Article Text
Supported by the EGS Foundation

Statistics from Altmetric.com
2 Classification and Terminology
2.1 - Primary Congenital Forms/Childhood Glaucomas
Primary congenital glaucoma is a rare disease but has a major impact on the child’s development and quality of life over his/her whole life span. Early diagnosis and appropriate therapy can make a huge difference in the visual outcome and can prevent lifelong disability. Surgical treatment is always necessary1, 2 [I,C].
2.1.1 Primary congenital glaucoma (PCG): from birth to >2 years of life
Neonatal or newborn onset (0-1 month)
Infantile onset (>1 until 24 months)
Late onset or late recognized (>2 years)
Spontaneously non-progressing cases with normal IOP but typical signs of PCG may be classified as PCG
Etiology:
Angle dysgenesis is caused by incomplete development of the trabecular meshwork before and/or after birth. Strong monogenetic influence. Heredity shows recessive inheritance with variable penetrance in most cases or is sporadic. Specific chromosomal abnormalities have been identified at chromosomes 1p36 and 2q212.
Pathogenic mechanism:
Decreased aqueous outflow causes significant elevation of IOP. Isolated trabeculodysgenesis is the most common form of primary congenital glaucoma.
Epidemiology:
Congenital glaucoma occurs in about 1 in 12-18,000 births among Caucasians. Incidence can be 5 to 10 times higher if consanguinity of parents is present. Severe visual disability is common. PCG is more common in males (65%), and is bilateral in 70% of patients.
Symptoms:
Crying unhappy child during first weeks or year of life. Not always symptomatic.
Signs:
Photophobia, tearing, blepharospasm, and eye rubbing are typical early signs.
Eyes are larger compared to age, with corneal diameter usually >10.5 mm at birth and >12 mm in the first year of life. Axial length is increased, >20 mm at birth or >22 mm after 1 year. Corneal oedema is frequent; epithelial and stromal oedema can de associated with ruptures of Descemet’s Membrane, or Haab’s striae, not to be confused with forceps delivery trauma.
IOP can sometimes be measured in the awaked child with hand-held tonometers. Under general anesthesia the level of IOP is often artificially lowered by sedation and anesthetic medications: IOP values alone are insufficient to confirm the diagnosis unless IOP is extremely elevated and confirmed by corneal signs. Severe cases show extremely extended globe when the diagnosis is delayed, described as “buphthalmos” (Ox eye). A useful approach is to compare the width of the palpebral apertures.
The optic nerve head shows pressure distension or uniform cup enlargement in newborns; cupping is a typical signs for later stages (CDR >0.3). Optic disc signs may be reversible with the normalization of IOP.
Gonioscopy shows anterior insertion of the iris, forming a scalloped line with persistent uveal tissue and poorly differentiated structures and/or trabeculodysgenesis often described as Barkan´s “membrane”.
Treatment:
Initial surgery is indicated in nearly all cases with primary congenital glaucoma 2-5 [I,D]. Classical initial surgery is goniotomy or trabeculotomy1, 6-8. 360° trabeculotomy using a catheter to open the whole circumference of Schlemm’s canal has been described with favourable results9-11. Filtration surgery may be indicated if these are unsuccessful [I,D]. Repeat surgery is relatively frequent.
Medical treatment is usually neither effective nor practicable in the long term. Medications, including oral CAIs can be used while decision is made on a surgical approach and for eyes where surgery fails to achieve IOP control.2. Cycloablation is an intermediate or add-on procedure when primary trabecular surgery has failed. Severe cases and secondary childhood glaucomas, particularly aphakic childhood glaucoma, sometimes need long-tube drainage device surgery.
Cases with later manifestation usually do not have enlargement of the globe and may have a more favourable outcome with surgery.
2.1.2 Late-onset childhood open-angle glaucoma/Early Juvenile (onset >2 to puberty)
Etiology and pathophysiology: as in PCG, except :
– no ocular enlargement
– no congenital ocular anomalies or syndromes
– asymptomatic until field loss advanced
Signs:
open angle, elevated IOP, optic nerve and visual field damage depending on the stage of disease
Treatment:
See above 2.1.1.1
The treatment of pediatric glaucoma cases is particularly challenging due to the nature of the disease and to the intrinsic difficulties in operating them and in examining patients of this age. Treatment is to be adapted to the primary anomaly, and the mechanism of IOP elevation [I,D]. Whenever possible these cases should be referred to tertiary care centers.
2.1.3 Secondary Childhood Glaucoma
A variety of pathogenetic mechanisms are possible. A complete list and extensive discussion are outside the scope of the guidelines.
2.1.3.1 Glaucoma associated with non-acquired ocular anomalies
Axenfeld Rieger anomaly (Syndrome if systemic associations)
Peters anomaly (Syndrome if systemic associations)
Ectropion uveae
Congenital iris hypoplasia
Aniridia
Persistent fetal vasculature/PFV (if glaucoma present before cataract surgery)
Oculodermal melanocytosis (Nevus of Ota)
Posterior polymorphous dystrophy
Microphthalmos
Microcornea
Ectopia lentis
2.1.3.2 Glaucoma Associated with Non-acquired Systemic Disease or Syndrome
Chromosomal disorders such as Trisomy 21 (Down syndrome)
Connective tissue disorders
Marfan syndrome
Weill-Marchesani syndrome
Stickler syndrome
Metabolic disorders
Homocysteinuria
Lowe syndrome
Mucopolysaccharidoses
Phacomatoses
Neurofibromatosis (NF-1, NF-2)
Sturge-Weber syndrome
Klippel-Trenaunay-Weber syndrome
Rubinstein-Taybi
Congenital rubella
2.1.3.3 Glaucoma Associated with Acquired Condition
Uveitis
Trauma (hyphema, angle recession, ectopialentis)
Steroid induced
Tumors (benign/malignant, ocular/orbital)
Retinopathy of Prematurity
2.1.3.4 Glaucoma Following Childhood Cataract Surgery
Secondary glaucoma is a frequent serious complication after cataract surgery in early infancy. The incidence may increase up to 50% if cataract surgery is performed before the 9th month of life12, 13. This secondary glaucoma is difficult to treat and often needs long-tube drainage device surgery for long-term IOP control.
2.1.3.5 Treatment of secondary childhood glaucoma [I,D]
The management of these cases is particularly challenging.
Medical treatment is usually not effective nor practicable in long term. Medications, including oral CAIs can be used while decision is made on a surgical approach and in case of failed surgery while awaiting for further options.
Primary surgery: early goniotomy or trabeculotomy or filtration surgery may be indicated if these are unsuccessful. Repeat surgery is relatively frequent.
Treatment to be adapted to the primary anomaly, the mechanism of IOP elevation and the quality of life of the patient. These cases require highly specialized care.
2.2 - Primary Open-Angle Glaucomas
The open-angle glaucomas are chronic, progressive optic neuropathies, that have in common characteristic morphological changes at the optic nerve head and retinal nerve fibre layer in the absence of other ocular disease or congenital anomalies. Progressive retinal ganglion cells death and visual field loss are associated with these changes.
2.2.1 Epidemiology
Glaucoma is the second leading cause of blindness both in Europe and worldwide. It is the most frequent cause of irreversible blindness. POAG is unusual under the age of 50 yrs. Its prevalence increases with age14-25. However, the reported percentage largely depends on definition.
2.2.2 Risk factors for open-angle glaucoma
As most population studies did not differentiate between POAG and secondary open angle glaucomas such as pseudoexfoliation (PEX) glaucoma, the following statements apply to both varieties, here are labelled OAG.
Risk assessment
Consideration of risk factors is important: it helps to identify individuals who can be targeted for early detection and to guide management decisions about the initiation and escalation of treatment in established glaucoma patients.
Terminology
Risk Factors: risk factors for open-angle glaucoma (OAG) are those statistically associated with the development of OAG or conversion from ocular hypertension to glaucoma26.
Prognostic Factors: prognostic factors for OAG are statistically associated with the progression of established OAG. Neither risk factors nor prognostic factors establish causation. Sometimes the terms risk factors and prognostic factors are used interchangeably.
Predictive Factors: the term predictive factors should be used for factors which are associated with increased risk for glaucoma and which are part of the definition of OAG, such as optic disc parameters and visual field indices.
2.2.2.1 Risk factors for the development of OAG (See FC V)
Initial evidence on potential risk factors for OAG has been provided by cross-sectional population-based studies. Firm conclusions on risk factors for the development of OAG can only be drawn by longitudinal population-based cohort studies27-30.
Age
Cross-sectional population-based studies have consistently reported that the prevalence of OAG increases dramatically with age14-17,19-25,31. Longitudinal population-based studies have confirmed that older age is an important risk factor for OAG27-30. Two studies reported a 6% and 4% increased risk per year of age at baseline of developing OAG.
Intraocular pressure (IOP)
Higher IOP has been consistently associated with the prevalence14-17,19-25,31 and incidence of OAG27,28,30,32. According to longitudinal data, the risk of developing OAG increases by 11-12% in Caucasians27,28, 10% in people of African origin32 and 18% in Latinos30 for each 1 mmHg increase in IOP. To date, IOP is the only modifiable risk factor for OAG.
Race/ethnicity
The prevalence of glaucoma is several times higher in African-Americans and Afro-Caribbeans than in Caucasians18,33,34. In Latinos, it has been shown that the prevalence20-23 and incidence35 of OAG is higher than in Caucasians, but lower than in Afro-Caribbeans.
Family history of glaucoma
Two studies studying different ethnic groups found that the risk of having OAG was 9.2-fold and 4 fold higher, respectively for individuals having a first-degree relative with confirmed OAG, compared with those who did not 36, 37. Also, self– reported family history of glaucoma has been associated with increased risk of developing OAG27,29.
Pseudoexfoliation
Population-based studies which specifically assessed pseudoexfoliation and pseudoexfoliative glaucoma have consistently reported that pseudoexfoliation is associated with increased prevalence of OAG19,24,38-47. Based on longitudinal data, the presence of pseudoexfoliation is associated with an 11.2-fold increased risk of developing OAG27.
Central corneal thickness (CCT)
In two population based studies, there was a 41% and 30% increased risk of developing OAG per 40 μm thinner CCT29,48.
Myopia
Several cross-sectional population-based studies identified moderate to high myopia (greater than -3 diopters) as a factor associated with increased OAG prevalence47,49-55. A Dutch study showed that subjects with high myopia (greater than -4 D) had a 2.3-fold increased risk for developing OAG28. Latinos in California had a risk of OAG increased by 48% with each 1 mm increase in axial length30.
Ocular perfusion pressure
The association of low ocular perfusion pressure with increased OAG prevalence has been a consistent finding in population-based studies20,31, 56-61. Recent evidence suggests that this association may depend on whether subjects are treated for systemic hypertension or not29,56,58,61-66.
