Article Text

Statistics from Altmetric.com
Self enucleation or “oedipism”1 is a rare form of self mutilation, occurring with paranoid delusions, either as a result of a drug related toxic psychosis or in functional psychoses, such as schizophrenia. It is most often described in acutely psychotic patients, who have religious or sexual delusions.2
We report a case of self enucleation of a right eye in a 19 year old male—induced by drug psychosis. The force of autoenucleation traumatised the chiasm resulting in a left temporal field defect. Only two cases of contralateral field defect secondary to chiasmal damage have been reported in the literature.3,4 Many drugs are known to cause hallucination leading to self mutilation.
Deliberate self harm (DSH)5 is a well known entity which varies from mild (skin picking and hair pulling) to severe forms of self mutilation like self amputation and self enucleation.5 DSH is known to result from delusions and command hallucinations occurring in psychotic and mood disorders, dementia, personality disorder, drug misuse, and mental retardation. In adults, attempts at ocular damage are associated with acute psychosis, self enucleation being the extreme form of ocular mutilation.
Case report
A 19 year old man was admitted following attempted enucleation of his right eye during an acute psychotic episode after taking ecstacy, LSD, and excess alcohol. He described, “seeing an army of police officers attacking him.” He attempted to remove a “bomb” which had gone into his eye using a nail clipper and pliers. He was still in a state of psychosis running around aimlessly and had to be held to the ground by six people to prevent further self mutilation.
He was admitted to a general medical hospital in a state of psychosis and was treated with haloperidol. He had no known past psychiatric disorders. He is healthy, fit with no known past medical illness. Full blood count, urea and electrolytes, and blood gases were normal.
Toxicology of urine and blood were positive for amphetamine; no test for LSD was performed
He was transferred to the Royal Victoria Eye and Ear Hospital on the same day in a stable condition. Ocular examination revealed no perception of light in his right eye with severely chemosed eyelids and the globe could not be visualised. Visual acuity in the left eye was 6/6 with normal anterior segment and fundus examination.
Exploration of the right socket under anaesthesia revealed no identifiable structures except for orbital fat, inferior rectus muscle, conjunctiva, and Tenon’s capsule (fig 1). The optic nerve stump was not visible. A porous polyethelene orbital implant was inserted, the Tenon’s and conjunctiva sutured over it in separate layers. Considering the instruments and force used to extract the eye, surprisingly there was no apparent loss of conjunctival tissue, leaving adequate fornices for a prosthesis, which was fitted 6 weeks later.

