Article Text

Statistics from Altmetric.com
Recently, there have been several reports concerning the efficacy of intravitreal bevacizumab injection (IVB) in reducing macular oedema in patients with retinal vein occlusion (RVO).1 2 According to a safety survey of IVB, adverse ocular events are extremely rare.3 At our clinic, we have performed more than 300 IVB for RVO, and the majority of these injections did not have any adverse results. However, we experienced two cases of progression of macular ischaemia despite an improvement in macular oedema after IVB for central retinal vein occlusion (CRVO) in patients with poor glycaemic control of their diabetes and a history of systemic vascular disease.
Case report
Case 1
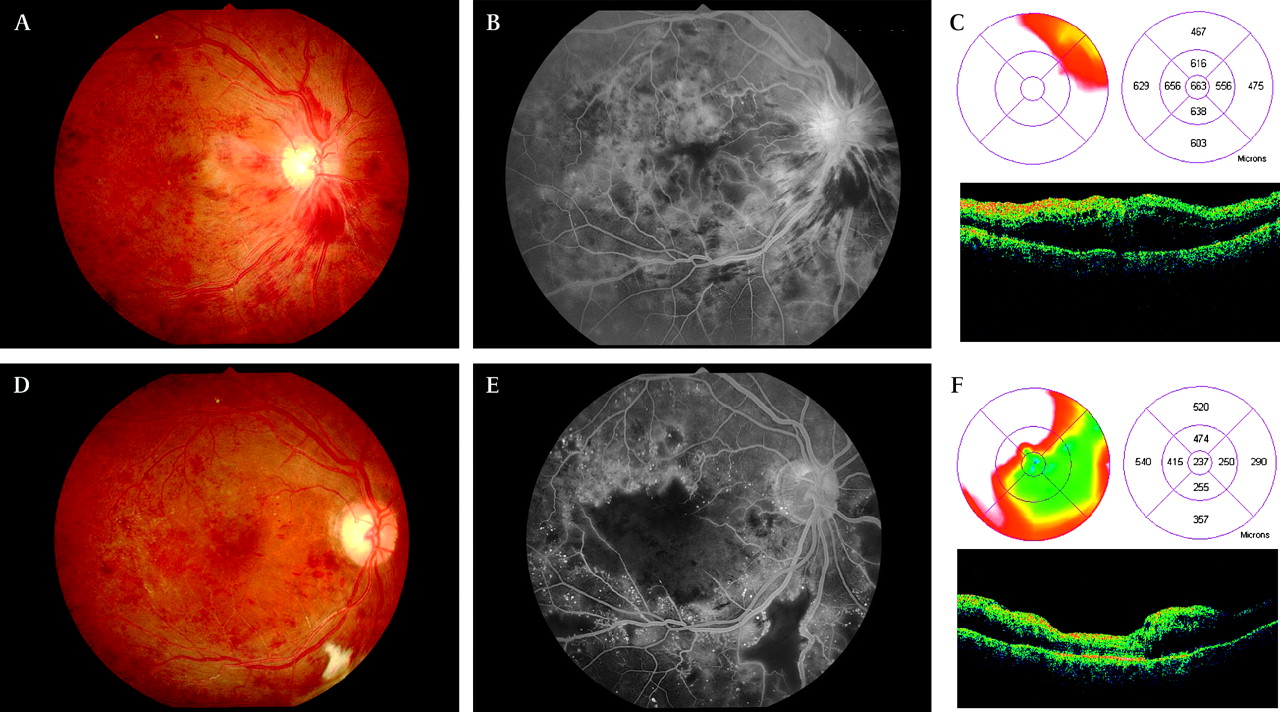
A 76-year-old female with diabetes for 26 years, without a history of retinopathy, presented with CRVO in the right eye (figure 1A) and no retinopathy in the left eye. She was treated with insulin, but had poor glycaemic control (HbA1c 9.6%). General blood examination revealed mild renal dysfunction (BUN: 19.8 mg/dl, Cr 1.1 mg/dl). She had a history of a cerebrovascular accident (CVA) 5 years previously. Initially, her best-corrected visual acuity (BCVA) was 20/200. Fluorescein angiography (FA) revealed diffuse hyperfluoresence of the macular area (figure 1B), and optical coherence tomography (OCT) indicated definite macular oedema (figure 1C). The central foveal thickness (1000 μm in diameter) as deduced using the OCT retinal mapping program was 663 μm.

