Article Text

Statistics from Altmetric.com
Although success in treating intraocular retinoblastoma with radiation was first reported in 1903,1 all the eyes originally treated with radiation were lost as a result of radiation complications. Stallard in England2 and Reese in the USA3 recognised that by modifying the technique, it was possible to save the child's life, eye and in some cases vision. Stallard and Reese pioneered the use of external beam radiation, but it was Stallard who developed and perfected the use of brachytherapy for retinoblastoma in the 1930s.
Radiation was almost never used for unilateral cases, as they were all deemed too advanced to treat with anything but surgery. Thus, virtually all the eyes that received radiation were children with the germinal form of retinoblastoma. More than 50 years ago, it was recognised that some of these irradiated children subsequently went on and developed cancers outside the eye (called ‘second non-ocular cancers’). Reese believed that these second cancers were an unfortunate complication of radiation alone, as they only developed in irradiated children and in the field of radiation and after long latent periods. Subsequent work by Sagerman et al4 confirmed a lower incidence with lower doses, and in recent years a clear dose–response curve for sarcoma development in the field of radiation was demonstrated. In going from 35 Gy to 60 Gy, the incidence of sarcoma development is increased by eightfold.5
Even before the retinoblastoma gene was cloned in 1986,6 it was clear that genetics played an important role in the development of these cancers and that it was primarily the gene, not radiation, that was the cause of these cancers. By the 1990s, the most common cause of death of a retinoblastoma patient in the USA was not metastatic retinoblastoma, but rather these second (or third, fourth or fifth) cancers.7 The alternative to radiation (and enucleation) for advanced eyes has been systemic chemotherapy. Systemic chemotherapy for intraocular disease was first used in 