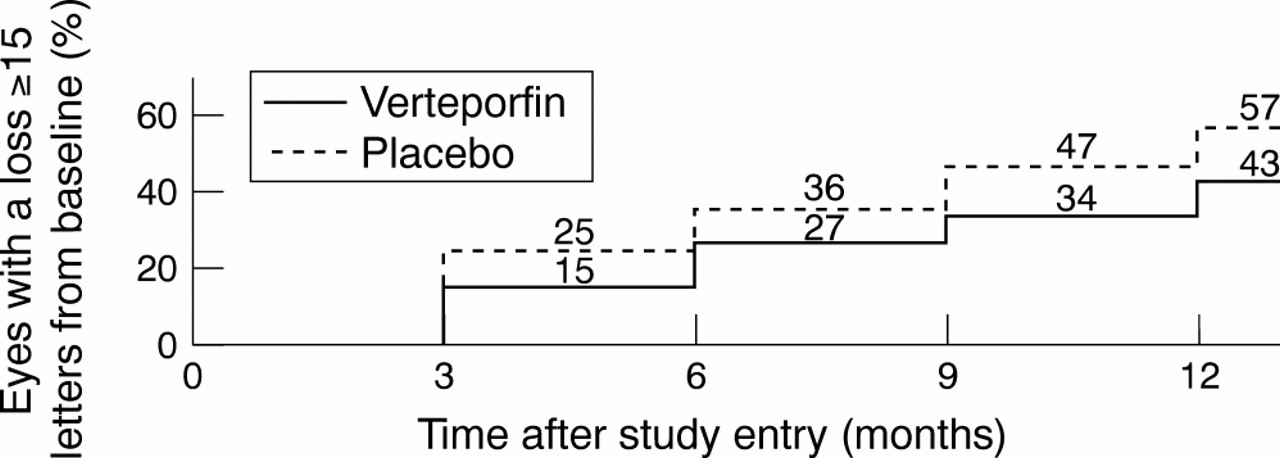
Ninety four per cent of each group completed a follow up examination at 12 months. The proportion of verteporfin treated patients who required retreatment decreased with each follow up visit (91% at month 3, 79% at month 6, 70% at month 9, and 64% at month 12). The proportion of eyes with at least moderate vision loss (a decrease in the letter score of ⩾15 letters or approximately ⩾3 lines) was greater in placebo treated eyes than in verteporfin treated eyes throughout the period from examination at month 3 to the examination at month 12 (Fig 2). These visual acuity benefits were supported by numerous other outcomes. For example, the proportion of eyes with severe vision loss (a decrease in the letter score of ⩾30 letters or approximately ⩾6 lines) was greater in the placebo treated group than in the verteporfin treated group throughout this follow up. Verteporfin treated eyes were more likely to have a visual acuity better than 20/200 at month 12, and the mean number of contrast sensitivity letters lost was almost zero in the verteporfin treated eyes compared with about five letters in the placebo treated eyes.

Kaplan–Meier estimates of the cumulative proportion of eyes treated with verteporfin or given placebo with moderate visual acuity loss (⩾15 letters or approximately ⩾3 lines) at each 3 month study visit over time during the first 12 months of the TAP investigation. (Reproduced with permission from Treatment of Age-related Macular Degeneration With Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularisation in age related macular degeneration with verteporfin. Arch Ophthalmol 1999; 117 :1329–45.)
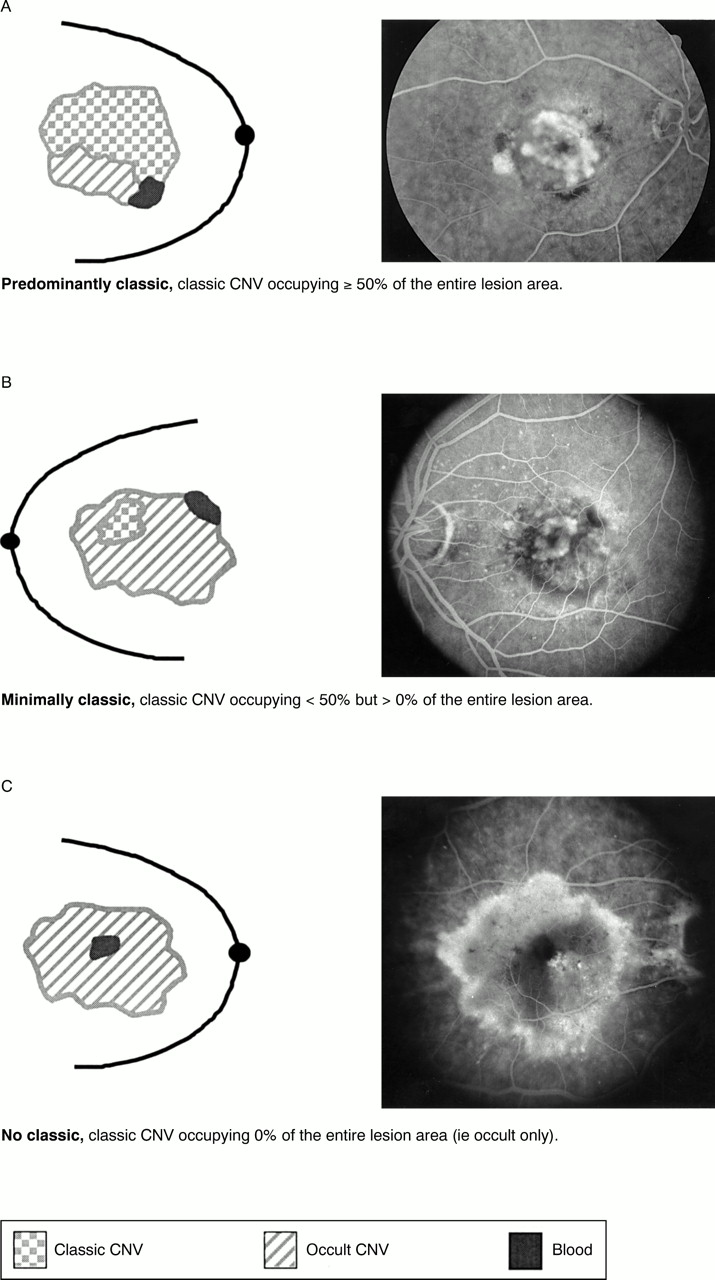
In subgroup analysis based on the gradings of all fluorescein angiograms at a central photograph reading centre (Fig 3), the visual acuity benefit of verteporfin therapy was clearly demonstrated in eyes with classic CNV occupying at least 50% of the area of the entire lesion (termed “predominantly classic” lesions). With respect to predominantly classic lesions, 33% of the verteporfin treated eyes had at least moderate vision loss at 12 months compared with 60% of the placebo treated eyes (Fig 4). Furthermore, at this time, 12% of verteporfin treated eyes and 33% of placebo treated eyes had severe vision loss.32

Schematic representations of mid phase angiographic examples of baseline lesion composition for a predominantly classic lesion (A), minimally classic lesion (B), and no classic, or occult only, lesion (C).