Tolal absence of globe.
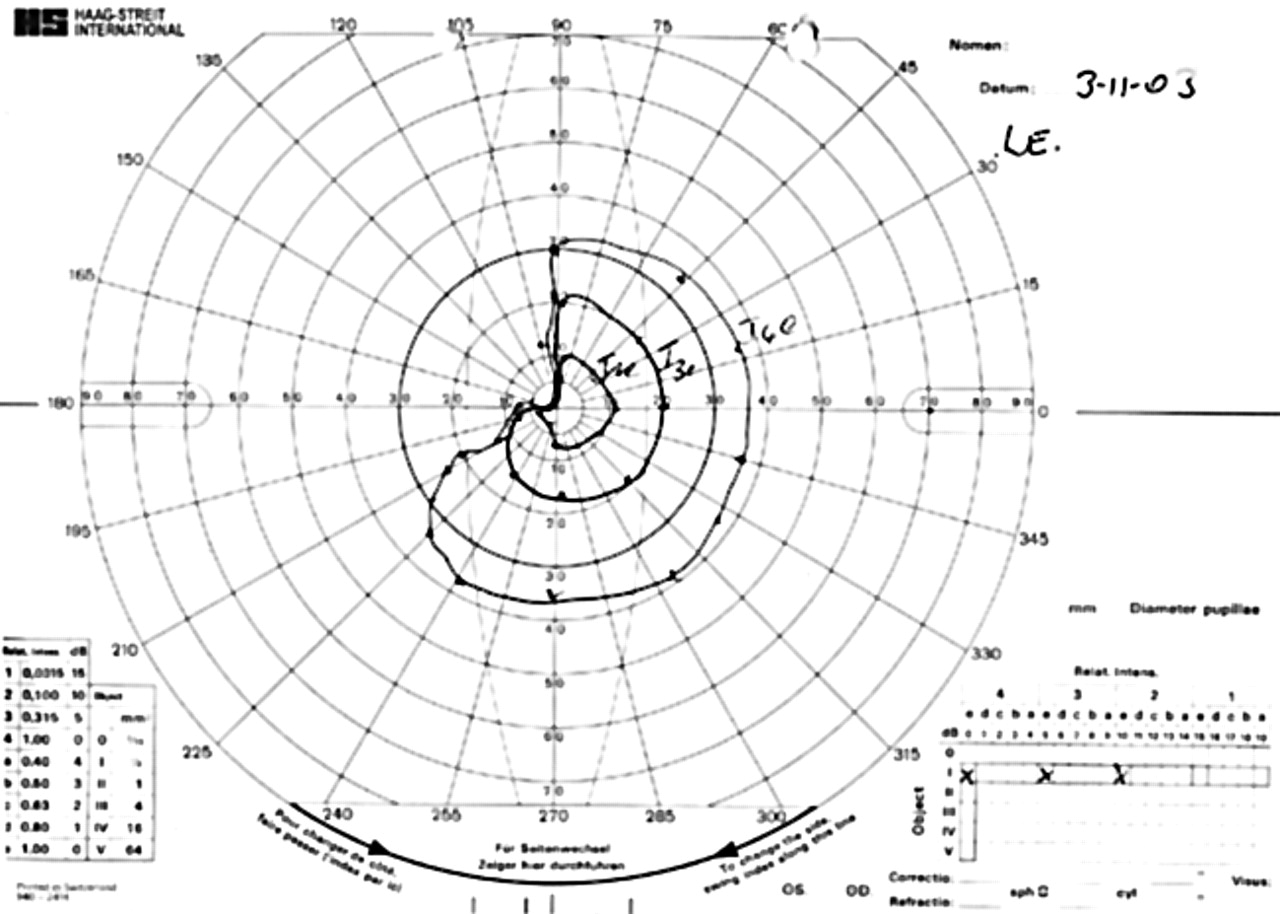
Goldmann visual field showed left upper temporal quadrantanopia to the I4e and I3e targets, and a left hemianopia to the I2e target (fig 2), indicating trauma to the chiasm. The patient has been advised not to drive at present. A magnetic resonance image showed no visible abnormality of the chiasm or left visual pathway. The patient is being closely monitored by the psychological team and is attending a drug rehabilitation clinic.
{kind=link}
{kind=link}
Goldmann field of the left eye.
Comment
This report presents a rare case of a self enucleation of the right eye in a young man. This severe trauma resulted in loss of vision in the right eye and partial visual field loss in the other eye. Avulsion of the optic nerve was found in the right eye. The left eye showed no evidence of ischaemia or sympathetic ophthalmia. The visual field defect of the left eye resulted from traumatic severance of the right optic nerve causing secondary chiasmal damage. There were no intracranial complications.
Life threatening complications may result from self enucleation, including intracranial or subarachnoid haemorrhage, cerebrospinal fluid leakage, and bacterial meningitis.3 Radiographic imaging is required to exclude intracranial bleeding, optic chiasmal injury, and bone fractures.
Self enucleation or “oedipism” is a rare entity which requires operative reconstruction of the orbit, and also neurological monitoring to identify and treat any possible intracranial complications. The other eye should be observed for possible sympathetic ophthalmia which may occur because of residual uveal tissue in the socket. Visual field of the remaining eye must be performed in the acute phase, as field loss secondary to chiasmal trauma or severance traumatic optic neuropathy may occur and may respond to intravenous steroids,4 though this is controversial. Field loss will have implications with regard to driving and some occupations and may even require the patient to be registered as partially sighted.
Long term psychiatric therapy should be implemented to prevent further self injurious behaviour, as according to literature severe forms of self mutilation after self enucleation can occur.6 This includes attempted suicide.
Though cases of severance optic neuropathy and chiasmal damage are rarely reported, this may be due to lack of symptomatology and failure to perform field testing. The importance of visual field analysis cannot be overemphasised, because of the potential implications for affected patients.