1953 by Kupfer.8 Reese was so impressed that he immediately began using it and published on its use in over 300 cases.3 Reese's idea was to use systemic chemotherapy with radiation in the hope of decreasing the dose of radiation from 15 000 cGy to 7500 cGy. Ultimately, he abandoned chemotherapy because of the associated systemic toxicity. In the 1970s, Bob Ellsworth, MD and I began using multiagent systemic chemotherapy as salvage treatment.9 We quickly learnt that despite the dramatic response to vincristine, cytoxan and Adriamycin, tumours would regrow when chemotherapy was stopped, so we focally treated the (temporarily) shrunken tumour with focal techniques with success. We gave that up because of the cardiac toxicity of Adriamycin.
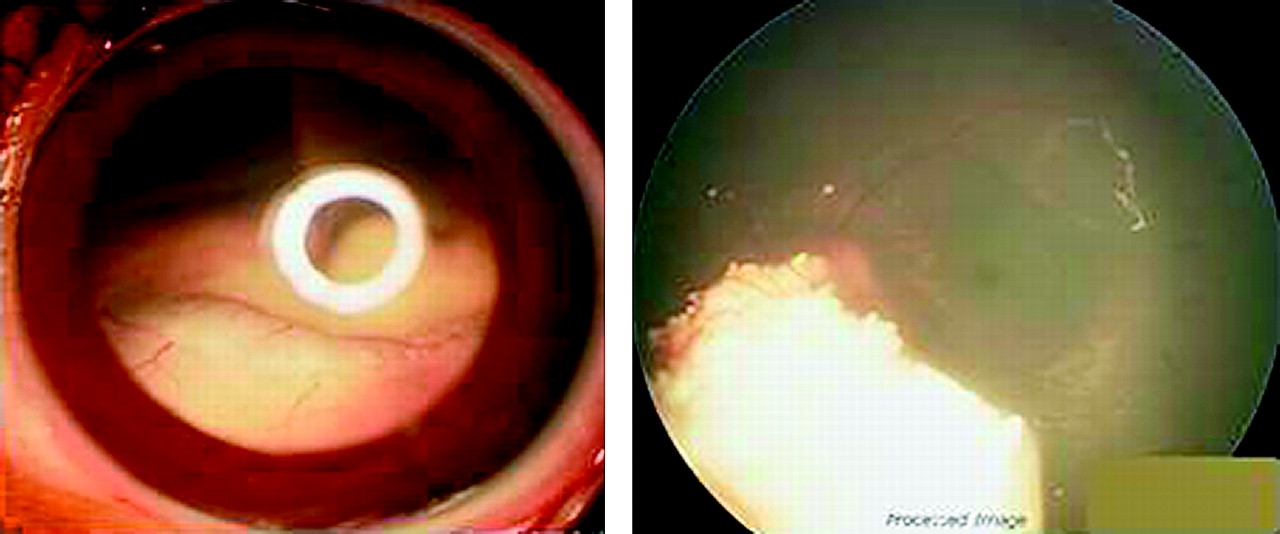
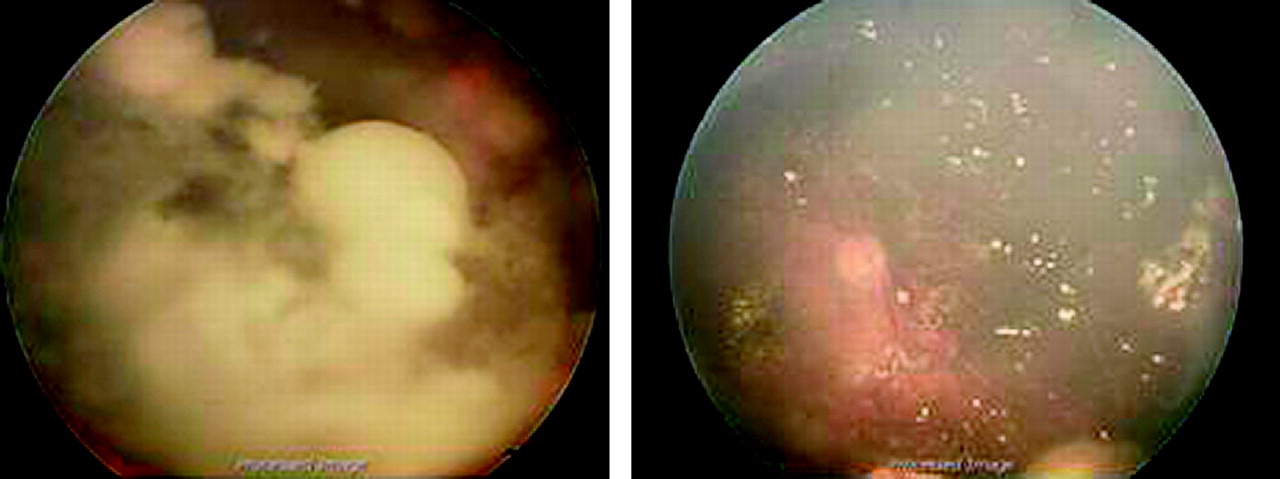
Beginning in the 1990s, all centres worldwide began using chemotherapy for intraocular disease in the hope of diminishing the use of external beam radiation. Since then, more than 150 papers have been written, and all the publications have demonstrated that carboplatin-based therapy (with one, two or three additional drugs) causes a rapid reduction in the size of intraocular tumours (approaching 50% reduction within 3 cycles/3 months).10 For example, figure 1 represents the right eye and figure 2 the left eye of a single patient before and after three cycles of systemic chemotherapy. In both eyes, the optic nerve was not visible before treatment, and the tumour has pulled away from the nerve in subsequent photographs. Although protocols vary considerably in the drugs used (generally carboplatin with vincristine and/or in addition etoposide, VP16 (VM 28 in Canada), cisplatin and topotecan), number of drugs used (1,2,3 with/without ciclosporin-A) and duration (once, 6 months, 9 months, 12 months or 15 months), all centres have had gratifying responses. The overwhelming number of eyes treated have been saved without compromising the excellent ocular and patient survival available in the radiation only days.