A phenotype characterized by vascular dysregulation has been described64. The Barbados Eye Study confirmed that low ocular perfusion pressure increases the risk for the development of OAG29.
Because of our limited understanding of this complex variable and of its interaction with potential risk factors for glaucoma, the exact place of ocular perfusion pressure in glaucoma management remains unclear67-69.
Other factors
There have been reports on other factors that may be associated with increased risk for OAG, such as diabetes, systemic blood pressure, migraine, Raynaud syndrome and obstructive sleep apnoea. However, data from the literature are inconsistent.
Risk factors by type of OAG
In general, population-based studies analyses have not differentiated between types of OAG. A recent analysis which considered POAG and PEX glaucoma revealed that IOP was the only factor associated with both of them; vascular systemic diseases and their treatment were associated only with POAG47. This may suggest differences in pathogenesis between these two common types of OAG.
2.2.2.2 Risk factors and predictive factors for the conversion of ocular hypertension to POAG
The Ocular Hypertension Treatment Study (OHTS), and the European Glaucoma Prevention Study (EGPS)70 are two randomized controlled trials (RCTs) which evaluated the effect of IOP-lowering treatment on the conversion of ocular hypertension to POAG. The following risk factors and predictive factors were consistently reported in both the OHTS and the EGPS:
Age (risk increased by 26% per decade)
IOP (risk increased by 9% per 1 mmHg)
Vertical and horizontal cup-to-disc ratio (risk increased by 19% per 0.1 larger)
Pattern standard deviation (PSD) in the visual field (risk increased by 13% per 0.2 dB greater)
CCT (2.04 fold increased risk per 40 μm thinner)
Based on the pooled OHTS–EGPS predictive model, a quantitative calculator was developed to estimate the 5-year risk for the conversion of ocular hypertension to POAG71. This tool is available to the clinician and may help to discuss frequency of visits and possible treatment.
However, limitations should also be considered. Because the calculator was based on the OHTS and EGPS data sets, results may not apply to individuals < 40 years old, individuals who have untreated IOPs < 22 mmHg or who are not of Caucasian or of African origin. Also, the calculator does not take into account other factors associated with increased risk for glaucoma, such as family history of glaucoma and pseudoexfoliation. In addition, life expectancy issues should be addressed.
2.2.2.3 Prognostic factors for progression of OAG
Factors associated with the progression of established OAG have been identified by large RCTs: Early Manifest Glaucoma Trial (EMGT)72, Advanced Glaucoma Intervention Study (AGIS)73, Collaborative Initial Glaucoma Treatment Study (CIGTS)74, Collaborative Normal Tension Glaucoma Study (CNTGS)75.
Age
Older age is significantly associated with increased risk for the progression of OAG. In the EMGT, after a mean follow-up of 8 years, patients ≥ 68 years old had a 51% increased risk of progression compared to those who were younger72. In the AGIS the risk of progression increased by 30% with every 5 years increase in age73; in CIGTS the risk increased by 35% for every decade74. Also, in the untreated arm of the EMGT, progression was considerably faster in older than in younger patients76.
IOP
Most of the above RCTs suggest a positive effect of IOP reduction on the onset or progression of glaucomatous damage. In the EMGT the risk of progression decreased by about 10% with each mmHg of IOP reduction from baseline to the first follow-up visit77. Conversely, the role of long term IOP fluctuation in glaucoma progression is still debated78-80. Also, the role of diurnal IOP fluctuation in glaucoma progression needs to be investigated more thoroughly in RCTs.
Pseudoexfoliation
In the EMGT, the risk of progression increased by a 2.12-fold in those with pseudoexfoliation compared with those without pseudoexfoliation72. In addition, in the untreated arm of the EMGT, progression was considerably faster in eyes with pseudoexfoliation, despite similar baseline IOP values between the pseudoexfoliative and non pseudoexfoliative eyes76. Pseudoexfoliation has not been evaluated in the AGIS, CIGTS and CNTGS.
CCT
In the EMGT, thinner CCT was a significant but weak prognostic factor for OAG and this association was observed only in patients with higher baseline IOP72. The role of CCT in glaucoma progression has not been evaluated in the AGIS, CIGTS and CNTGS.
Disc haemorrhages
In the CNTGS the presence of optic disc haemorrhages was significantly associated with glaucoma progression80. Also, in the EMGT patients with disc haemorrhages had significantly shorter time to progression81. A systematic review (January 1950-January 2013) evaluating risk factors for glaucoma among routine diagnostic examination reported disc haemorrhage (LR, 12; 95% CI, 2.9-48) being highly suggestive of glaucoma, but the absence of a haemorrhage was nondiagnostic (LR, 0.94; 95% CI, 0.83-0.98)82.

2.2.3 Primary Open-Angle Glaucoma
Definition:
Primary open-angle glaucoma (POAG) is a chronic progressive optic neuropathy with characteristic morphological changes at the optic nerve head and retinal nerve fibre layer in the absence of other ocular disease or congenital anomalies. Progressive retinal ganglion cell death and visual field loss are associated with these changes.
Etiology:
The etiology of primary open angle glaucoma remains unclear. Multiple genetic factors and the influence of co-morbidities are likely to play a role.
Pathophysiology:
The current concept of how damage is elicited includes deformation of the lamina cribrosa caused by IOP levels that are not tolerated by the individual eye. This is thought to result in axonal damage with consequent apoptotic death of the retinal ganglion cells. A substantial proportion of patients develop POAG at IOPs within the normal range. Any increase in IOP is caused by elevated outflow resistance in the trabecular meshwork outflow pathways.
Treatment:
POAG is treated by reducing intraocular pressure using medication, laser or incisional surgery (See Ch 3). So far, there is no evidence for other suggested treatment modalities, e.g. neuroprotection or modifying blood flow.
2.2.3.1 Primary Open-Angle Glaucoma / High Pressure Glaucoma (POAG/HPG)
The relative risk for POAG rises continuously with the level of the intra-ocular pressure (IOP), and there is no evidence of a threshold IOP for the onset of the condition. It is presumed that risk factors other than IOP have a relatively greater importance if there is glaucomatous optic neuropathy at the lower (statistically ‘normal’) pressure levels. POAG has been arbitrarily subdivided into High Pressure and Normal-Pressure disease to reflect this, even though they may represent a spectrum of optic neuropathies variably sensitive to the IOP. See Ch. Introduction.
Etiology:
Unknown
Pathomechanism:
Unknown.
TIGR and Myoc mutations may be associated83, 84.
Features:
Onset: from the young adult age onwards
Signs and symptoms:
Asymptomatic until field loss advanced
Elevated IOP without treatment (diurnal tension curve)
Optic nerve head: acquired characteristic glaucomatous damage and/or retinal nerve fiber layer changes (diffuse or localized defects) (See Ch. 1)
Visual field: usually detectable glaucomatous defects corresponding to the optic disc damage may be present
Gonioscopy: open anterior chamber angle (not occludable, no goniodysgenesis). (See Ch. 1).
Treatment:
Refer also to Introduction II and Ch. 3
A target pressure is to be identified for each case (See also Ch. 3.2 and FC IX-X) [I,D].
Medical treatment (See FC XI-XIII)
Mono therapy
Combination therapy as needed in selected patients
Laser trabeculoplasty (LTP)
Filtration Surgery with / without antimetabolites
Adjunctive medical therapy when needed
Insertion of aqueous long- tube drainage implants
Cyclodestructive procedures
Choice of primary therapeutic modality needs to be made on an individual patient basis [I,D].
Laser trabeculoplasty can be considered as primary treatment and as an alternative to additional medications [I,A].
2.2.3.2 Primary Open-Angle Glaucoma / Normal–Pressure Glaucoma (POAG/NPG)
Etiology:
Unknown
Pathomechanism:
Unknown.
Optineurin mutation has been found in families with NPG
Features:
Onset: from the 35th year onwards
Signs and symptoms:
Normal IOP without treatment (diurnal curve or 24-hour phasing). Asymptomatic until field loss advanced
Optic nerve head damage typical of glaucoma
Disc haemorrhages
Visual field defects typical of glaucoma; e.g. paracentral defects
Gonioscopy: open anterior chamber angle (exclude intermittent angle-closure; See Ch. 2)
No history or signs of other eye disease or steroid use.
Consider central corneal thickness if findings do not match; CCT may be thinner than average (See Ch. 1.1).
Treatment:
Refer also to Chapter Introduction II, Ch. 3 and FC VI
There are few prospective clinical trials indicating clearly the advantages of treatment [I,A]. Target pressure: in most cases a peak IOP = 8 mm - 15 mm Hg on diurnal curve or a 30% IOP reduction from baseline (See Ch. 3.2) [I,D]
Medical therapy:
Any drug singly or in combination which is effective and tolerated, whose IOP lowering effect is sufficient to reach a maintain the target IOP [I,D]
Avoid medications with potential vasoconstrictive effects or with systemic hypotensive effects [II,D]
Oral calcium channel blockers are being investigated in selected patients by some investigators.
Laser trabeculoplasty [I,D]
Glaucoma Surgery:
In cases of progressive glaucomatous damage, in spite of maximal medical therapy or laser trabeculoplasty, or failure to reach target pressure [I,D]. Intensive postoperative care with bleb manipulation may be needed to maintain low IOPs [I,D]
Follow-up intervals, depending on the stage of disease and on the rate of progression, with examination of [II,D]:
Optic disc
Visual field
IOP
ONH and RNFL documentation
2.2.4 Primary Juvenile Glaucoma
Etiology: Unknown
Pathomechanism: Decreased aqueous outflow
Features:
Onset: beyond infancy, usually after puberty or early adulthood. Heredity: if familiar frequently dominant trait. Genes associated with primary juvenile glaucoma have been identified as MYOC and CYP1B1
Signs and symptoms:
No enlargement of the globe
Asymptomatic until field loss is advanced
Elevated IOP without treatment (diurnal tension curve)
Optic nerve head and RNFL: Diffuse damage typical, but any type of glaucomatous damage
Visual field: glaucomatous defects
Gonioscopy: wide open anterior chamber angle, often poorly differentiated
No congenital or developmental anomalies
Treatment [I,D] (See FC VI):
Medical therapy: any ef fective and well tolerated topical regimen. Pilocarpine causes fluctuating myopic shift, visual symptoms and headache particularly in the young and should be avoided.
Surgery: early surgery often required filtering procedure or trabeculotomy; consider antimetabolites.
Laser trabeculoplasty: not recommended due to poor and short-lived IOP lowering effect.
2.2.5 Primary Open-Angle Glaucoma Suspect (POAG)
Etiology:
Unknown
Pathomechanism:
Unknown
Features:
Visual field and/or optic disc and/or nerve fiber layer normal or suspicious, with at least one being suspicious
IOP can be normal or increased
Treatment [II,D] (See FC VI):
Risks and benefits of treatment need to be weighed against the risk of the development of glaucomatous disc damage. The risk of developing glaucoma increases with the number and strength of risk factors.