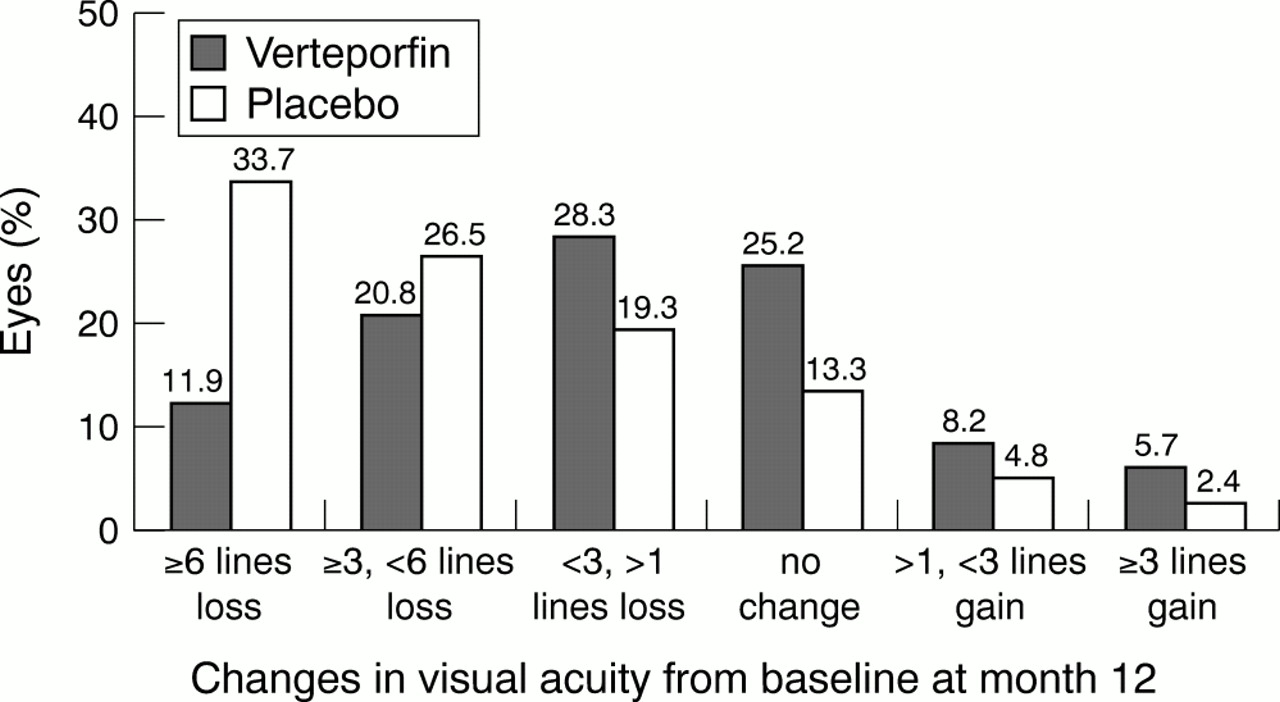
Distribution of changes in visual acuity from baseline at the month 12 examination of the TAP investigation for eyes with predominantly classic lesions.
The results were even greater for predominantly classic lesionsand no occultCNV; 23% of verteporfin treated eyes had at least moderate vision loss at 12 months compared with 73% of placebo treated eyes. Ten per cent of the verteporfin treated eyes had severe vision loss compared with 41% of the placebo treated eyes. These results prompted the TAP Study Group to recommend verteporfin therapy for all predominantly classic lesions that met the eligibility criteria for the studies.
No statistically significant difference in visual acuity was noted when the area of classic CNV was greater than 0% but less than 50% of the area of the entire lesion (termed “minimally classic” CNV). There was a difference in favour of the verteporfin treated patients in the subgroup of lesions enrolled with no classic CNV. However, these cases should not have been enrolled because there was no evidence of classic CNV. Also, the number of patients in this subgroup was small: 37 patients treated with verteporfin and 19 patients given placebo had a follow up at month 12. Therefore, no recommendation could be made at this time regarding treatment for this subgroup. These findings underscore the importance of identifying occult CNV, which is facilitated by stereoscopic frames and images obtained 5 and 10 minutes after fluorescein injection. Failure to recognise some occult CNV may result in overestimating the proportion of the lesion which is classic CNV or underestimating the GLD of the lesion and the spot size of the laser.