Impact of systemic chemotherapy on advanced intraocular retinoblastoma. Right eye before (upper left) and after (upper right), left eye before (upper left) and after (upper right) multiple cycles of systemic chemotherapy.

Fellow eye of patient in figure 1 before and after systemic chemotherapy.
Despite these many successes, there has been worldwide disenchantment with this approach. Retinoblastoma at diagnosis is almost always a localised disease, and many have questioned the use of chemotherapy for young children for a localised cancer. Systemic chemotherapy for intraocular retinoblastoma is rarely curative alone. Although studies vary, the overwhelming majority of studies show that at least 75% of tumours treated with chemotherapy will recur if not additionally treated.11 In some cases, the use of laser and or cryotherapy is sufficient to salvage the eye, but enucleation and external beam irradiation are still necessary to save the eye. It is now recognised that eyes that initially receive systemic chemotherapy and then have external beam radiation are at higher risk for complications that compromise both vision and the anatomical integrity of the eye.12
One of the disconcerting side effects of the use of systemic chemotherapy in retinoblastoma has been impairment of hearing. Recently, two long-term studies have demonstrated that long-term impairment of hearing in patients treated with chemotherapy is more common than thought. In France, a 5% incidence of measurable hearing impairment has recently been reported,13 as has a 20% rate from St Jude. Younger children appear more sensitive to these effects, and a third of the children in St Jude's experience under the age of 6 months have measurable hearing deficits.14 Some centres have used cis-platin instead of carboplatin, and from Mexico it has been shown that 100% of children treated had hearing impairment.15
In the days of external beam irradiation, treatments were done over a month and children followed every 3 months under anaesthesia. Now, however, in the days of systemic chemotherapy, curing an eye requires monthly exams, many repeated focal treatments and repeated examinations for exam, studies, procedures, etc. It has been called ‘an arduous journey’ by the St Jude team.16 They reported their experience with 25 of their children. These children had 895 outpatient appointments, 698 exams under anaesthesia, 230 focal treatments and 1272 anaesthesias, and collectively travelled 822 312 miles for these exams, procedures and treatments.
Since the cure rate for children with retinoblastoma is so high, long-term issues of fertility are a realistic concern. There is no information on long-term fertility questions in retinoblastoma survivors, but such information has been collected in children who have survived other cancers (in some cases with similar and some cases with different drugs). The subject of fertility in prepubertal children who receive chemotherapy was reviewed in the New England Journal of Medicine this year. It was pointed out that treatment regimens for childhood cancer are ‘extremely toxic and pose a threat to the fertility of young patients,’ and it recommended that alkylating agents (used in all centres for retinoblastoma patients) including etoposide should be ‘eliminated.’17
There are many ‘routine’ complications of chemotherapy that are expected in any child receiving multiagent chemotherapy. Despite the more than 100 papers published detailing the use of chemotherapy for intraocular disease, an attempted meta analysis of complications was impossible because so few publications even list complications associated with treatment. This was the subject of an editorial in the Archives of Ophthalmology, where it was pointed out that 100% of the children need ports (which includes surgery, anaesthesia and a known rate of infection and failure), 100% of children need red cell transfusion(s), about 50% have significant thrombocytopaenia or require platelet transfusion, all children have at least one hospitalisation for complications, and fever/neutropenia develops in as many as 50% of these children.18 Increasingly, the problems of transfusions are being highlighted in the literature. There are obvious issues such as cost, anxiety, time and anaphylaxis, but significant complications are worth mentioning. In countries that transfuse blood that has not been irradiated, graft versus host disease can develop. Transfusion-related acute lung injury develops in 1/5000 transfusions but carries with it a 5–10% mortality. Most people think that transmission of serious infections is rare and does not occur in the Western World. One such infection is Babesiosis, which develops in 1/600 to 1/800 transfusions and is fatal in 5–10% of cases. Interestingly, in 2008, there were 39 cases of transfusion transmitted Babesiosis in New York City alone.