The indication for any form of therapy is relative
Medical therapy: any topical agent alone or in combination as long as well tolerated and effective
Avoid adjunctive medical treatment unless strictly needed
Laser trabeculoplasty: not usually indicated
Filtering operation: not indicated
Follow-up [II,D] at intervals of 6-12 months initially, to be increased if all parameters remain normal with examination of:
Optic disc
Visual field
IOP
ONH RNFL documentation initially and every 2-3 years
2.2.6 Ocular Hypertension (OH)
Etiology:
Unknown
Pathomechanism:
Unknown
Features:
Signs and symptoms:
IOP > 21 mm Hg without treatment
Visual field: normal
Optic disc and retinal nerve fibre layer: normal
Gonioscopy: open anterior chamber angle (exclude intermittent angle-closure. See Ch 2.4.2.2)
No history or signs of other eye disease or steroid use.
Other risk factors: none
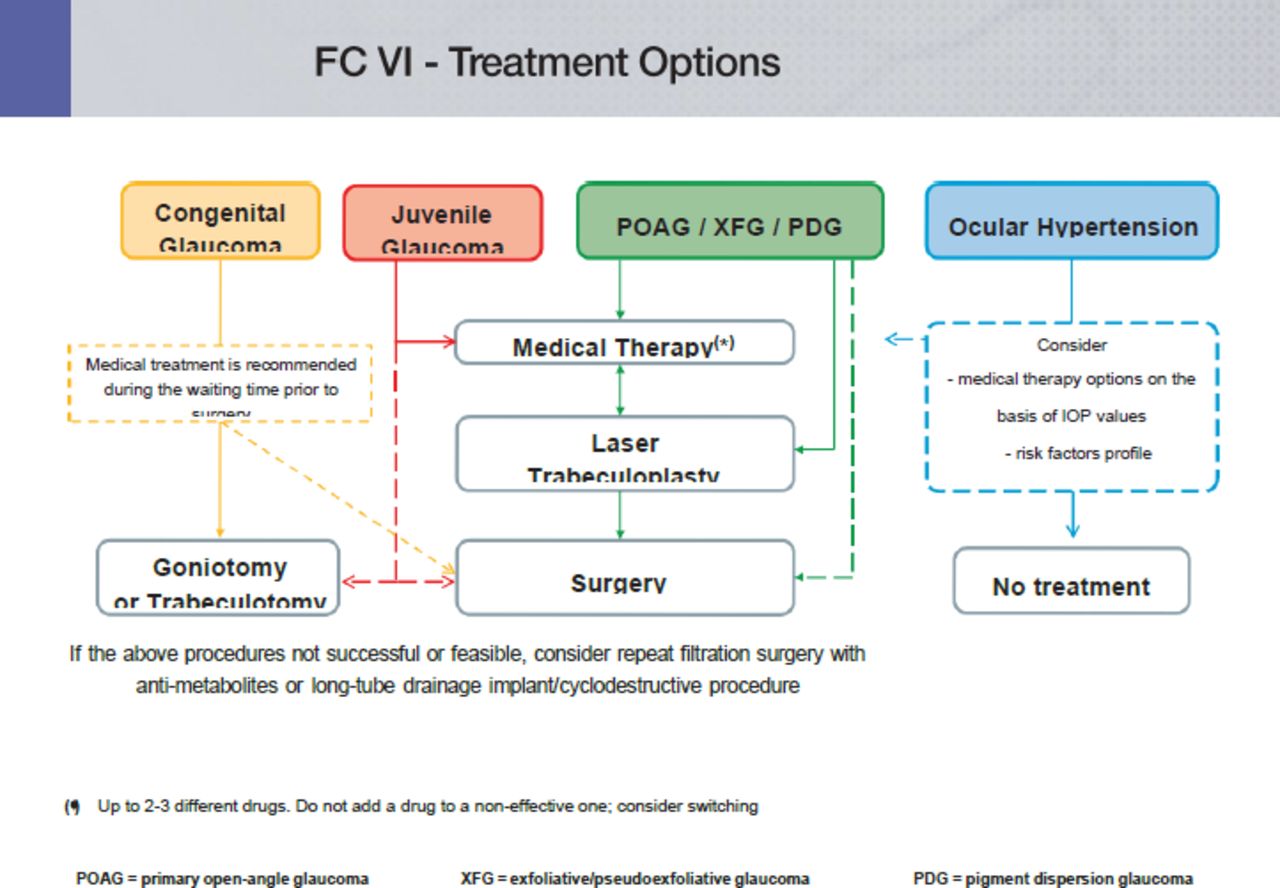
Treatment:
Although in the past it has been used as a diagnosis, Ocular Hypertension should be used to indicate that the IOP is consistently outside 2 or 3 standard deviations above the mean. Consider corneal thickness (See Introduction II and Ch. 1.1; FC II and IV).
A modest increase in IOP is not sufficient reason for treatment, but consider it in patients with repeated IOPs in the high twenties, even without risk factors. For treatment modality See Ch. 4.2.3-a (See also Ch. 2.2.3. and flow-charts).
If left untreated (See Ch. Introduction II)
up to 9.5% develop glaucoma over 5 year of follow-up
the risk of developing glaucoma increases with increasing IOP
prophylactic IOP-lowering therapy to be discussed with individual patients considering the presence of risk factors
Follow-up [II,D] at intervals of 12-24 months initially, to be increased if all parameters remain negative, with examination of:
Optic disc
Visual field
IOP
ONH and RNFL photographs initially and every 2-3 years
Patients for the ocular hypertension treatment study (Ch. Introduction II) were selected excluding myopes, labile diabetics, poor compliance. In most of Europe black Africans are a minority.
Assess each patient individually when deciding whether or not to treat [I,D].
2.3 - Secondary Glaucomas
Secondary glaucomas are a heterogeneous group of conditions, in which elevated IOP is the leading pathological factor causing glaucomatous optic neuropathy. Most forms of secondary glaucoma like uveitic or traumatic glaucoma have complex pathomechanisms including both an open or closed angle.
2.3.1 Secondary Open-Angle Glaucoma
2.3.1.1 Secondary Open-Angle Glaucomas Caused By Ocular Disease
2.3.1.1.1 Exfoliative (pseudoexfoliative) glaucoma
Features:
Onset: usually older than 60 years
Asymptomatic until visual field loss advanced
One or both eyes affected, often bilateral and asymmetrical
Etiology and pathogenic mechanisms.
Exfoliative glaucoma (XFG) develops from exfoliation (pseudoexfoliation) syndrome ( XFS), in which an abnormal f ibrillo-granular protein (exfoliation material) is produced in the eye and the body. Development of XFS is strongly associated with certain variants of the LOXL1 gene, but the onset of glaucoma may depend on other environmental and/or genetic factors. In the eye exfoliation material accumulates in a characteristic pattern on the anterior lens capsule, pupillary margin, trabecular meshwork and the zonules85, 86. Pigment granules from the posterior layer of the iris are liberated and together with the exfoliation material play an important role in the development of decreased aqueous humour outflow and elevation of IOP, which may lead to the development of glaucoma. Clinically both XFS and XFG may appear in only one eye, but they may develop gradually in the fellow eye in many cases. To identify exfoliation material pupil dilation is recommended. Typically XFG develops after 60 years of age, the IOP is considerably higher than that in POAG, and the diurnal IOP fluctuation is high. As a consequence, in the involved eye(s) optic nerve head damage and visual field deterioration are frequently severe already at the time of the first visit. At a population level, this may partially be counterbalanced by the fact that in certain countries XFG is significantly less undiagnosed than POAG87. In XFG the risk for progression is particularly high even when the eye is under IOP lowering treatment76. XFS and XFG are associated with poor pupil dilation and other ocular alterations like dense nuclear cataract and zonular damage which make cataract surgery more difficult and increase the risk for surgical complications86. Due to zonular damage lens dislocation and resulting secondary angle closure may occur.
Epidemiology:
XFG is the most common type of secondary open angle glaucomas, its prevalence varies considerably across populations24, 86. According to population-based data, XFG develops in approximately 15% to 26% of eyes with XFS (depending on the definition of glaucomatous damage) over a 5 year period27.
Also, it has been reported that XFS and XFG are associated with systemic diseases, particularly cardiovascular alterations88. However, there are recent reports which do not support this association47, 61, 89-91.
Signs and symptoms:
IOP: > 21 mm Hg, frequently higher than in average POAG cases. Visual field loss as in POAG; frequently severe at least in one eye.
Dandruff-like exfoliation material on the pupil border and on the surface of the anterior lens capsule except the central zone, better visualized after pupillary dilation. The pupillary collarette is irregular and typically has a moth-eaten appearance.
Pigmentary loss from the central or mid-iris and positive transillumination are possible. The angle can be open, narrow or closed; usually the TM is heavily pigmented with a blackish hue and dandruff-like particles and pigment granules may be seen in the lower angle recess.
When pigment accumulates along an ondulating line on or anterior to the Schwalbe’s line, this feature is called Sampaolesi’s line, which is pathognomonic of XFS.
Loose zonules are frequent with occasional phacodonesis, lens subluxation and more frequent complications during cataract surgery.
Narrow or closed-angle is relatively common.
Treatment:
Decrease the IOP with all medications, laser trabeculoplasty and filtering surgery used in the treatment of POAG. Usually XFG responds well to laser trabeculoplasty92 To achieve target IOP usually more medications are needed than in POAG. Due to the high diurnal IOP fluctuation, to characterize untreated baseline IOP and IOP under treatment several IOP measurements are necessary. When XFG is clinically unilateral the fellow eye must be also carefully followed because there is a high probability of development of XFG93.
2.3.1.1.2 Pigmentary glaucoma
Etiology:
Melanin granules cause an increase of trabecular meshwork outflow resistance and hence an elevation of IOP. The current understanding is that trabecular meshwork cells phagocytise pigment, which subsequently leads to their death94.
Pathogenic mechanism:
Melanin pigment is released from the iris pigmented epithelium as the result of rubbing between lens zonules and posterior surface of the iris. Posterior bowing of the iris with “reverse pupillary block” configuration is noted in many eyes with pigment dispersion95,96.
Three entities can be described:
Pigment dispersion syndrome (PDS) - ocular condition, usually bilateral characterized by dispersion of iris pigment
Pigmentary ocular hypertension (POH) - pigment dispersion syndrome with elevated IOP and without glaucomatous optic neuropathy
Pigmentary glaucoma (PG) - glaucomatous optic neuropathy and pigment dispersion syndrome
Epidemiology:
PG represents 1-1.5% of all glaucoma cases97. It is more common in Caucasian myopic men. It typically diagnosed at the age of 30-50 years. The risk of developing glaucoma in patients with PDS is 25 - 50%.