Several angiographic outcomes were consistent with the visual acuity outcomes. Progression of classic CNV beyond the area of the lesion identified at baseline occurred in only 166 (46%) of 361 verteporfin treated eyes compared with 133 (71%) of 187 placebo treated eyes by the month 12 examination. Placebo treated lesions were almost twice as likely (73%) to be greater than 6 MPS disc areas in size than verteporfin treated lesions (40%), even though most lesions in both groups were less than 6 MPS disc areas in size at baseline. Fluorescein leakage was absent from classic CNV in 68 (19%) of the verteporfin treated eyes compared with 17 (9%) of the placebo treated eyes. No major differences in angiographic outcomes of occult CNV were noted between the verteporfin and placebo groups. These results suggest that verteporfin therapy reduces lesion growth, is associated with cessation of leakage from classic CNV, and decreases the likelihood of progression from classic CNV. Angiographic outcomes appeared to be better for lesions treated with verteporfin that had minimally classic CNV, even though a visual acuity benefit was not noted in this subgroup. This finding suggests that angiographic outcome cannot be used as the only surrogate outcome for the visual acuity benefits of verteporfin therapy for CNV in AMD.
Few ocular systemic adverse events judged to be of any clinical relevance were noted. Compared with placebo patients, verteporfin treated patients had more transient vision disturbances (18%v 12%), injection site adverse events (13%v 3%), transient photosensitivity reactions (3% v 0%), and infusion related low back pain (2% v 0%). However, most of these events were mild to moderate, and discontinuation of treatment was rarely (<2% of the time) requested by the ophthalmologist or study participant or both. These findings suggest that patients should be warned of mild, transient visual disturbances and that they need to return for follow up soon after treatment only if severe vision loss is noted. Infusion should be to the antecubital veins, whenever possible, to reduce risk of extravasation. If extravasation occurs in the antecubital fossa, it can be easily covered with long sleeved clothing. Furthermore, patients should realise that, although back pain may rarely occur during infusion, it causes no known long term problem and should be relieved as the infusion ends. Finally, avoiding direct sunlight or bright indoor light for the first 48 hours after treatment is probably sufficient if there is no extravasation.
In summary, the TAP investigation showed that verteporfin therapy reduced the risk of at least moderate vision loss compared with placebo for at least 12 months in patients with predominantly classic CNV who presented with subfoveal lesions. In the TAP investigation, the visual acuity results were complemented by similar outcomes for contrast sensitivity evaluations.
Recent reports suggest that the overall beneficial outcomes noted in the TAP investigation at 12 months remained the same at follow up examinations up to 24 months, with 41% of verteporfin treated eyes compared with 69% of placebo treated eyes having at least moderate visual acuity loss at the month 24 examination for predominantly classic lesions. Thus, the 2 year results provide further support to recommend verteporfin therapy in the management of patients with predominantly classic subfoveal CNV due to AMD.
Other treatments currently under investigation
The following treatments are still under investigation; no proved benefit has yet been demonstrated in large scale randomised clinical trials.
REFINEMENTS OF PHOTOCOAGULATION
Many patients with neovascular AMD probably present with occult CNV without classic CNV.18 In the past few years, a number of therapeutic techniques have been investigated for this type of CNV, but none has shown convincing evidence of efficacy.
Improvement in diagnosis
CNV often has poorly defined boundaries on fluorescein angiography. Indocyanine green (ICG) angiography may improve the visualisation of these lesions. Accurate delineation and localisation with ICG angiography can allow some of these lesions to be superimposed over a red-free photograph or on early phase fluorescein angiograms. This approach may result in ICG guided laser photocoagulation treatment of lesions with poor definition on fluorescein angiography that are well defined and do not involve the fovea on ICG angiography. These lesions would not be eligible for treatment under MPS guidelines; thus, a combination of fluorescein and ICG angiography might allow more eyes with CNV due to AMD to be treated.
The results from a limited number of small, uncontrolled studies evaluating laser photocoagulation guided by ICG angiography have shown that there is complete resolution of fluid and other clinical manifestations of CNV in some eyes with occult CNV. Furthermore, some of these eyes showed improvement or stabilisation of visual acuity. Similar results have been obtained for laser photocoagulation of focal spots at the edge of plaques of subfoveal occult CNV.57The same approach has been considered for CNV associated with RPE detachment. In one pilot study, ICG guided laser photocoagulation temporarily stabilised visual acuity in some eyes but final visual acuity decreased with time.58 These results should be compared with the natural history outcomes of these lesions to establish if they differ from those seen without treatment.59
Because of the light absorption peak of the ICG dye, some authors considered the use of ICG enhanced diode laser photocoagulation. This approach was thought to permit a selective removal of ICG stained CNV with relative sparing of the neighbouring neurosensory retina. Limited groups of patients showed potential benefits in small, uncontrolled studies.60 However, little difference was demonstrated between ICG enhanced and non-enhanced mild diode laser burns and thus this approach has still to demonstrate its efficacy.
Some investigators have claimed that other approaches based on ICG angiography are successful. Various techniques using either dynamic or high speed videoangiography have been used to visualise extrafoveal feeder vessels of subfoveal CNV that would not benefit from laser photocoagulation. These techniques have been used in conjunction with fluorescein angiography, but results were not reproducible because it was not always possible to distinguish arterial and venous feeder vessels. With very early phase ICG angiography, arterial feeder vessels can be distinguished from the draining veins. Photocoagulation of the feeder vessels is performed with argon green laser61 (Fig5), dye laser,62 or diode or micropulse diode laser. According to the results of small, uncontrolled studies this technique based on ICG angiography may decrease fluid and thus allow improvement in visual acuity.