The main driving force for the use of systemic chemotherapy has been the development of (fatal) second non-ocular cancers. It was widely predicted that the use of chemotherapy would eliminate the second cancers related to irradiation. Unfortunately, it has not turned out that way. Four studies19–22 employing different methodologies, using different chemotherapy at various doses (and from different countries) with different endpoints, have attempted to look at this important question, and all four have demonstrated that children receiving chemotherapy and radiation are at higher risk for the development of second cancers than those receiving radiation alone. In the first such study published in 1986,19 there was a threefold difference in second cancer incidence. Using better statistical modelling, two studies have suggested an increase in standardized incidence ratios (S/I/R) of 25–60%.
The major established cause of acute myelogenous leukaemia (AML) is chemotherapy, and this has been recognised for more than 10 years. In fact, this form of leukaemia is referred to as secondary acute myelogenous leukaemia (sAML). The leukaemia is a known consequence of predictable molecular derangement caused by certain drugs, especially epipodophyllotoxins (etoposide is the one used extensively in retinoblastoma worldwide) and alkylating agents (also used routinely for retinoblastoma); between 2 and 12% of patients who receive epipodophyllotoxins will develop this second cancer.23
Prior to the introduction of chemotherapy for retinoblastoma, this type of leukaemia had never been reported in even one retinoblastoma patient. Gombos and others collected 15 cases of sAML in retinoblastoma patients worldwide,24 and the majority of these patients died of their chemotherapy-induced leukaemia. While this paper has been criticised (because the authors do not know the denominator), there appears to be little doubt that the sAMLs were related to chemotherapy treatment.
Although our experience with super selective ophthalmic artery delivery of chemotherapy for retinoblastoma began in an IRB approved protocol in May 2006 (with collaborators Pierre Gobin, MD, Ira Dunkel, MD, Scott Brodie, MD, Jonathan Kim, MD and Brian Marr, MD) we designed our protocol on the prior publications from two groups. In the 1950s, Reese used intracarotid injections of chemotherapy (triethylene melanamine TEM) for retinoblastoma in the hope of decreasing the total dose of radiation. The Japanese investigators Mohri and Kaneko developed a balloon catheter for selective delivery of chemotherapy in retinoblastoma.25 The catheter was passed up into the carotid on the side to be treated from the femoral artery, and when the balloon was just beyond the orifice of the ophthalmic artery, they expanded their balloon and injected chemotherapy posterior to the balloon. Their studies had suggested that Melphalan was the best agent to use. Melphalan is an alkylating agent, approved for adults only and available for more than 50 years now. Because the chemotherapy was not placed directly into the ophthalmic artery, it was called ‘selective.’
Our technique is referred to as ‘super selective,’ because we pass a small catheter (diameter 450 μm) from the femoral artery directly into the ophthalmic artery and then inject the chemotherapeutic agent directly into the ophthalmic artery in a pulsatile fashion over a 30 min period. Details of the technique have already been published elsewhere.26 27 Our initial protocol called for eyes that were advanced (Reese–Ellsworth V eyes) and scheduled for enucleation. Most of these eyes had no sight and flat ERGs with afferent pupillary defects. We reported our results in our first 10 eyes.26 Despite the advanced nature of these eyes, we retained eight of the nine we treated. In one case, we were unable to cannulate the ophthalmic artery. Since that time, we have been successful in cannulating the artery in every case. That publication emphasised that the procedure could be repeatedly done without local complications (as many as six times), that there were minimal systemic problems, that very advanced eyes could avoid enucleation and that in a few cases there was improvement in vision, pupillary response and ERGs. Many eyes with vitreous seeds and/or total retinal detachment were salvaged. An example from this original (previously reported) group is shown in figure 3.