The estimated incidence of PDS and PG is 4.8/100 000 and 1.4/100 000 population per year respectively. The risk of developing pigmentary glaucoma from pigment dispersion syndrome is 10% at 5 years and 15% at 15 years98.
Symptoms:
Patients may experience transient visual blurring or halos during episodes of IOP rise, particularly after exercise or pupillary dilation, uncommonly associated with mild to moderate pain.
Signs:
PDS maybe either unilateral or bilateral. Signs of PDS or PG are very deep anterior chamber with backward bowing of the peripheral iris, midperipheral iris transilluminations with a radial spoke like pattern due to pigment loss best visible with retroillumination, pigment deposition on the iris surface and lens equator among zonular insertions, pigment deposition in the corneal endothelium typically accumulating vertically as a Krukenberg spindle. The presence of Krukenberg spindle is not necessary to make the diagnosis of PDS and may occur in other conditions such as exfoliation syndrome. Gonioscopy shows a homogenously dark brown, densely pigmented trabecular meshwork around 360° and pigment at or anterior to the Schwalbe's line, not to be confused with the Sampaolesi’s line of pseudoexfoliation; dim light in the examination room is recommended in order pupillary constriction and enhance gonioscopic observation of peripheral iris shape. Ultrasound biomicroscopy (UBM) can be helpful to confirm reverse pupillary block. PDS and PG can be independently combined with primary angle closure.
IOP is typically elevated with large fluctuations. Gradual decrease of IOP after 60 years of age has been reported99.
Treatment:
Medical treatment recommendations for PG are not different to that of POAG [I,D]. Pilocarpine is no longer a preferred drug, but if used, one should check the peripheral retina for tears [II,D].
Laser trabeculoplasty [I,C] is effective. However, the heavily pigmented trabecular meshwork warrants power settings lower than usual [I,D]. The initially good pressure fall may be lost over time. Repeat ALT is rarely successful100. c) Nd:YAG laser peripheral iridotomy (LPI) has been proposed as a means for eliminating reverse pupillary block (if present). The benefit from an LPI in patients with PDS and pigmentary ocular hypertension is not established101. d) Filtering procedures [I,D] are usually as successful as in POAG. Young myopic patients are at increased risk of hypotony maculopathy102.
Examination after exercise should be considered, especially when visual symptoms after exercises are reported. Increased pigment dispersion with posterior iris bowing during exercise is a sign of potentially progressing disease; in such patients; LPI may be considered103.
2.3.1.1.3 Lens-induced open-angle glaucoma
Etiology:
In lens induced open angle glaucoma trabecular meshwork outflow pathways are obstructed by lens particles and/or inflammatory cells104.
Pathogenic mechanism:
Phacolytic glaucoma: the trabecular meshwork is obstructed by lens material leaking from mature or hypermature cataract
Traumatic lens injury: the trabecular meshwork is obstructed by lens particles from a traumatically or surgically injured lens
Phacoanaphylactic glaucoma: lens proteins lead to granulomatous uveitis affecting the trabecular meshwork.
Sympathetic Ophthalmia: in rare cases uneventful cataract surgery in one eye can induce inflammation of the previously healthy contralateral eye leading to IOP spikes
Clinical features:
Patients usually suffer from unilateral pain with redness and inflammation. Reduced vision and elevated IOP. Signs of injured lens and/or mature/hypermature cataract or cataract surgery are present, with or without iritis (cf aqueous flare and keratic precipitates).
Treatment:
Extraction of lens or lens fragments followed by topical anti-inflammatory medication, vitrectomy if needed [I,D].
2.3.1.1.4 Glaucoma associated with intraocular haemorrhage
Etiology:
Either acute bleeding in the anterior chamber or long standing blood in the vitreous of any source can cause IOP elevation. Sickle cell trait / disease should always be considered because these patients may be at a higher risk for elevated IOP.
Pathogenic mechanism:
Large quantity of normal red blood cells (hyphaema) or haemoglobin-laden macrophages (haemolytic glaucoma) or degenerated red blood cells (ghost cell glaucoma) obstruct the trabecular meshwork.
Symptoms:
Pain and eye irritation.
Signs:
Elevated IOP is more common with larger hyphaemas and is more often due to recurrent haemorrhage or re-bleeding. Re-bleeding can follow traumatic hyphaema, usually after 3-7 days (incidence 5 - 10%). Patients with sickle cell disease / trait have an increased incidence of elevated IOP. They are also more prone to developing glaucomatous neuropathy and can be more difficult to treat105.
In haemolytic glaucoma red-tinged cells in the aqueous humour and reddish brown discoloration of the trabecular meshwork are present. “Ghost cells” occur 1 to 4 weeks after vitreous haemorrhage and reach the anterior chamber. Small khaki-coloured cells may be seen circulating in anterior chamber. Gonioscopic examination may show layering of the ghost cells over the inferior part of trabecular meshwork.
Treatment:
Topical and systemic IOP lowering medication as needed [I,D]. It is recommended to avoid carbonic anhydrase inhibitors and hyperosmotic agents in patients with sickle cell disease.
Conservative treatment, bed rest, topical cycloplegics and steroids, can be considered for uncomplicated hyphaema [II,D]. Antifibrinolytic agents such as tranexamic acid can reduce the risk if re-bleeding106. However it is not clear whether any of the interventions have an effect on visual acuity107.
Wash-out through a paracentesis of the anterior chamber [II,D] and/or vitrectomy for removing RBCs from vitreous if IOP remains high with the risk of causing corneal blood staining and/or optic neuropathy [II,D].
2.3.1.1.5 Uveitic glaucoma
Etiology:
Acute IOP elevation is typical in Posner-Schlossman syndrome or in viral infection such as HSV and VZV. Chronic IOP elevation is typical for Fuchs’ uveitis, juvenile idiopathic arthritis, Behcet disease, pars planitis, sympathetic ophthalmia, sarcoidosis and syphilis.
Pathogenic mechanism:
Obstruction and oedema of the trabecular meshwork are caused by inflammatory cells, precipitates, debris, secondary scarring and neovascularization of the chamber angle. Secondary angle-closure glaucoma can be due to synechial closure of the chamber angle or seclusio pupillae with subsequent appositional angle closure. Corticoid treatment can also contribute to IOP elevation108.
Symptoms:
Pain, redness, photophobia, decreased vision are possible.
Signs:
Features depend on the underlying cause. Elevated IOP; some forms are associated with wide oscillations or periodic rise in IOP.
Treatment [I,D]:
Topical and systemic anti-inflammatory therapy according to the underlying disease
Topical and systemic IOP lowering medication
traditionally topical -blockers and CAIs were used as first-line treatment.
prostaglandin analogues are used as first-line therapy in eyes with controlled uveitis. There are studies that support the efficacy and safety of prostaglandin analogues as IOP lowering medication in uveitic glaucoma109.
Glaucoma surgery suited for the type of inflammatory disease, ALT and SLT should be avoided110,111.
2.3.1.1.6 Neovascular Glaucoma
(See Secondary Angle Closure Glaucoma)
2.3.1.1.7 Glaucoma due to intraocular tumour
Etiology:
Reduced aqueous humour outflow due to primary or secondary intraocular tumours, mainly of the anterior segment.
Pathogenic mechanism:
Infiltration of the trabecular meshwork by the tumour or tumour cells floating in the aqueous humour. Trabecular meshwork obstruction due to tumour related inflammation, tumour debris, haemorrhage or pigment dispersion. Secondary angle closure glaucoma may also develop112.
Symptoms and signs:
Elevated IOP. A highly variable clinical picture, combining evidence of both tumour and glaucoma.
Treatment [I,D]:
Treatment of underlying tumour (irradiation, surgical tumour excision, enucleation)
Topical and systemic IOP lowering medication; medical therapy is often first-line treatment while awaiting definitive treatment:
topical -blockers, -agonists, topical and systemic CAIs are safe and effective
prostaglandin analogues (increasing uveoscleral outflow) and pilocarpine (increasing trabecular outflow) may theoretically promote metastasis
Cycloablation
Incisional glaucoma surgery indicated only after successful tumour therapy.
2.3.1.1.8 Glaucoma associated with retinal detachment
Etiology and pathogenic mechanism:
Long standing retinal detachment that leads to ischaemic neovascularization. Retinal detachment is usually associated with a reduction of IOP. Gas tamponade can elicit significant IOP spikes. Dispersed silicon oil may cause chronic IOP elevation.
The trabecular meshwork may be obstructed by neovascularization caused by proliferative retinopathy, or by scarring, pigment dispersion and inflammation, or by cellular debris from retinal cells outer segments (Schwartz’s syndrome). Surgery for retinal detachment can also cause glaucoma113.
Symptoms and signs:
Elevated IOP and retinal detachment are present. Redness and pain are common features.
Treatment [I,D]:
Topical and systemic IOP lowering medication
Surgery for retinal detachment
Consider glaucoma surgery
2.3.1.2 Open-angle glaucoma due to ocular trauma
Ocular trauma leads to glaucoma by several different mechanisms. The secondary traumatic glaucomas can be caused by both open-angle and angle-closure mechanisms. In order to identify and treat the causes of IOP elevation; careful evaluation of the ocular damage must be performed.
Etiology:
Blunt non-penetrating or penetrating trauma to the eye.
Pathogenic mechanisms:
Blunt non-penetrating trauma can lead to reduced trabecular outflow due to traumatic changes of the trabecular meshwork. Scarring and inflammation of the trabecular meshwork, obstruction by red blood cells and debris, angle recession, lens-induced glaucoma. Elevated IOP may occur a very long time after the trauma. Positive steroid response after anti-inflammatory treatment should also be considered. Penetrating injury may damage one or more intraocular structure leading to elevated IOP114.
Symptoms and signs:
Redness, pain, decreased vision with acute IOP elevation, or no symptoms with chronic IOP elevation. Acute or late IOP elevation (occurring months or even decades later) may follow blunt trauma.
Chemical burns, hyphaema, traumatic cataract, uveitis, angle recession, ruptured iris sphincter, iridodialysis can be present in various combinations.
Note: It is not recommended to perform gonioscopy in fresh ocular trauma to avoid compressing the eye. This examination can be delayed for several weeks.
Treatment [I,D]:
Anti-inflammatory
Topical and systemic IOP lowering medication
Long-term IOP follow up in the presence of permanent anterior segment damage.
Glaucoma surgery
2.3.2 Iatrogenic Secondary Open-Angle Glaucomas
2.3.2.1 Glaucoma due to corticosteroid treatment
Etiology:
Topical, intravitreal as well as high dose and long-term systemic corticosteroid therapy can induce acute or chronic IOP elevation115. The risk of IOP elevation depends on the chemical structure (strength) of the steroid, dose, frequency and duration of therapy, and route of administration. The risk factors for being steroid responder are: POAG, family history of glaucoma, diabetes, myopia, rheumatoid arthritis, children and elderly patients.