ICG guided feeder vessel photocoagulation. Very early phase ICG angiography at presentation (A) of patient with subfoveal occult CNV and visual acuity of 20/40. The early photographs show a horizontal choroidal vessel (arrow), intensely hyperfluorescent at the arterial choroidal phase, located in the superotemporal part of the posterior pole, outside of the foveal avascular zone. This vessel was considered to be the arterial feeder vessel of the CNV because it was only perfused for 3 seconds of the arterial phase, and was no longer visible thereafter. Furthermore, its perfusion was pulsatile, and its flow was in the opposite direction to that in the normal choroidal artery. The vessels below the feeding vessel were filling subsequently. Early phase of ICG angiography (B) immediately after focal laser photocoagulation of the feeder vessel shows hypofluorescence of the laser treated area superotemporal to the hypofluorescence of the neovascular lesion of the feeder vessel identified.
Improvement in photocoagulation techniques
The destruction of the neurosensory retina overlying the CNV has always been a concern with laser photocoagulation. In order to minimise the destruction, and even spare the photoreceptors, selective photocoagulation has been attempted. Multiple short argon laser pulses of a green Nd:YLF laser63 or repetitive short micropulses of a diode laser (710 nm) have been shown histologically to reduce damage to the photoreceptors and to allow the replacement of the original RPE by a monolayer of new RPE cells. In addition, a minimal inflammatory response was observed with these techniques. This approach for the treatment of macular diseases is at present under evaluation in small, uncontrolled studies.64
Transpupillary thermotherapy
Transpupillary thermotherapy is a technique by which heat is delivered to the choroid and RPE using a diode laser at 810 nm. This therapy has been reported to be effective for choroidal melanomas.65 The goal in using this technique for treatment of CNV is to achieve occlusion of the neovascularisation without damage to other cells. Heat penetration is optimised by exposure time, beam diameter, and wavelength. In addition, inner retinal effects produced by coagulation are absent, thus optimising the penetration of the light. Transpupillary thermotherapy may also minimise collateral damage to the adjacent normal retina due to delivery of decreased thermal energy.
A retrospective study with a limited number of cases and limited follow up without controls evaluated 16 eyes presenting with subfoveal occult CNV on fluorescein angiography.66 The spot size was adapted to the size of the CNV, and the power ranged between 360 and 1000 mW for 60 seconds. The end point was an area of no visible colour change to a light grey appearance of the level of the pigment epithelium. In this study, visual acuity remained stable in nine eyes (56%), while three eyes (19%) showed two lines of improvement, and four eyes (25%) a decrease of two lines or more during a mean follow up period of 12 months. The authors reported that most eyes (94%) demonstrated a decreased exudation on clinical examination, fluorescein angiography, and optical coherence tomography. The value of this therapeutic approach would require comparison with controls in randomised clinical trials.
SUBMACULAR SURGERY
A variety of surgical techniques have been investigated for the treatment of subfoveal CNV secondary to AMD. The risks and benefits, which still remain imprecise, are under investigation in the USA in randomised clinical trials sponsored by the National Eye Institute of the National Institutes of Health.67 These trials include eyes with subretinal haemorrhage that is too extensive to allow laser photocoagulation or photodynamic therapy, as well as eyes with some classic CNV (but not necessarily predominantly classic lesions) and an initial visual acuity of 20/100 to 20/800.
Removal of CNV by submacular surgery is through a small retinotomy and may therefore minimise injury to the overlying photoreceptors.68 However, histological examination shows that CNV removed by this technique often contains photoreceptors and RPE cells, and thus explains why submacular surgery in AMD usually results in a central scotoma.69-72 Retinal detachment or postoperative cataract may also occur secondary to this surgical procedure.69
Most studies investigating submacular surgery have shown that submacular excision of CNV does not improve mean vision in patients with AMD.6973 In the largest prospective study in patients undergoing excision of subfoveal CNV, mean visual acuity 12 months after surgery was 20/320 with a mean loss in visual acuity of one line compared with baseline.74 As with laser photocoagulation, recurrence of CNV may be common following submacular surgery, as suggested by the results of Thomas et al, showing a recurrence rate of 46% in eyes that were followed up for a period of 12 months or more.75 The reasons for poor vision outcomes after submacular surgery potentially include irreversible damage to the photoreceptors or RPE, caused either by the subfoveal CNV or by partial removal of these structures by the surgical technique, and retinal damage mediated by subretinal fibrin.73 The use of tissue plasminogen activator before CNV excision did not provide any vision or anatomical benefit in a randomised double masked trial.74
Despite these limitations, submacular surgery may increase the chance for stable or slightly improved vision in selected patients with new subfoveal lesions with evidence of classic CNV that otherwise might progress to a large amount of vision loss if left untreated. This is being investigated in a randomised clinical trial, (Group N Protocol) Submacular Surgery Trials (SST) sponsored by the National Eye Institute.67 Submacular surgery also might be beneficial compared with no surgery for patients who present with large submacular haemorrhages due to CNV in which the large amount of blood precludes use of laser for photocoagulation or photodynamic therapy. This is being investigated in another SST protocol, Group B. Both protocols are designed to study whether submacular surgery would increase the likelihood of vision stabilisation or improvement, compared with no surgery. These studies are ongoing, and no results have yet been published.