We have now performed the procedure over 200 times, and patients clearly fall into two groups: those who are primarily treated with chemosurgery and those who are treated after exhausting every other treatment (frequently in an only eye) and are desperate to avoid impending enucleation (figure 4). We have completed our analysis of the cases treated primarily in the past 3 years, and I will present them below. Although our analysis of refractory cases treated with chemosurgery is still under review, the success rate is lower (between 50 and 66% of cases) and the ocular complications higher. Neither group has any significant systemic complications from treatment.

Reese–Ellsworth Vb eye that had failed all prior treatments before (left) and after (right) intra-arterial melphalan.

Reese-Ellsworth Vb eye that had failed all prior treatments before (left) and after (right) intra-arterial melphalan. Unfortunately the response was not durable.
Our initial hope was that chemosurgery would be as effective as systemic chemotherapy but have fewer side effects. As of 31 May 2009, we had used chemosurgery as initial management in 28 patients. There were no patient deaths, no child required transfusion, there were no strokes and no complications at the femoral artery site, and no child required a port. Twenty-seven of these eyes have been saved to date, and the Kaplan–Meier 3-year survival is 88%. The one eye that came to enucleation had active disease, confirmed pathologically, but the optic nerve showed no evidence of local toxicity. When one realises how advanced these eyes are, in the future the ability to save eyes using chemosurgery as an initial therapy will be very high (over 90%).
We then wondered if six cycles were necessary, and since the response was so dramatic, we wondered if radiation (external beam or plaque) were needed at all. It quickly became obvious that most eyes could be cured with an average of three sessions. It was also apparent that radiation was not needed, and for more than 2 years now, no eye we treated has subsequently had any form of radiation. An example of advanced eyes that were treated with only three sessions and no radiation is presented in figure 3.
In our initial 10 patients, we had noted a few who had an improvement in ERG status. We then recognised that most of the patients who had a significant improvement in ERGs had retinal detachments that completely resolved, thus explaining the improvement in retinal function.
Our next step was treatment of both eyes at the same session. We have called this ‘tandem treatment.’ This has not been a technical challenge, but it does require giving the child a total higher dose of chemotherapy. Despite this, we have not needed any transfusions in these children.
We have also been interested in the cost of this procedure. A recent analysis of our costs done by Amanda Kosack revealed that the total cost of intra-arterial chemosurgery was half the cost of systemic chemotherapy. Interestingly, two-thirds of the cost of systemic chemotherapy goes towards managing the side effects of the chemotherapy itself. Since chemosurgery has no need for ports, transfusions, hospitalisations for fever, neutropenia or infection, the cost of chemosurgery is less.
An overall comparison of the standard complications of systemic chemotherapy (published) and chemosurgery is presented in table 1.
Comparison of systemic side effects of intra-arterial chemosurgery with previously reported side effects of systemic chemotherapy for retinoblastoma
Although there have been no significant ocular complications from the procedure, three things have developed that are of interest.
One patient had transient periocular lid oedema. It resolved within days and was painless.
Four patients developed redness in the forehead just temporal to the midline that can extend from the lid up into the forehead. The redness is flat, blanches with pressure and is transient (figure 5).
Five patients have developed nasal lash loss. The lashes return, and they have no symptoms.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Typical transient localised redness in the distribution of the supratrochlear artery seen after intra-arterial melphalan delivery.
The redness seen and lash loss are in the distribution of one of the branches of the ophthalmic artery, the supratrochlear artery (previously called the frontal artery), and are due to the drug itself.
As with all new techniques, careful follow-up of all patients is needed before long-term success or complications are known, but chemosurgery is an exciting, new approach to retinoblastoma.
References
Footnotes
Linked articles 174276
Funding The Fund for Ophthalmic Knowledge; Louis and Rachel Rudin Foundation.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Weill-Cornell IRB.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Editorial