Pathogenic mechanism:
Corticosteroids induce changes in the trabecular extracellular matrix (glycoproteins) which lead to decreased outflow facility. A TIGR gene modification is present116.
Symptoms:
Pain and eye irritation are possible but not at all mandatory especially in acute IOP elevation.
Signs:
Elevated IOP usually develops 2 to 6 weeks after initiating therapy, but may occur at any time. Usually IOP elevation is slowly reversed after stopping the use of corticosteroid. Corneal oedema can be present. Prolonged IOP elevation can lead to typical glaucomatous optic nerve head changes and visual field damage.
Treatment [I,D]:
Discontinuation of corticosteroid therapy is recommended; steroid-sparing therapy of underlying condition should be considered. If this is not possible, consider switching to weaker steroid (e.g. loteprednol, fluorometholone)
Topical and systemic IOP lowering medication
Laser trabeculoplasty
Glaucoma surgery may be performed in intractable cases
2.3.2.2 Secondary open-angle glaucoma due to ocular surgery and laser
Ocular surgery can cause secondary open-angle glaucoma by some of the mechanisms discussed above: intraocular haemorrhage, inflammatory reaction, lens material, pigmentary loss from uveal tissue, or trauma117.
Pathogenic mechanism:
Open-angle glaucoma following ocular surgery or laser is a result of reduced trabecular outflow:
IOP elevation after intraocular surgery is usually transient. The elevated IOP may be caused by: viscoelastic material, inflammatory debris, vitreous in the anterior chamber after cataract surgery, lens particles, intra-operative application of -chymotrypsin, and prostaglandin release.
Acute onset secondar y IOP elevation af ter Nd:YAG laser i r idotomy, capsulotomy and laser trabeculoplasty. IOP elevation is usually transient, within the first 24 hours, most frequent in the first 4 hours after treatment.
IOP elevation with open- angle following vitrectomy with sil icon oil implantation develops as a result of:
Migration of silicon oil into anterior chamber and obstruction of the trabecular meshwork (early post-op IOP increase) usually due to overfill of oil.
Migration of emulsified silicon oil into anterior chamber with obstruction of trabecular meshwork where oil particles are partially phagocytised by macrophages and accumulate in the trabecular meshwork especially in the upper quadrant and can induce trabeculitis (intermediate and late onset IOP increase). Prolonged contact of silicon oil with the trabecular meshwork may cause permanent structural changes. Risk factors for developing IOP elevation following vitrectomy with silicon oil implantation include pre-existing ocular hypertension or glaucoma, diabetes mellitus, and aphakia (closed angle type)118,119.
Uveitis-glaucoma-hyphema (UGH) syndrome - IOP elevation associated with an anterior chamber intraocular lens due to induced iris root bleeding and anterior uveitis. Modern IOLs pose a significantly lower risk of inducing UGH syndrome.
Treatment [I,D]:
Topical and systemic IOP lowering medication
Anti-inflammatory treatment
Removal of silicone oil may be considered in eyes with IOP elevation secondary to silicon oil emulsification. However current data suggest that removal of silicon oil is not effective in all cases and the risk of re-detachment increases. Trans-scleral cyclophotocoagulation and aqueous drainage devices seem to represent more effective options, although the latter are associated with the r isk of silicon oil escape into sub- conjuctival space. Endoscopic cyclophotocoagulation in eyes requiring silicon oil removal and antiglaucoma treatment seems to be effective option. Conventional filtration surgery is associated with poor prognosis.
Removal of the intraocular lens may be needed in case of UGH syndrome
Glaucoma surgery according to the specific condition.
2.3.3 Secondary Open-Angle Glaucoma Caused By Extrabulbar Disease
2.3.3.1 Glaucoma caused by increased episcleral venous pressure
Etiology and pathogenic mechanism:
Episcleral, orbital or systemic diseases can cause the elevation of episcleral venous pressure with subsequent reduction of trabecular outflow and IOP elevation. The following disorders can be described:
Episcleral and orbital causes: chemical burn or radiation damage of the episcleral veins, hemangioma in Sturge-Weber syndrome, Nevus of Ota, endocrine orbitopathy, orbital (retrobulbar) tumor, pseudotumor, orbital phlebitis, orbital or intracranial arteriovenous fistula
Neurologic conditions: dural shunts, cavernous sinus thrombosis
Other systemic causes: superior vena cava obstruction, jugular vein obstruction (radical neck dissection), pulmonary venous obstruction
Idiopathic forms
Symptoms and signs:
IOP elevation can be acute with eye irritation and pain. Visual acuity can be decreased. Dilated, congested episcleral veins, chemosis, facial lymphedema, orbital bruit can be present. Vascular bruits are characteristic signs of A/V fistulae120
Treatment [I,D]:
Treatment of the underlying disease
Topical and systemic IOP lowering medication
Glaucoma surgery
2.4 - Primary Angle-Closure
Scientific publications on angle-closure have suffered from the lack of a uniform definition and specific diagnostic criteria. Only in recent years has there been recognition of the need to standardize definitions of the various types.
Angle-closure is defined by the presence of iridotrabecular contact (ITC). This can be either appositional or synechial. Either can be due to any one of a number of possible mechanisms. Angle closure may result in raised IOP and cause structural changes in the eye. Primary angle-closure (PAC) is defined as an occludable drainage angle and features indicating that trabecular obstruction by the peripheral iris has occurred. The term glaucoma is added if glaucomatous optic neuropathy is present: Primary angle-closure glaucoma (PACG). The main reason to distinguish Primary angle-closure glaucoma from Primary open-angle glaucoma is the initial therapeutic approach (i.e. iridotomy or iridectomy) and the possible late complications (synechial closure of the chamber angle) or the complications resulting when this type of glaucoma undergoes filtering surgery (uveal effusion, cilio-lenticular block leading to malignant glaucoma)121,122.
The prevalence of primary angle closure glaucoma (PACG)
Ethnic background is one of the major factors determining susceptibility to primary angle-closure (PAC). Population surveys show that PAC is more common among people of Asian descent than those from Europe. Among people aged 40 years and over, the prevalence of PAC ranges from 0.1% in Europeans123,124 through 1.4% in East Asians123,124 and up to 5% in Greenland Inuit125. Of those over 40 years old in European derived populations, 0.4% are estimated to have PACG. Three-quarters of cases occur in female subjects. There are 1.60 million people in Europe and 581 000 people in the USA with PACG126.
Primary glaucoma cases should be examined and the anterior chamber angle shown to be open on gonioscopy before PACG is excluded127.
Provocative Tests
In general provocative tests for angle-closure provide little additional information since even when negative they may not rule out the potential for angle-closure. In addition they may be hazardous, triggering an acute angle-closure attack even while the patient is monitored.
2.4.1 Primary Angle-Closure (PAC)
Angle-closure is defined by the presence of iridotrabecular contact (lTC). Gonioscopy remains the standard technique for identifying ITC. Primary angle-closure (PAC) results from crowding of the anterior segment, and as such, usually occurs in eyes with smaller than average anterior segment dimensions. Pathological angle-closure is defined by the presence of ITC combined with either elevated intraocular pressure (IOP) or peripheral anterior synechiae (PAS), or both. The absence of ocular diseases which may induce the formation of PAS such as uveitis, iris neovascularisation, trauma and surgery, defines primary angle-closure. Additionally, angle- closure resulting from the action of forces at the level of the lens or behind the lens is usually regarded as secondary (i.e. cataract, massive vitreous haemorrhage, and silicone oil or gas retinal tamponade) as the successful management is aimed at the underlying lens or posterior segment pathology. Angle-closure may impair aqueous outflow through simple obstruction of the trabecular meshwork (TM), or by causing irreversible degeneration and damage of the TM.
2.4.1.1 Natural History of PAC
PAC becomes more likely as the separation between the iris and TM decreases128. The risk of iridotrabecular contact in a “narrow” angle begins to increase once the iridotrabecular angle is ≤ 20°129. With angles of 20° or less, signs of previous angle-closure, such as PAS or iris pigment on the TM, should be carefully sought as signs of previous closure. Most angle- closure occurs asymptomatically. Although symptoms of pain, redness, blurring of vision or haloes may help identify people with significant angle-closure, the sensitivity and specificity of symptoms for identifying angle-closure are very poor. The most commonly identified sign which indicates that treatment is required is ITC. There is not a precise extent of gonioscopically evident ITC which will dictate the indication to treatment for all cases.
An international group of experts reached a consensus that 2 quadrants or more of ITC is an indication for prophylactic treatment130 [II,D].
Clearly, in established disease with high IOP, established PAS or glaucomatous optic neuropathy, any potential for angle-closure should be considered and treated on individual merits.
2.4.1.2 Staging of Primary Angle-closure123
Primary Angle-closure Suspect (PACS)
Two or more quadrants of iridotrabecular contact (lTC), normal IOP, no PAS, no evidence of glaucomatous optic neuropathy (GON).
Primary Angle-closure (PAC)
Iridotrabecular contact resulting in PAS and/or raised IOP. No evidence of GON.
Primary Angle-closure Glaucoma (PACG)
Iridotrabecular contact causing GON; PAS and raised IOP may be absent at the time of initial examination.
2.4.1.3 Ocular Damage in Angle-closure
Primary angle-closure (PAC) may cause ocular tissue damage in many ways. Corneal endothelial cell loss occurs after symptomatic “acute” angle-closure. With very high IOP values the iris may suffer ischaemic damage to musculature causing iris whirling (distortion of radially orientated fibres) and/or a dilated, unresponsive pupil. The lens epithelium may suffer focal necrosis causing anterior sub-capsular or capsular opacity of the lens associated with focal epithelial infarct called “Glaukomflecken”. The trabecular meshwork can be damaged by the formation of PAS, or as the result of long- standing appositional closure. Optic neuropathy in angle-closure may manifest in at least 2 ways. After an “acute” symptomatic episode, the disc may become pale but flat, suggesting an anterior ischaemic optic neuropathy. Typical glaucomatous optic neuropathy manifests in with an excavated surface and a pattern of visual field loss indistinguishable from open-angle glaucoma. Angle-closure accounts for 50% of all glaucoma blindness worldwide, and is probably the most visually destructive form of glaucoma.
2.4.1.4 Outcome following treatment
In asymptomatic (“chronic”) angle-closure, a high presenting pressure (>35 mmHg), more than 6 clock hours of peripheral anterior synechiae and/or established glaucomatous optic neuropathy are signs that a case of angle-closure will not respond fully to a laser iridotomy131, and that a trabeculectomy may be needed to control pressure” [II,D].