OTHER SURGICAL TECHNIQUES
Other surgical techniques include RPE transplantation and macular translocation of subfoveal classic CNV. Macular translocation has been developed to rotate the retina and therefore move the foveal region away from the CNV.76-79 After a 360º retinotomy, improvement in distance vision was obtained in only 10% of the patients in published reports—about half of these patients experienced an improvement in reading vision.7778 Postoperative complications with this technique include the development of retinal detachment, macular pucker, increased lens opacity in the phakic eyes, and disorienting side effects of diplopia and tilted image that might be managed with muscle surgery.7778 A potentially less damaging technique consists of performing a shortening of the sclera combined with a retinal detachment allowing a more limited (1–2 mm) translocation of the macula.79 The application of laser photocoagulation, after macular translocation, to the CNV that is no longer subfoveal may avoid subsequent immediate vision loss (Fig6).79 Published reports of this technique has only been investigated in a small number of patients. The results from the first three patients indicated vision improvement in about 40–60% of the eyes. Translocation of the RPE, from the edge of the RPE defect to a subfoveal location, following submacular removal of CNV, has also been suggested recently as a new approach to the surgical management of neovascular AMD.80

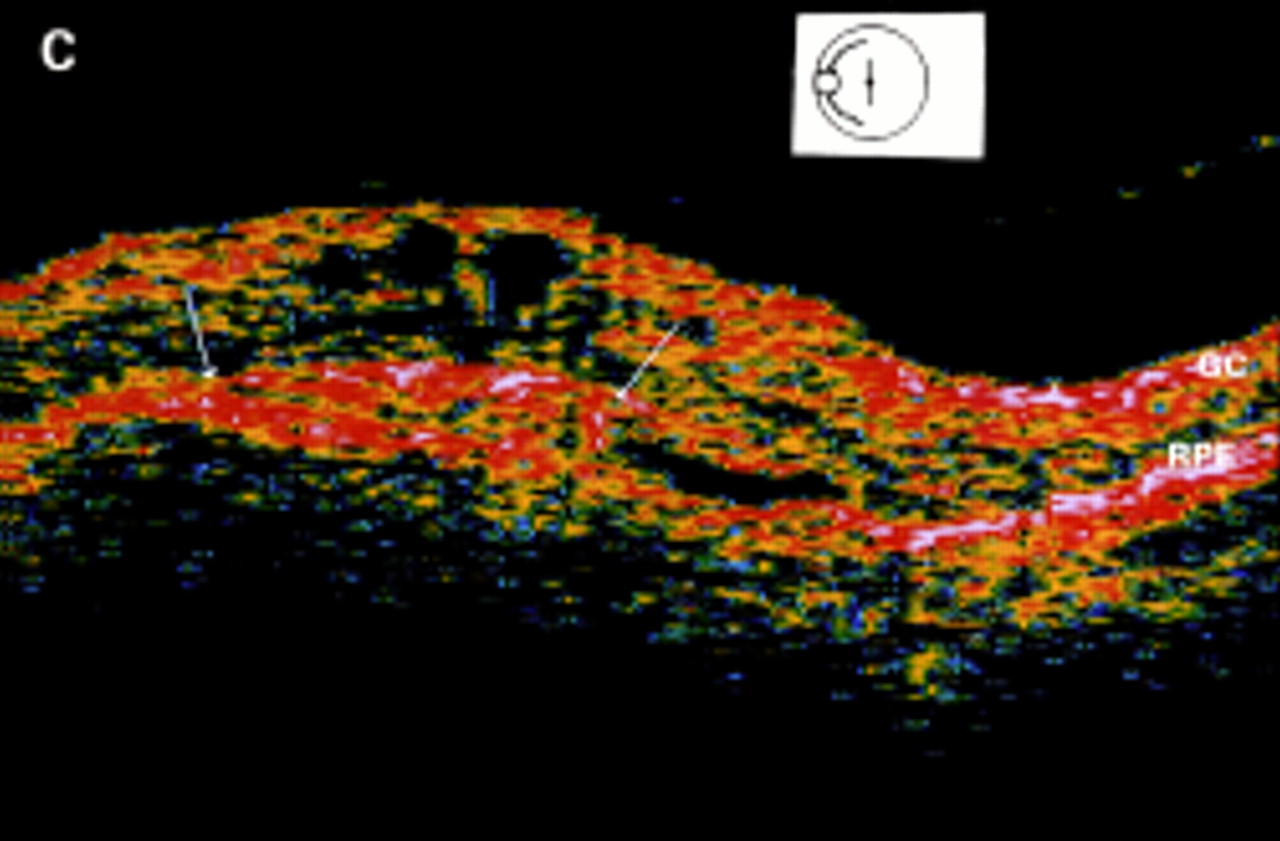
Limited foveal translocation. Fluorescein angiography at presentation (A) shows a small well defined foveal lesion involving the entire avascular zone. ICG angiography (B) discloses the subfoveal classic lesion in the same location as fluorescein angiography. OCT imaging (C) shows the normal hyperreflectivity of the ganglion cell layer in the inner retina (GC) and of the outer complex of retinal pigment epithelium, Bruch's membrane, and choriocapillaris (RPE). This later hyperreflectivity is a continuous layer, but a mushroom outgrowth is extending into the neurosensory retina (arrows). This aspect appears to correspond to the well defined choroidal lesion. ICG angiography (D) performed after surgically limited translocation and photocoagulation of the classic CNV shows that the laser treated area now lies next to the superotemporal retinal artery, outside of the fovea which is located away from the photocoagulated area (circle).