Fundus photograph (A) and fluorescein angiography (B) before bevacizumab injection in central retinal vein occlusion. Optical coherence tomography showed prominent macular oedema (C). Four weeks after intravitreal injection of 1.25 mg bevacizumab, retinal haemorrhage had regressed (D). Although optical coherence tomography showed a regression of macular oedema (F), fluorescein angiography indicated foveal ischaemia and non-perfusion area out of temporal inferior vessel arcade (E). Best-corrected visual acuity did not change from 20/200.
After obtaining approval from the Institutional Review Board (IRB) and informed consent, she received IVB (1.25 mg) to reduce the macular oedema.
Four weeks later (3 months after the onset of CRVO), despite regression of the retinal haemorrhage (figure 1D) and improvement in the macular oedema to 237 μm (figure 1F), the BCVA was still 20/200, and FA revealed an area of prominent non-perfusion of the macula (figure 1E).
Case 2
A 74-year-old male with diabetes for 20 years, without retinopathy, presented with CRVO in the left eye (figure 2A) and no retinopathy in the right eye. He took oral antiglycaemic drugs but was in poor glycaemic control (HbA1c 11.2%). He had no renal dysfunction. He had a history of a non-fatal myocardial infarction (MI) 8 years previously. Initially, his BCVA was 20/100. FA and OCT revealed definite macular oedema associated with CRVO (figure 2B,C). After obtaining the approval of the IRB, he received IVB (1.25 mg) twice. One week after the first injection, macular oedema had regressed, and BCVA was improved to 20/40. However, 6 weeks later, recurrence of macular oedema was seen, and BCVA had decreased to 20/200, so the patient received a second injection. Four weeks later (5 months after the onset of CRVO), despite regression of the retinal haemorrhage and macular oedema (figure 2D,F), the BCVA remained 20/200. FA revealed an area of non-perfusion of the macula (figure 2E).

{kind=link}
{kind=link}
Fundus photograph (A) and fluorescein angiography (B) before bevacizumab injection in central retinal vein occlusion. Optical coherence tomography showed prominent macular oedema (C). 1.25 mg of intravitreal bevacizumab was injected twice, and 10 weeks after the first injection, retinal haemorrhage had regressed (D). Although optical coherence tomography showed regression of macular oedema (F), fluorescein angiography indicated foveal ischaemia (E). Best-corrected visual acuity worsened from 20/100 to 20/200. ILM-RPE, internal limiting membrane-retinal pigment epithelium.
Comments
In these two cases, despite the fact that IVB was effective for a reduction in macular oedema, visual function did not recover due to the onset of macular ischaemia. Both patients had diabetes mellitus with poor glycaemic control and a history of a non-fatal CVA or MI, and which may have contributed to the progression of macular ischaemia.
Bevacizumab is a humanised immunoglobulin G monoclonal antibody that binds to all VEGF isoforms with high specificity, thus impairing both physiological and pathological angiogenesis.4 Although spontaneous progression of non-ischaemic CRVO to ischaemic CRVO may have occurred,5 the possibility that bevacizumab suppressed the physiological angiogenesis in patients with chronic, debilitating illnesses like our cases, cannot be excluded. Recently, IVB-induced ischaemic change in non-ischaemic CRVO was reported.6 Therefore, IVB should be considered carefully when used in patients with systemic conditions such as diabetes mellitus, hypertension or a history of CVA, MI.
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the Institutional Review Board of NTT East Japan Tohoku Hospital Clinical Research Ethics Committee.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.