2.4.1.5 Mechanisms of angle-closure
It is important to identify secondary causes of narrow or closed-angles, such as phakomorphic, uveitic and neovascular cases, as the management of these cases is initially directed at controlling the underlying disease. In isometropic eyes it is helpful to compare axial anterior chamber depths of the two eyes. Asymmetry of > 0.2 mm (3 standard deviations) is suggestive of a secondary pathological process. A-mode or ultrasound biomicroscopy may be helpful in measuring axial dimensions (Iength, AC depth and lens thickness) and defining anatomical relationships. In primary angle-closure these will be the same in each eye. Mechanisms responsible for angle- closure are described in terms of anatomical location of obstruction to aqueous flow, successively, at the pupil, the iris and ciliary body, the lens and behind the lens. This is also order of decreasing frequency of each mechanism. Two mechanisms may co-exist, especially levels I and II (i.e. pupil and iris/ciliary body). Often, one mechanism predominates.
Pupillary block mechanism
Pupillary block is the predominant mechanism in around 75% of cases of primary angle-closure. Pupillary block is an exaggeration of a physiological phenomenon in which the flow of aqueous from the posterior chamber through the pupil to the anterior chamber is impeded causing the pressure in the posterior chamber to become higher than the pressure in the anterior chamber. As a result, the peripheral iris bows forward and comes into contact with the trabecular meshwork and/or peripheral cornea.
In a minority of cases, this becomes a self-perpetuating cycle with obstruction of trabecular outflow leading to a rise in IOP up to 50-80 mmHg. When total trabecular obstruction occurs rapidly (within a few hours), it causes the symptoms and signs of acute angle-closure (AAC).
The increased resistance to trans-pupillary aqueous flow is believed to result from co-activation of both sphincter and dilator muscles, causing the pupil margin to grip the anterior surface of the lens. This may occur in response to physiological stimuli, such as reading in poor light, or pharmacologically, such as with miotic therapy and concomitant dilator muscle stimulation by phenylephrine (the Mapstone provocation test)132. In most cases, the predisposition to pupil block is created by a narrow anterior segment and the age-related increase of lens volume (See Ch. 2.5.1 and 2.5.3).
The prevalence of PAC is higher in elderly people women and in some races (especially East Asians). There is a weaker association with hypermetropia, exfoliation syndrome, diabetes and retinitis pigmentosa.
Anomalies at the level of the iris and/or ciliary body (“plateau iris configuration”)
This group of anterior, non-pupil-block mechanisms are sometimes erroneously referred to under the umbrella term “plateau iris”. They are the result of variations in iris and ciliary body anatomy that brings the peripheral iris into contact with the trabecular meshwork. These include a thicker iris, a more anterior iris insertion and a more anterior ciliary body position. These anatomical factors predict failure of a laser iridotomy to open an appositionally closed angle133.
Anteriorly positioned ciliary processes cause “typical” plateau iris configuration134. Plateau iris “syndrome” should be differentiated from plateau iris configuration. The “configuration” refers to a situation in which the iris plane is flat and the anterior chamber is not shallow axially. In most cases, the angle-closure glaucoma associated with the plateau iris configuration is cured by a peripheral iridectomy. “Plateau iris syndrome” refers to a post-laser condition in which a patent iridotomy has removed the relative pupillary block, but gonioscopically confirmed angle closure recurs without shallowing of the anterior chamber axially. Plateau iris syndrome is rare compared to the configuration, which itself is not common. It usually occurs in a younger age group than pupillary-block angle-closure. The treatment is laser iridoplasty or the long-term use of pilocarpine postoperatively as long as it is needed [II,D]. This syndrome must be considered in the differential diagnosis when the intraocular pressure rises unexpectedly following an adequate peripheral iridectomy procedure for angle-closure glaucoma135.
Ideally, treatment should be instituted before synechial closure of the angle occurs [II,D]
Anomalies at the Level of the Lens
The most widely recognised risk factor for primary angle-closure is a shallow anterior chamber. The anterior surface of the lens marks the depth of the anterior chamber, and as such, PAC patients typically have a thicker, more anteriorly positioned lens than people with wide open angles. Nuclear sclerotic cataract is a frequent finding in primary angle-closure. If a separate pathological or iatrogenic process causes the lens to suddenly increase in thickness (e.g. “classic” diabetic or post-traumatic cataract), become more anteriorly positioned (retinal gas or oil tamponade) or subluxate (Marfan syndrome or trauma), this may cause secondary angle-closure (See Ch. 2.5.1 and 2.5.3).
Anomalies posterior to the Lens (Aqueous misdirection syndrome)
In rare cases, aqueous misdirection can complicate the management of primary angle-closure. This may occur following trabeculectomy, lens extraction, laser iridotomy and other surgical procedures. Forward movement of the lens iris diaphragm causes secondary angle-closure resulting in IOP elevation. These cases, typically have very small eyes (axial length <21 mm) and higher hypermetropic refraction (> +6D). It is believed that the ciliary processes come into contact with the lens equator, and/or a firm zonule/posterior capsule diaphragm, causing misdirection of aqueous into the vitreous135, 136. As a consequence, the lens/iris diaphragm is pushed forward and occludes the anterior chamber angle. After iridotomy or iridectomy, the use of miotics raises the IOP, whereas the use of cycloplegics reduces the IOP. This ‘inverse’ or ‘paradoxical’ reaction to parasympathomimetics should be tested only after iridotomy has been performed. Ultrasound biomicroscopy can demonstrate abnormal posterior chamber anatomy in these rare cases (See Ch. 2.5.3).
Asymmetry of anterior chamber depth is a cardinal sign of secondary (types III and IV) angle-closure.
Systemic drugs and angle-closure
Systemic drugs which may induce angle-closure in pre-disposed individuals are: nebulised bronchodilators (ipratropium bromide and/or salbutamol), selective serotonin re-uptake inhibitors (SSRI’s), tricyclic antidepressants, proprietary cold and flu medications, muscle relaxants, anti-epileptics (topiramate) and other agents with a parasympatholytic and sympathomimetic action137.
2.4.1.6 Demographic risk factors for Primary Angle-Closure135,138
Older age
Female
Asian and Eskimoan Race
Family history if primary angle-closure: family screening is vital in these families as robust evidence now exists for significant increased risk of angle closure in family members of an affected patient: first degree relatives may have a 1 in 4 risk of a PAC disease requiring treatment139.
2.4.1.7 Descriptions of subtypes:
Primary angle-closure has previously been divided into 5 clinical subtypes according to mode of presentation. There is debate on whether this approach to classification is useful in determining the prognosis or optimal management.
Primary Angle-Closure Suspect (PACS)
Acute Angle-Closure (AAC)
Intermittent Angle-Closure (IAC)
Chronic Angle-Closure Glaucoma (CACG)
Status Post-Acute Angle-closure Attack
2.4.1.7.1 Primary Angle-Closure Suspect (PACS) or “occludable” angle
Etiology and pathomechanism:
Pupillary block or plateau iris configuration; each component plays different roles in different eyes (See Ch. 2.4.1.5).
Features:
Signs:
Two or more quadrants of iridotrabecular contact (lTC)
Normal IOP
No peripheral anterior synechia (PAS)
No evidence of glaucomatous optic neuropathy (GON)
No glaucomatous visual field defect
The fellow eye of a documented non-secondary angle-closure is considered capable of occlusion.
Treatment:
PACS or “occludable angle” is a clinical assessment. Whether to treat or not is the responsibility of the ophthalmologist. There is not a precise extent of gonioscopically evident ITC which will dictate the indication to treatment for all cases.
If a PAC suspect has narrow angle with two or more quadrants of ITC but no synechial angle closure, the treatment to offer the patient is laser peripheral iridotomy (LPI) followed by argon laser peripheral iridoplasty (ALPI) in cases with plateau iris configuration [II,D].
The same applies to fellow eyes of primary angle-closure [I,C]. All cases must be assessed individually [I,D]. In general, the risks of treatment are to be balanced against the perceived risk of angle-closure.
2.4.1.7.2 Acute Angle-Closure (AAC) with pupillary block mechanism
Etiology:
Circumferential iris apposition to the trabecular meshwork with rapid and excessive increase in IOP that does not resolve spontaneously.
Pathomechanism: See Ch. 2.4.1.5
Features:
Signs:
IOP >21 mmHg, often to 50-80 mmHg.
Decreased visual acuity
Corneal oedema, initially mostly epithelial oedema. Shallow or flat peripheral anterior chamber
Peripheral iris pushed forward and in contact with Schwalbe’s line. Gonioscopy: iridotrabecular contact 360°
Pupil mid-dilated and reduced or no reactivity
Venous congestion and ciliary injection
Fundus: disc oedema, with venous congestion and splinter haemorrhages, or the disc may be normal or show glaucomatous excavation
Bradycardia or arrhythmia
Gonioscopy clues from the other eye Symptoms:
Blurred vision, “halos” around lights
Pain
Frontal headache of variable degree on the side of the affected eye
Nausea and vomiting, occasionally
Palpitations, abdominal cramps, occasionally
Treatment options:
See also flowchart FC VII-VIII
Medical treatment
Laser peripheral iridotomy (LPI)
Argon Laser Peripheral Iridoplasty (ALPI)
Lens Extraction
Trabeculectomy
Anterior Chamber Paracentesis
Goniosynechialysis (GSL)
Iridotomy or iridectomy together with medical treatment is the preferred definitive treatment of acute angle-closure glaucoma with a pupillary block component [I,D]
A: Medical Treatment [I,D]
Medical treatment serves to lower IOP, to relieve the symptoms and signs so that laser iridotomy or iridectomy is possible
Medical therapy aims for
withdrawal of aqueous from vitreous body and posterior chamber by hyperosmotics
pupillary constriction to open the chamber angle
reduction of aqueous production reduction of inflammation.
All the above steps of medical therapy should be implemented concurrently [I,D]
Consider contraindications to each of the medications to be used
Reduction of aqueous production
acetazolamide 10 mg/Kg intravenously or orally. Topical carbonic anhydrase inhibitors (CAls) are not potent enough to break the pupillary block
topical alpha-2 agonists
topical beta-blockers
Dehydration of vitreous body
Hyperosmotics are the effective agents but carry significant systemic risk in some patients: patients must be evaluated for heart or kidney disease because hyperosmotics increase blood volume which increases the load in the heart [IID]. Glycerol may alter glucose blood levels and should not be given to diabetics (FC VII) [I,D]
- glycerol 1.0 - 1.5 g/Kg orally
- mannitol 1.0 - 1.5 g/Kg intravenously
Pupillary constriction [I,D]
pilocarpine 1% or 2% or aceclidine 2% twice or three times within 1 hour Note: while the sphincter is ischaemic and the pupil non-reactive to light for sphincter paresis, multiple applications of topical parasympathomimetics is not helpful, will not cause pupillary constriction and may cause forward rotation of the ciliary muscle, thereby increasing the pupillary block. Since miotics in large doses can cause systemic side effects due to trans-nasal absorption leading to abdominal spasms and sweating, intensive topical parasympathomimetics are no longer indicated to treat this condition.Miotics are likely to constrict the pupil only after IOP has been lowered.
dapiprazole 0.5%
Alpha-1 blockers relax the dilator muscle. They do not reduce pupil size when the sphincter-muscle is paretic.