RPE transplantation might be used after removal of subfoveal CNV to replace destroyed or degenerated RPE to improve visual function.81 This therapeutic approach started as a form of intraocular grafting performed by Gouras et al in 1984 by placing human xenografts into monkey eyes.82 In animal models receiving human xenografts, retinal function has been maintained at the transplantation site for long periods.8183 Several anatomical and functional tests have suggested that fetal retinal cells give the best results in the host retina.83 However, the survival of these cells might be affected by age and RPE depigmentation.83 RPE transplantation needs to be conducted at an early stage of the degenerative process so that the rescue effect on degenerative photoreceptor cells can be obtained.83
In neovascular AMD, transplantation of RPE allografts into the submacular space after surgical removal of CNV can lead to macular oedema, chronic fluorescein leakage around the transplant, and gradual reduction of visual acuity. This is attributed to host-graft rejection of the transplanted material, which may require regional immunosuppression at the site of transplantation.8183Subretinal transplantation has also been performed using cell suspensions containing autologous pigment epithelium collected from the human iris before surgery. The results of this technique are not yet known in humans. In the rabbit, although these cells have proved capable of phagocytosis,84 their full metabolic capacity still remains to be elucidated.
Current uncontrolled clinical trials are investigating the potential benefits and complications following transplantation of human fetal neuroretinal cells in patients blinded by retinitis pigmentosa.8385 Results of these studies have suggested that this technique may be less immunogenic, although no convincing evidence of functionality in the host eye has been found.85
In AMD, however, the photoreceptors and RPE are either damaged or destroyed, and thus a graft of the two layers into the damaged macula may be required. Another possibility is the use of the diffusible trophic factor released from normal rods, which has been shown to stimulate cone survival in degenerated retinas.86 This factor still needs to be identified and isolated.
Research has been carried out into the feasibility of by passing damaged photoreceptors and electrically stimulating the remaining viable retinal layers to provide limited visual input to patients who are visually impaired because of severe photoreceptor degeneration. A large number of experimental studies have been performed using either subretinal87-89 or epiretinal90 implanted electronic devices. In experimental models, electrophysiological recording has demonstrated the possibility of electrical stimulation of the inner retina. Histologically, subretinal implants result in a significant loss of retinal cells in areas overlying the implant, while the retina at a distance from the implant and from the surgical site remains normal.88
Some short duration attempts have been performed in the operating room on five patients under local anaesthetic. Local electrical stimulation of the retinal surface resulted in focal light perception that seemed to arise from the stimulated area.91 However, the perception of a spot of light is still a very early stage compared with the perception of shapes. A number of issues still remain to be addressed—localisation of the implant (subretinal or epiretinal), stability of the position of the implant, biocompatibility and the possibility of central fixation, and long term results are awaited.
RADIATION THERAPY
The rationale of radiation therapy is to deliver a precise dose of ionising radiation to a defined area to inhibit neovascularisation within that area, without causing damage to surrounding healthy tissue.92 The mechanism through which ionising radiation inhibits the formation and growth of new vessels has not yet been fully elucidated. Radiation therapy has its major application in the treatment of malignant tumours and intraocular tumours,93and has been investigated as a potential treatment for AMD since the early 1990s.94
In clinical trials, either external beam therapy, also called teletherapy, or brachytherapy is used to treat AMD. The first method involves the use of a clinical linear accelerator that produces a high energy x ray beam delivered to the portion of the eye to be treated. The second method uses sealed radioactive sources that are placed directly into, or adjacent to, the area to be treated.92 Radiation therapy could be applicable to eyes with CNV not amenable to laser photocoagulation, because it is non-invasive, has no effect on the neurosensory retina, and can be conducted with precision.95
The optimal total dose of radiation therapy, fractionation schedule, and method of delivery have not yet been fully elucidated,9295-97 and preliminary results suggest that multiple treatments may be necessary for an effective total dose.92 In short term uncontrolled studies, radiation therapy has been reported to stabilise visual acuity and cause regression of subfoveal CNV.9294 In patients with occult CNV and no classic CNV,98 this technique has been shown to stabilise visual acuity and angiographic choroidal neovascular lesion size in 28 eyes at 6 and 9 month follow up.99 However, recent longer term studies in larger numbers of patients with neovascular AMD have shown that external beam radiation therapy does not control the growth of CNV9597 or have beneficial effects on visual acuity.96 A recent report from a randomised, controlled, double blind study indicated that teletherapy provided no benefits in terms of visual acuity in 178 patients with AMD related CNV at 1 year follow up,100 even though a smaller randomised clinical trial had suggested some benefit.101
Although visual acuity improvement has been suggested to be dose related,9596 there is no convincing evidence that high dose irradiation leads to a beneficial visual acuity effect at this time.95 Furthermore, high doses of irradiation have been associated with the risk of optic neuropathy, and retinal and choroidal vasculopathy (Fig 7).95 In addition, radiation retinopathy may develop in a 6 month to 3 year period with teletherapy, but tends to occur sooner with brachytherapy.95 Extra caution should be taken with radiation therapy in case of potential concomitant retinal vascular disease such as in patients with diabetes mellitus.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Radiation therapy for subfoveal occult CNV. Early phase fluorescein angiogram at presentation (A) shows small adjacent areas of hyperfluorescence and hypofluorescence involving the whole macula. Late phase fluorescein angiogram 1 month later (B) shows active occult new vessels with occurrence of retinal haemorrhage and subfoveal fluorescein leakage 2.5 MPS disc areas in size. No laser photocoagulation treatment could be considered and thus the patient was submitted to radiation therapy. Early phase ICG angiogram (C) performed 14 months after treatment demonstrates five areas of round, hyperfluorescent choroidal dilatation disseminated on the border of the remaining lesion (arrowheads). Later phase ICG angiogram (D) discloses the washout of some of the hyperfluorescent bulges (arrowheads)
ANTIANGIOGENIC THERAPY
To date, the findings from clinical studies with antiangiogenic drugs have not been encouraging.23 A randomised, placebo controlled, multicentre trial of systemic interferon alfa-2a has shown that the therapy for CNV secondary to AMD is not beneficial and may even be harmful.102 Such a specific treatment may be ineffective because of the variety of factors that are involved in angiogenesis.