Reduction of inflammation
Topical steroid every 5 minutes for three times, then 4-6 times daily, depending on duration of raised IOP and severity of inflammation.
B: Surgical Treatment
Neodymium YAG laser iridotomy
Laser iridotomy should be attempted if the cornea is sufficiently clear [I,C]. Argon laser iridotomy is rarely performed nowadays but thermal laser pre-treatment (e.g,. argon) of dark irides reduces total YAG energy required127 [II,B]
Surgical iridectomy
Transcorneal approach.
Advantages:
– No conjunctival scarring
– A water-tight self-sealing incision is possible
Disadvantages:
– Technically more difficult in dilated fixed pupil and flat anterior chamber
– More traction an iris with increased risk of haemorrhage
Corneoscleral approach
Advantages:
– Iridectomy can be basal
Disadvantages:
– Conjunctival wound may lead to scarring compromising the outcome of a filtering procedure which may become necessary at a later stage insufficient wound closure and aqueous misdirection may occur in rare cases
General advantages of surgical iridectomy:
– It can be performed even when the cornea is cloudy
– It allows deepening of the anterior chamber, breaking freshly formed PAS
– General disadvantages of surgical iridectomy:
– All the potential risks of any intraocular procedure in an eye with angle closure
C: Argon Laser Peripheral Iridoplasty (ALPI)
There is now some evidence from randomised controlled trials that ALPI can break an attack of acute angle closure as or more swiftly than medical therapy140. Many glaucoma specialists now routinely use ALPI if topical treatment + acetazolamide have not broken an attack within an hour, prior to considering hyper-osmotics. ALPI is also a useful procedure to eliminate appositional angle closure resulting from mechanisms other than pupillary block (i.e: plateau iris configuration)141.
Diode Laser Peripheral Iridoplasty has greater penetration of an oedematous cornea but has been less extensively studied.
Anterior chamber paracentesis is being evaluated to break the attack in cases that are refractory to medical management142.
D: Lens extraction See FC VII
Clinical reports of phacoemulsification with posterior chamber intraocular lens implantation in the treatment of acute, chronic, and secondary angle-closure +/- glaucoma describe very favourable results. The appropriate role for lensectomy in the management of primary angle closure, however, still remains unproven. The first case-series study showed that cataract extraction was associated with a good reduction in IOP and a reduction in the number of medications required to control IOP143.
A few prospective case series or randomized clinical trials have been performed143-146 or are ongoing147 to determine the value and comparative risks and efficacy of lens surgery, both clear lens extraction and cataract surgery, versus medical therapy, laser peripheral iridotomy, laser iridoplasty, and filtration procedures for the treatment of acute and chronic primary angle closure and for the prevention of chronic angle-closure glaucoma, both after and instead of laser peripheral iridotomy. Cataract surgery in PACG is generally more challenging and prone to complications than in normal eyes or eyes with POAG because of the shallow AC, larger lens, corneal oedema, poorly dilated or miotic pupil, extensive posterior synechiae, lower endothelial cell count, weaker zonules, especially after an acute angle closure attack.
In an eye with a clear lens: laser PI first. If the angle does not open and IOP not well controlled with unquestionable glaucomatous damage, consider to proceed with phacoemulsification and IOL implantation [I,D].
E: Trabeculectomy
Trabeculectomy in chronic PACG is also associated with higher risk of postoperative anterior chamber shallowing, malignant glaucoma, and a significant rate of cataract formation compared to POAG137. Even when filtration surgery has successfully reduced the IOP, the ailing trabecular meshwork does not regain its function, and so the disease is not cured.
Combined lens extraction and trabeculectomy
In a study in CACG eyes with coexisting cataract, combined phacotrabeculectomy resulted in significantly more surgical complications than phacoemulsification alone. Visual acuity or disease progression did not differ between the 2 treatment groups148.
F: Anterior Chamber Paracentesis139, 142
Rapidly lowers IOP in APAC
Instantaneous relief of symptoms
Prevention of further optic nerve and trabecular meshwork damage secondary to the acutely elevated IOP
The IOP-lowering benefit may decrease by 1 hour after the procedure
Anti-glaucoma medications are necessary to maintain IOP control.
Paracentesis will not directly break the pupillary block but can allow the cornea to clear permitting to perform LPI
Possible complications include
Excessive shallowing of the anterior chamber
Puncture of iris, lens
Choroidal effusion
Haemorrhage due to the sudden decompression
G: Goniosynechialysis138
Often performed with other procedures such as lens extraction, to detach synechia from the angle, in eyes with minimal to moderate optic nerve damage.
The procedure may be complicated by:
hyphema
fibrinous inflammation and
recurrent synechial closure of the angle
2.4.1.7.3 Acute Angle-Closure (AAC) with plateau iris configuration (See FC VII)
In plateau iris configuration the iris plane is flat and the anterior chamber is not shallow axially. (See above under Staging of Primary Angle-closure).
Medical treatment [II,D]:
Pupillary constriction to pull the peripheral iris centripetally
In plateau iris configuration, a modest pupillary constriction may prevent further angle- closure
– pilocarpine 1%, aceclidine 2%, carbachol 0.75%
– dapiprazole 0.5%
Surgical treatment [I,D]:
Iridotomy is essential to confirm the diagnosis because it eliminates any pupillary block component
Argon Laser Peripheral Iridoplasty (ALPI) stretches the iris and widens the chamber angle149.
“Plateau iris syndrome” refers to a post-laser iridotomy condition in which a patent iridotomy has removed the relative pupillary block, but gonioscopically confirmed angle closure recurs without central shallowing of the anterior chamber. Isolated plateau iris syndrome is rare compared to the plateau configuration, which itself is not common. It usually occurs in a younger age group than pupillary-block angle-closure. The treatment is laser iridoplasty or the long-term use of pilocarpine postoperatively [II,D]. This condition must be considered in the differential diagnosis when the intraocular pressure rises unexpectedly following an adequate peripheral iridectomy procedure for angle-closure glaucoma135.
2.4.1.7.4 Intermittent Angle-Closure (lAC)
Etiology:
Similar but milder clinical manifestations than AAC, it resolves spontaneously.
Pathomechanism: See above Ch. 2.4.1.5
Features:
Signs:
May vary according to amount of iridotrabecular contact of chamber angle and mimic acute angle-closure in a mild form
When not on miotics, pupil is round and reactive
The optic disc rim may show atrophy with an afferent pupillary defect
Symptoms:
Mild, intermittent symptoms of acute angle-closure type
Treatment:
Pupillary constriction, iridotomy, iridoplasty or lens extraction are to be considered according to the main mechanism determining angle occlusion [II,D]

2.4.1.7.5 Chronic Angle-Closure Glaucoma (CACG) (See FC VIII)
Etiology:
Permanent synechial closure of any extent of the chamber angle as confirmed by indentation gonioscopy.
Pathomechanism: See Ch. 2.4.1.5
Features:
Signs:
Peripheral anterior synechiae of any degree at gonioscopy
IOP elevated to a variable degree depending on the extent of iridotrabecular contact, above 21 mmHg
Visual acuity according to functional status (may be normal)
Damage of optic nerve head compatible with glaucoma
Visual field defects “typical” of glaucoma may be present
Superimposed intermittent or acute iridotrabecular contact possible
Symptoms:
Visual disturbances according to functional states.
Usually no pain; sometimes discomfort
Transient “halos” when intermittent closure of the total circumference causes acute IOP elevations
Treatment:
Medical treatment alone is contraindicated as all patients require relief of pupil block by iridotomy, iridectomy or lens extraction [I,D]. If the synechial closure is less than half the circumference, iridectomy/iridotomy may be sufficient.
Since complications of iridotomy are uncommon, its use as the initial procedure is justified in practically every case [I,D].
Argon laser trabeculoplasty is contraindicated as it may increase synechial angle-closure [I,D]. Lens removal may be considered at all stages and can lead to relief of pupil block and sufficient IOP control [II,D].
If IOP cannot be controlled medically after breaking pupil block (with or without lens extraction), a filtering procedure is indicated [II,D].
These eyes are more frequently prone to develop posterior aqueous misdirection and the necessary precautions must be taken when considering surgery.
2.4.1.7.6 Status Post-Acute Angle-closure Attack
Etiology:
Previous episode of acute angle-closure attack
Pathomechanism: See Ch. 2.4.1.5
Features:
Signs:
Patchy iris atrophy Iris torsion/spiralling posterior synechiae
Pupil either poorly reactive or non-reactive
“Glaukomflecken” of the anterior lens surface
Peripheral anterior synechiae on gonioscopy
Endothelial cell count can be decreased
Therapy:
Management according to angle, lens, IOP and disc/visual field. In case of cataract surgery, non dilatable pupil, low endothelial cell count and loose zonules are of concern.