Other pharmacological agents which have been suggested as potential antiangiogenic drugs for the treatment of neovascular AMD include retinoids, corticosteroids, triamcinolone acetate, thalidomide, matrix metalloproteinase inhibitors, and apoptotic agents.23103-107 Most of these agents have only been studied in animal models: a few of these drugs have been evaluated in small clinical trials. In an animal model of corneal neovascularisation, thalidomide administered orally and intraperitoneally effectively inhibited angiogenesis.103108 The clinical safety of thalidomide in the treatment of neovascular AMD is currently under investigation.109 Among the latter antiangiogenic agents, isotretinoin, a retinoid, has not shown any significant effect, whereas others await further larger scale clinical trials to confirm their effects.23
Several growth factors that have been shown to contribute to the molecular events involved in the regulation of blood vessel growth may play an important part in the pathogenesis of CNV. These include vascular endothelial growth factor (VEGF), transforming growth factor β, platelet derived growth factor, and basic fibroblast growth factor.23 VEGF, in particular, has stimulated much research interest.110-113 These growth factors are not expressed at levels detectable by immunochemistry in normal RPE cells, but show an increased expression in AMD, suggesting a pathogenic role in CNV growth.110
It has been suggested that basic fibroblast growth factor and VEGF act synergistically to accelerate neovascularisation, and that upregulation of VEGF is stimulated by hypoxia, which is possibly a pathogenic factor in CNV secondary to AMD.110-112 This hypothesis is further strengthened by the findings from a study in 164 patients undergoing intraocular surgery showing that VEGF concentrations are elevated in those patients with active intraocular neovascularisation.111 Inhibitors of VEGF have been identified in studies conducted in vitro and in animal models, and include VEGF antagonists and suppressants, and inhibitors of the VEGF intracellular transduction cascade.23111 Clinical research will confirm whether growth factors are better targets for antiangiogenic therapies in the future.
OTHER STUDIES USING PHOTODYNAMIC THERAPY WITH VERTEPORFIN
A phase IIIB investigation, the Verteporfin In Photodynamic Therapy (VIP) Trial should provide further understanding of the benefits of verteporfin therapy in eyes with CNV that were not included in the TAP investigation. This trial includes a large proportion of eyes with subfoveal CNV secondary to AMD containing an occult component but no classic component. Patients were enrolled with subfoveal occult CNV secondary to AMD associated with haemorrhage or visual acuity deterioration within the past 3 months (⩾1 line loss), or evidence of anatomical growth of the neovascular lesion within the past 3 months (an increase of 10% or more of the GLD on fluorescein angiography). In addition, the VIP Trial enrolled patients with subfoveal CNV secondary to AMD that had a classic component, if the visual acuity was better than that in patients enrolled in the TAP investigation (specifically, better than 20/40). Since the results from the phase I/II investigation suggested that verteporfin therapy might be beneficial in subfoveal CNV secondary to pathologic myopia,56 patients with this type of lesion were also enrolled in the VIP trial. Recent results reported that the therapy was beneficial for subfoveal lesions caused by pathological myopia.114 However, no statistically significant difference for the primary outcome (<15 letter loss at the month 12 examination) was reported for the subgroup of patients with AMD with occult CNV but no classic CNV at baseline.
PHOTODYNAMIC THERAPY WITH OTHER PHOTOSENSITISERS
A number of other photosensitisers are being developed for the treatment of AMD. For example, lutetium texaphyrin (Lu-Tex) is a water soluble photosensitiser with an absorption peak at 730 nm.115 Studies in a tumour model in mice have shown that the optimum time of irradiation may be 24–48 hours after injection of the photosensitiser.115 In an experimental monkey model, cessation of fluorescein leakage from CNV was obtained with 1–2 mg/kg body weight of Lu-Tex and a light irradiation dose of 50–100 J/cm2.116 At these doses there is limited toxicity to retinal and choroidal structures. Lu-Tex is currently in phase I clinical trials which evaluate the safety of this compound for patients with subfoveal CNV.
Tinethyl etiopurpurin (SnET2) is activated by low energy 664 nm red light. Preliminary work with this photosensitiser includes photodynamic therapy of corneal neovascularisation in rats and in rabbits.117 The activating light can be administered 5–20 minutes after SnET2 injection to cause effective occlusion of choroidal capillaries. In phase I/II trials conducted in 28 patients with subfoveal CNV, photodynamic therapy with SnET2 (0.5–1.0 mg/kg body weight) resulted in cessation of leakage of fluorescein from CNV associated with improvement in visual acuity in 89% of 28 eyes within 1 week of treatment.118 Fluorescein leakage was noted in 64% of the eyes 12 weeks after initial treatment. Longer term visual acuity effects of this treatment were investigated in a subsequent study, in which 14 eyes were treated with 0.25–1.0 mg/kg body weight of SnET2 using a light dose of 35 J/cm2.119 At the 6 month follow up examination, visual acuity declined by 1.1 lines in 50% of the treated eyes. Patients are currently being enrolled in a phase III trial to determine if this treatment can reduce the risk of visual acuity loss compared with placebo.
Mono-l-aspartyl chlorin e6 (NPe6) is a hydrophilic photosensitiser, which is activated at 664 nm and has been shown to selectively occlude experimentally induced CNV in primates.120 As a hydrophilic agent, NPe6 is supposed to have the advantages of having limited extravascular uptake and rapid elimination. Consequently, the duration of skin photosensitivity will be shorter with this agent than with HPD.121
Conclusions
Because the prevalence of AMD is associated with age, its socioeconomic implications are becoming more important as the proportion of older people increases in developed countries. However, AMD not only affects people in the older age groups; people over 50 years of age, who are still relatively young and may still be active, are also at an increased risk of acquiring the disease.
No preventive treatment exists for neovascular AMD, the form of AMD that is responsible for severe vision loss, although two approaches are under investigation, including micronutrient use (Age Related Eye Disease Study)122123 and light laser photocoagulation (Complications of Age Related Macular Degeneration Prevention Trial).124 If left untreated, neovascular AMD will usually result in a poor vision outcome. During the 1990s, laser photocoagulation was used to treat neovascular AMD, but it can only benefit a small proportion of selected cases. Other therapies, such as surgery, radiation therapy, and antiangiogenic therapy, are under investigation.
Photodynamic therapy is a proved treatment modality for certain eyes with subfoveal CNV secondary to AMD. Compared with other light activated drugs, verteporfin is at the most advanced developmental stage. Phase III data from 12 and 24 months demonstrate that verteporfin therapy is safe, with few systemic side effects and no prolonged skin photosensitivity, and that verteporfin therapy reduces the risk of vision loss in subfoveal cases with predominantly classic CNV. Verteporfin therapy does not repair irreversibly damaged tissue but might prevent further growth of CNV as suggested by fluorescein angiography. Verteporfin therapy became available in early 2000 as the first drug therapy for patients with subfoveal neovascular AMD.
Several new treatment opportunities may be afforded by verteporfin therapy because this new treatment modality, without the destructive effects on the neurosensory retina seen with laser photocoagulation, can be of benefit to a greater number of patients with subfoveal lesions compared with photocoagulation. The results from current clinical investigations will confirm whether verteporfin therapy is useful in the treatment of a wide range of cases of subfoveal CNV due to AMD with occult CNV but no classic CNV and cases with CNV due to non-AMD causes, such as pathological myopia.
Acknowledgments
The authors thank all the members of the TAP Study Group, whose names and affiliations are listed in the following reference: Treatment of Age-related Macular Degeneration With Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin. One-year results of 2 randomized clinical trials—TAP Report 1. Arch Ophthalmol1999;117:1329–45.
References
Cover illustration: Birds of a feather
The barking owl (Ninox connivens) is a medium to large Australian owl with bright yellow eyes and interesting vocalisations. This hawk-like owl is agile and aggressive and could be described as crepuscular. Others would describe these birds as semidiurnal as they have been seen taking live prey in broad daylight.
One of the bird's vocalisations provides a reason for its name because it does indeed sound like a barking dog (a gruff double bark), and it was not understood as the call of an owl until the 1930s. The bird was known as the winking owl before that time. Both sexes make the same call, but the female's call is higher pitched and seems to penetrate the dense foliage of the forest better than the male's. The other principal call, referred to as the “screaming woman”, mystified ornithologists for decades until satisfactorily identified as also belonging to the barking owl. The “screaming woman” call is only heard occasionally, generally in the Australian autumn months of March and April and is given 8–10 times over approximately 90 seconds. Indeed, the sound resembles the cry a woman might utter in abject terror. This call is usually given outside of the breeding season, but its significance is unknown.
These robust birds are versatile predators and take a great variety of prey including insects, fish, mammals, marsupials, and many bird species, including ducks and even tawny frogmouths. Their ideal habitat is open country with large trees for roosting, but the owl's range extends even into the rain forest. Both sexes are fearless and pugnacious at the nest. The upper part of the cover shows the face of a barking owl. The bottom half of the cover deserves a bit more explanation.
Birds are covered in feathers. Feathers are composed of keratin and are among the strongest material per weight produced by an animal. There are at least four different types of feathers including contour and flight feathers, down, filoplumes, and powder-down feathers. Look closely around the eyes of the barking owl and you will see what look like eyelashes. These are filoplumes, modified feathers that resemble hair in both appearance and function. Filoplumes come in at least two varieties, both of which can be found around the eyes. The bristles (subclass of filoplumes) are stiff, straight, and most closely resemble lashes. Most filoplumes have a sensory function, acting as movement detectors.
The bottom half of the cover exhibits two different electron micrographs to illustrate the similarity between filoplumes and lashes. The left hand electron micrograph is a shaft of a human lash (×3673) and the right hand one is of a shaft of a periocular avian filoplume simulating a lash (×3673). If you were not familiar with electron microscopy of eyelashes, you might guess that the photographs were reversed in the printing process. We assure you they are not reversed.
Convergent evolution has created the same form for the periocular protection of the ocular surface with lashes or lash-like structures to prevent stray matter from entering the eye from above and pressure and movement detection to provide avoidance when necessary (the blink reflex). The avian outer eyelids are very different from human eyelids as they utilise smooth muscle and rarely close during waking hours. None the less, the lash-like filoplumes have evolved in a manner very similar to that of human hair. Or, perhaps human hair has evolved to look like filoplumes, since birds are evolutionarily older than humans. In either case, it would appear that ocular protection with stiff sensitive structures is a preferred adaptation.—Ivan R Schwab, MD, UC Davis Department of Ophthalmology, 4860 Y Street, Suite 2400, Sacramento, CA 95817, USA (irschwab{at}ucdavis.edu).
Electron microscopy provided by Robert Munn, MD. Thanks to the Perth Zoo for allowing the photography and to Paul McMenamin, PhD, for enabling the photography.