{kind=link}
{kind=link}
{kind=link}
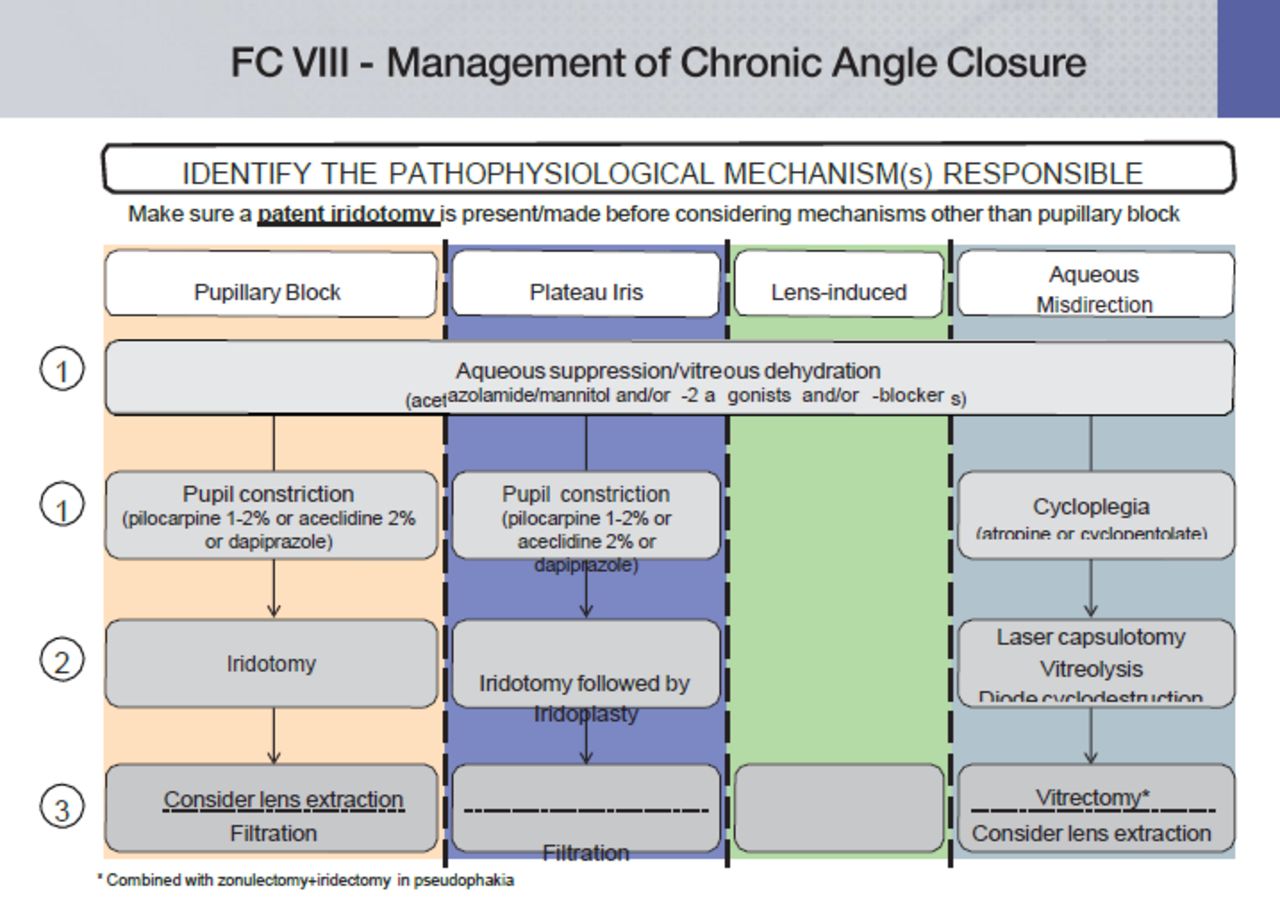{kind=link}
2.5 - Secondary Angle-Closure
There are many different causes of secondary angle-closure and the clinical signs vary according to the underlying condition. For example in secondary acute angle-closure, the chamber angle is closed by iridotrabecular contact that can be reversed, whereas in chronic secondary angle-closure, the angle-closure is irreversible due to peripheral anterior synechiae.
A complete discussion of these topics is outside the scope of this text.
2.5.1 Secondary Angle-Closure With Pupillary Block
Etiology:
The following is a limited list of other etiologies for relative or absolute pupillary block:
Enlarged, swollen lens (cataract, traumatic cataract)
Anterior lens dislocation (trauma, zonular laxity; Weil-Marchesani’s syndrome, Marfans’s syndrome etc.)
Posterior synechiae, seclusion or occlusion of the pupil
Protruding vitreous face or intravitreal silicone oil in aphakia
Microspherophakia
Miotic-induced pupillary block (also the lens moves forward)
IOL-induced pupillary block; anterior chamber IOL, phakic intraocular lens
(PIOL), anteriorly dislocated posterior chamber intraocular lens (PC-IOL)150
Pathomechanism:
Pupillary block pushes the iris forward to occlude the angle. In iritis or iridocyclitis, the development of posterior synechiae may lead to absolute pupillary block with consequent forward bowing of the iris or “iris bombé”. Acute secondary angle-closure glaucoma may result.
Features:
IOP>21 mmHg
Disc features compatible with glaucoma
Treatment:
Several steps may be considered, according to the clinical picture of causative mechanisms [II,D]
Topical and systemic IOP lowering medication
Nd:YAG laser iridotomy
Peripheral surgical iridectomy
Lens extraction, vitrectomy
Discontinuing miotics in miotic-induced pupillary block
Pupillary dilation
Nd:YAG laser synechiolysis of posterior synechiae
2.5.2 Secondary Angle-Closure With Anterior “Pulling” Mechanism Without Pupillary Block
Pathomechanism:
The trabecular meshwork is obstructed by iris tissue or a membrane. The iris and/or a membrane are progressively pulled forward to occlude the angle.
Features:
IOP>21 mmHg
Disc features compatible with glaucoma
2.5.2.1 Neovascular glaucoma
The iridotrabecular fibrovascular membrane is induced by ocular microvascular disease with retinal ischemia; initially the neovascular membrane covers the angle, causing a secondary form of open angle glaucoma (See Ch 2.3 Secondary Open Angle Glaucoma)
Treatment [II,D]:
Topical atropine or equivalent
Topical steroid initially
Topical and systemic IOP lowering medication as needed
Retinal ablation with laser or cryotherapy
Cyclodestruction
Filtering procedure with antimetabolites
Aqueous drainage devices
Miotics are contraindicated
The intravitreal injection of anti-VEGF molecules has shown benefit for this indication [II,C] and is in widespread use.
2.5.2.2 Iridocorneal endothelial syndrome
Iridocorneal Endothelial (ICE) Syndrome, with progressive endothelial membrane formation and progressive iridotrabecular adhesion.
Peripheral anterior synechiae, due to prolonged primary angle-closure; this is theoretically a primary angle-closure.
Treatment [II,D]:
Topical and systemic IOP lowering medications as needed
Filtering procedure, with antimetabolite according to risk factors
Aqueous drainage device
2.5.2.3 Posterior polymorphous dystrophy
Treatment [II,D]:
Topical and systemic IOP lowering medication as needed
Filtering procedure, with antimetabolite according to risk factors
2.5.2.4 Epithelial and fibrous ingrowth after anterior segment surgery or penetrating trauma
Epithelial and fibrous ingrowth after anterior segment surgery or penetrating trauma Inflammatory membrane.
Treatment [II,D]:
Topical and systemic IOP lowering medication as needed
Excision, destruction of the immigrated tissue
Filtering procedure, with antimetabolite according to risk factors
Aqueous drainage device
Cyclodestruction
2.5.2.5 Inflammatory membrane
Treatment [II,D]:
Anti-inflammatory medications and cycloplegics
Topical and systemic IOP lowering medication as needed
Filtering procedure with antimetabolite
Aqueous drainage device
Cyclodestruction
2.5.2.6 Peripheral anterior synechiae after ALT and endothelial membrane covering the trabecular meshwork late after ALT
After argon laser trabeculoplasty (ALT), early and late peripheral anterior synechiae and endothelial membrane covering the trabecular meshwork
Treatment [II,D]:
Topical and systemic IOP lowering medication as needed
Filtering procedure
2.5.2.7 Aniridia
Treatment [II,D]:
Topical and systemic IOP lowering medication as needed
Trabeculotomy
Filtering procedure with antimetabolites
Aqueous drainage device
Cyclodestruction
2.5.3 Secondary Angle-Closure With Posterior ‘Pushing’ Mechanism Without Pupillary Block
2.5.3.1 Aqueous misdirection (also known as cilio-lenticular block, ciliary block or malignant glaucoma)
Etiology:
Angle-closure is caused by the ciliary body and iris rotating forward. Aqueous misdirection, or malignant glaucoma, is a rare type of secondary angle-closure glaucoma most commonly encountered after filtering surgery. The syndrome, also known as ciliary block glaucoma, can occur spontaneously or following any type of intraocular surgery.
Pathomechanism:
The lens may be proportionally abnormally large or swollen, “phacomorphic glaucoma”
Aqueous humour accumulates in the vitreous body (posterior aqueous humour misdirection) or behind and around the crystalline lens (perilenticular misdirection) or behind the iridocapsular diaphragm or posterior chamber intraocular lens (PCL) after extracapsular cataract surgery, with or without PCL implantation, “retrocapsular misdirection”
Frequently precipitated by ocular surgery and flat anterior chamber
Predisposition may be similar in both eyes particularly in small eyes
Treatment:
Medical treatment
Parasympatholytics (atropine, cyclopentolate) both initially and for long-term pupillary dilation and cycloplegia [I,C]
Aqueous production suppressants given orally and/or topically [I,D]
Hyperosmotics (Ch. 3.3.1.3) [I,D] Miotics are contraindicated!
Surgical treatment
A patent iridotomy must be present or, if not present, iridotomy should be performed [I,D]
YAG laser vitreolysis/capsulotomy, especially in aphakia, pseudophakia [II,C]
Anterior vitrectomy, especially in aphakia, pseudophakia [II,C]
Cyclo diode laser
In selected cases lens extraction [II,D]
2.5.3.2 Iris and ciliary body cysts, intraocular tumors
Treatment:
Tumour irradiation or excision
Filtering surgery
Cyclodestruction
2.5.3.3 Silicon oil or other tamponading fluids or gas implanted in the vitreous cavity138
Treatment:
Topical/systemic IOP lowering medications as needed
Silicon oil or gas aspiration
Filtering surgery
Drainage device
Cyclodestruction
2.5.3.4 Uveal effusion151,152
It is due to:
Inflammation as in scleritis, uveitis, HIV infection
Increased choroidal venous pressure as in nanophthalmos, scleral buckling, panretinal photocoagulation, central retinal vein occlusion, arterio-venous communication
Tumor
Treatment:
Anti-inflammatory medication (for 1)
Topical and systemic IOP lowering medication as needed (for 1,2 and 3)
Relaxation of scleral buckling; vitrectomy, sclerectomy in nanophthalmus (for Tumor excision or irradiation (for 3)
Cyclodestruction
2.5.3.5 Retinopathy of prematurity (stage V)
Features:
Signs and Symptoms:
Variable discomfort, pain, redness, corneal oedema IOP ≥ 21 mmHg
Axially shallow anterior chamber
Treatment:
Topical and systemic IOP lowering medications
Cyclodestruction
Filtering procedure with or without antimetabolite
Drainage devices
2.5.3.6 Congenital anomalies that can be associated with secondary glaucoma
These conditions are extremely variable in pathogenesis, clinical presentation and required management; an extensive discussion is outside the scope of this chapter.
Etiology:
Familial iris hypoplasia, anomalous superficial iris vessels, aniridia, Sturge-Weber syndrome, neurofibromatosis, Marfan’s syndrome, Pierre Robin syndrome, homocystinuria, goniodysgenesis, Lowe’s syndrome, microcornea, microspherophakia, rubella, broad thumb syndrome, persistent hyperplastic primary vitreous.
Pathomechanism:
Angle-closure is caused by pushing forward the ciliary body and iris. Increase of volume of the posterior segment of the eye.
Features:
Signs and Symptoms:
IOP> 21 mmHg
Pain, redness, corneal oedema
Axially shallow anterior chamber
Laser iridotomy and surgical iridectomy are not effective
Some differential diagnoses:
Acute IOP elevation with corneal oedema but open-angle may result from Posner Schlossman syndrome (iridocyclitic crisis), or from endothelitis/trabeculitis as in disciform herpetic keratitis.
Neovascular glaucoma may be associated with an open or closed-angle and may mimic some signs and the symptoms of acute angle-closure.
Treatment:
Treatment to be adapted to the primary anomaly, the mechanism of IOP elevation and the quality of life of the patient.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.
- 152.